


1Department of Dermatology and Allergology, University Medical Center Utrecht, 2Pharmerit International, and 3Sanofi & Sanofi Genzyme, Amsterdam, The Netherlands
#These authors contributed equally to this work.
Given the introduction of new therapies targeting specific immune pathways for atopic dermatitis (AD), information on the economic burden of AD patients is needed. Direct costs (medication use and healthcare resource utilization) and costs of productivity loss were studied in 90 adult patients with AD indicated for systemic treatment. Costs were calculated for patients with controlled (Investigator Global Assessment (IGA) 0–2) and uncontrolled (IGA 3–5) disease at inclusion. Mean (95% confidence interval (95% CI)) total direct costs were €5,191 (€4,382–6,019) per patient per year (PPY), €4,401 (€3,695–5,215) for patients with controlled AD vs. €6,993 (€5,552–8,406), mean difference €2,593 (€820–4,282) (p=0.014) for patients with uncontrolled AD. Costs of productivity loss were €10,040 (€6,260–14,012) PPY for the total group, €6,886 (€4,188–10,129) PPY for patients with controlled AD vs. €13,702 (€6,124–22,996) for patients with uncontrolled AD, mean difference €6,816 (–€1,638–16,677; p=0.148). Total costs (direct costs+costs of productivity loss) were €15,231 (€11,487–19,455) PPY for the total group, €11,287 (€7,974–15,436) for patients with controlled AD vs. €20,695 (€14,068–34,564), mean difference €9,408 (–€119–19,964) (p=0.077) for patients with uncontrolled AD. Patients with AD using systemic immunosuppressive treatment incur considerable direct costs and costs of productivity loss.
Key words: atopic dermatitis; systemic treatment; health economics.
Accepted May 9, 2019; E-published May 10, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Lieneke F. M. Ariëns, Department of Dermatology and Allergology, Room G02.124, University Medical Center Utrecht, NL-3508 GA Utrecht, The Netherlands. E-mail: l.f.m.ariens@umcutrecht.nl
Given the introduction of new therapies targeting specific immune pathways for atopic dermatitis, information on the economic burden of patients with atopic dermatitis is needed. In 90 adult patients with atopic dermatitis indicated for systemic treatment, direct costs (including medication use and healthcare resource utilization) and costs due to reduced work productivity were calculated. Total costs (including directs and costs of productivity loss) were €15,231 per patient per year for the total group and €20,695 for patients with uncontrolled disease vs. €11,287 for patients with controlled disease. Costs of productivity loss had the larger impact on total costs. These data indicate that patients with atopic dermatitis using systemic immunosuppressive treatment incur considerable direct costs and costs of productivity loss.
Atopic dermatitis (AD) is a chronic, inflammatory skin disease characterized by intense pruritus and a relapsing and remitting course. With a prevalence of 4.4% among adults in the European Union, AD is one of the most common skin diseases (1, 2). AD has a significant effect on the quality of life (QoL) of patients and their families due to intense pruritus and resulting sleep loss and concentration problems, and its psychosocial impact (3, 4). In addition to the psychosocial burden, AD also has a substantial economic burden caused by costs directly related to treatment (direct costs) including inpatient and outpatient visits, diagnostic tests, transportation costs and medication costs (5). Indirect costs, caused by productivity losses also substantially contribute to the economic burden (4).
Several studies have attempted to quantify the economic burden of AD. However, studies are often difficult to compare as they have focused on variable costs in specific patient populations and used different definitions of direct and indirect costs (4–10). In addition, studies were performed in various healthcare systems across different countries and costs were based on claims or patient-reported data leading to a high risk of recall bias. A recent study using data from the 2013 US National Health and Wellness Survey demonstrated that patients with AD have significantly higher healthcare resource utilization and direct costs compared with non-AD controls (6). Another study performed in the US showed that patients with AD have a significantly higher work absenteeism rate and activity impairment rate compared with non-AD controls (4). This impact of AD on work productivity and activity impairment may lead to substantial indirect medical costs.
During the past decade, the increasing knowledge of the underlying immune pathogenesis of AD has led to the development of new therapies targeting specific immune pathways (11). Dupilumab, a fully human monoclonal antibody targeting the interleukin (IL)-4α receptor, thereby blocking the IL-4 and IL-13 pathway, is the first biologic treatment to be developed. It is approved for the treatment of moderate to severe AD patients, defined as patients who are candidates for systemic treatment including broad immunosuppressive drugs (cyclosporine, azathioprine, methotrexate, and mycophenolate mofetil) and newly developed therapies targeting specific immune pathways (12–14). Given the introduction of these new therapies targeting specific immune pathways for moderate to severe AD, more information on the economic burden and impact on the QoL in the group of AD patients indicated for systemic treatment is needed.
The aim of this study was to investigate the economic burden, including direct and costs of productivity loss, and impact on QoL in patients with moderate to severe AD indicated for systemic treatment in a daily practice setting. In a subgroup analysis, a distinction between patients with controlled vs. patients with uncontrolled AD has been made. The secondary aim of this study was to investigate differences in (economic) burden of patients with controlled and uncontrolled AD.
This observational cohort study included patients who attended the National Expertise Center for Atopic Dermatitis in the University Medical Center Utrecht (UMCU), the Netherlands between January 2016 and September 2017.
This study did not fall under the scope of the Medical Research Involving Human Subjects Act, as confirmed by the local Medical Research Ethics Committee (METC 16/757).
All adult patients with moderate to severe AD defined as patients treated, or starting with systemic treatment, including oral immunosuppressive drugs (cyclosporine A (CsA), methotrexate (MTX), azathioprine (AZA), enteric-coated mycophenolate sodium (EC-MPS) and mycophenolate mofetil (MMF)), visiting the specialized, multidisciplinary, eczema outpatient clinic of UMCU were included. Patients were concomitantly treated with topical corticosteroids and received instructions from a specialized dermatology nurse. AD was diagnosed by a dermatologist, according to commonly used criteria (15, 16). Exclusion criteria were: age below 18 years, treatment with oral immunosuppressive drugs for an indication other than AD and lack of available/essential data from the electronic patient file and/or pharmacist list.
Questionnaires and disease severity measures. Burden of disease and QoL was assessed at the moment of inclusion (baseline) by validated questionnaires including the Skindex-29 (17–19), Patient-Oriented Eczema Measure (POEM) (20), Hospital Anxiety and Depression Scale (HADS) (21) and EuroQoL 5-Dimension 5-Level (EQ-5D-5L) (22). For the HADS questionnaire, the proportion of patients with HADS-anxiety (HADS-A) and HADS-depression (HADS-D) scores of 8 or higher (the cut-off for identifying patients with anxiety or depression) at baseline were reported. The outcomes of the EQ-5D-5L were dichotomized into “no problems” (level 1) and “problems” (levels 2–5). The cut-off scores used to define severely impaired health-related quality of life (HRQL) based on the Skindex were > 44 for the overall score, ≥ 37 for functioning, ≥ 39 for emotions and ≥ 52 for symptoms (19).
Work productivity and activity impairment was measured according to the Work Productivity and Activity Impairment questionnaire (WPAI). The WPAI questionnaire is a validated self-administered instrument to measure impairments in work and activities across 4 domains in the past 7 days; 1: absenteeism or work time missed due to health problem; 2: presenteeism or percentage impairment while working due to health; 3: percentage of overall work impairment (absenteeism + presenteeism); and 4: percentage of activity impairment due to the health problem (23). AD severity was determined at the moment of inclusion by trained healthcare professionals using the Eczema Area and Severity Index (EASI) (15) and Investigator’s Global Assessment (IGA) score (24). Patients were categorized based on their level of disease control at inclusion in patients with controlled (IGA 0–2) and uncontrolled AD (IGA 3–5).
Recourse utilization and (in)direct costs. The numbers of outpatient visits at the dermatology department or other departments in the UMCU, telephone consultations, days of hospitalization and the number of diagnostic and laboratory tests in the year prior to the baseline visit were retrospectively extracted from the electronic patient files. Included patients signed consent to request medication use over the previous year at the patients’ pharmacy. Google Maps was used to determine the geographical distance between the patients’ residence and UMCU.
Yearly direct costs and costs of productivity loss were calculated for the year prior to the baseline visit according to the Dutch guideline for economic evaluations in healthcare (25). Cost analyses were performed from a societal perspective in which all costs available are included, irrespective of who bears those costs or to whom the benefits go. Medication costs were calculated using the Pharmacy Purchase Price, which is published by the Z-index.nl (26). Total medication costs included costs generated by oral immunosuppressive drugs, topical treatment, treatment for other atopic diseases and other AD-related treatment (including antibiotics). Costs for diagnostics and laboratory tests were calculated using the local unit prices.
Direct costs, costs of productivity loss, and total costs were calculated per patient per year (PPY) for the total group and separately for patients with controlled AD (IGA 0–2) and uncontrolled AD (IGA 3–5) at inclusion. Direct costs included costs in the past 12 months related to outpatient visits, hospitalizations, diagnostic and laboratory tests, medication use and parking and transportations costs. Costs of productivity loss included costs due to productivity losses from being absent from work (absenteeism) and being less productive at work (presenteeism). Costs were valued by the human capital approach. Weekly costs due to reduced productivity and missed work time were extrapolated to calculate the yearly lost wages.
All statistical analyses were performed using SPSS statistics 21 (Version 21.0.0.0, SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to describe baseline characteristics and direct costs and costs of productivity loss for the total group of patients. For the subanalysis of patients with controlled and uncontrolled AD, t-tests were used for comparisons of baseline characteristics and healthcare resource utilization between the 2 groups. Pearson’s χ2 test was used for differences of proportions between patients with controlled and uncontrolled AD. A bootstrap method with 1,000 iterations was used to study differences in costs between patients with controlled and uncontrolled AD. A p-value < 0.05 was considered statistically significant.
All costs were calculated per PPY for the total group and for patients with controlled and uncontrolled AD. Prices were adjusted for inflation (September 2018) using the Consumer Price Index (CPI-U) as presented by the Bureau of Labor Statistics. The formulas used to calculate the yearly total costs, direct costs, and costs of productivity loss are shown in Table I.
Table I. Formulas used to calculate the yearly total direct costs and costs of productivity loss
Patient characteristics are shown in Table II. A total of 90 patients indicated for systemic treatment were included for analysis. For the disease control subanalysis, a total of 84 patients were included, of which 51 patients with controlled AD (61%) and 33 with uncontrolled AD (39%). Six patients were excluded from the disease control subanalysis due to missing IGA values. These patients did not differ in baseline characteristics compared with the total group of patients
Table II. Baseline characteristics
Disease severity was measured at the moment of inclusion; i.e., at the point when the patient received or started oral immunosuppressive treatment. Among the total group of patients, the mean ± standard deviation (SD) EASI score at baseline was 9.4 ± 9.1 and the mean POEM at baseline was 12.1 ± 7.3. Out of the 90 patients, 50 (55.6%) patients had received ≥ 2 prior immunosuppressive treatments at baseline.
For the disease control groups, all baseline severity measures were significantly higher among patients with uncontrolled AD compared with patients with controlled AD (Table I).
Out of the 90 patients, 6 (6.8%) reported a baseline HADS-D and 21 (23.3%) a baseline HADS-A subscore of 8 or more, indicating anxiety and/or depression. For the EQ-5D-5L, patients reported “problems” most frequently for the dimensions: usual activity (36 patients (40.9%)), pain and discomfort (68 patients (76.4%)) and anxiety and depression (30 patients (33.7%)). HRQL-based on the Skindex was severely impaired in 26 patients (32.5%) for the overall score, in 52 patients (59.1%) for Symptoms, in 24 patients (27.9%) for Emotions and in 18 patients (20.9%) for Functioning. For the disease control groups, significantly more patients with uncontrolled AD reported a subscore of 8 or more on the HADS-D scale compared with patients with controlled AD (6 (11.8%) vs. 0 patients (0%), p = 0.003). Significantly more patients with uncontrolled AD scored a severely impaired HRQL based on the Skindex for the overall score (51.9% vs. 20.8%, p = 0.039), for emotions (48.4% vs. 18.0%, p = 0.035) and for functioning (38.7% vs. 12.0%, p = 0.048) compared with patients with controlled AD.
Out of the 90 patients, 60 (66.7%) were employed at the moment of inclusion (Table II). Among the employed patients the mean ± SD number of working hours per week was 31.2 ± 15.2. For the employed patients, the mean ± SD reported absenteeism over the past 7 days was 4.7 ± 15.7% and mean reported presenteeism was 21.5 ± 26.4% (Fig. 1). Percentage overall work impairment due to health yielded 23.1 ± 28.2% and the percent activity impairment due to health was 30 ± 27.6%.
Compared with patients with controlled AD, patients with uncontrolled AD reported higher absenteeism (11.1% vs. 0.6%, p = 0.020), presenteeism (32.1% vs. 14.6%, p = 0.015), overall work impairment (33.5% vs. 15.8%, p = 0.024) and activity impairment (38.8% vs. 22.4%, p = 0.006).
Fig. 1. Weekly productivity and activity impairment (mean percent (standard deviation)) in the total group and patients with controlled and uncontrolled atopic dermatitis (AD).
Yearly healthcare resource utilization and associated unit costs are shown in Table III. Compared with patients with controlled AD, patients with uncontrolled AD used significantly more healthcare resources, including the number of visits to a dermatologist (5.5 vs. 4.4, p = 0.028) and days of hospitalization for AD treatment (3.2 vs. 0.9, p = 0.027).
Table III. Healthcare resource utilization and associated unit costs for the total group and patients with controlled and uncontrolled atopic dermatitis (AD) (€)
Mean (95% CI) total costs including direct costs and costs of productivity loss for the total group of patients was €15,231 PPY (€11,487–19,455). There was a trend towards higher mean total costs in patients with uncontrolled AD compared with patients with controlled AD (€20,695 (€14,068–34,564) vs. €11,287 (€7,974–15,436), mean difference €9,408 (–€119–19,964), p = 0.077) (Table IV).
Mean total direct costs (including costs derived from healthcare resource utilization, AD-related medication, diagnostics, laboratory tests and transportation and parking) PPY were estimated at €5,191 (€4,382–6,019) (Table IV).
Mean total direct costs PPY were significantly higher for patients with uncontrolled AD compared with patients with controlled AD (€6,993 (€5,552–8,406) vs. €4,401 (€3,695–5,215), mean difference €2,593 (€820–4,282), p = 0.014). Higher mean total direct costs PPY for patients with uncontrolled AD was mainly caused by significantly higher healthcare resource costs (€3,345 (€2,073–4,807) vs. €1,528 (€1,052–2,125), mean difference €1,817 (€362–3,464), p=0.037) arising from higher healthcare resource use compared with patients with controlled AD.
Costs of productivity loss were extrapolated from weekly costs derived from the WPAI to calculate the yearly lost wages. Costs of productivity loss made up the largest portion of the total costs with an estimated mean of €10,040 (€6,260–14,012) PPY. Costs of productivity loss were higher among patients with uncontrolled AD compared with patients with controlled AD. However, due to the large variance, this difference was not statistically different (€13,702 (€6,124–22,996) vs. €6,886 (4,188–10,129), mean difference €6,816 (–€1,638–16,677), p = 0.148).
Table IV. Direct costs and costs of productivity loss (€) for the total group and patients with controlled and uncontrolled atopic dermatitis (AD)
This study estimated disease burden and direct costs and costs of productivity loss associated with AD in patients with moderate to severe AD indicated for systemic treatment in a real-life Dutch setting. Patients with moderate to severe AD using systemic immunosuppressive treatment incur considerable disease burden and direct costs as well as costs of productivity loss regardless of their level of disease control. Indirect costs due to productivity losses made up the largest portion of the total costs. Total direct costs due to higher resource utilization use were significantly higher in patients with uncontrolled AD compared with patients with controlled AD.
Limited data are available about the economic impact of AD in a well-defined patient population of patients with difficult to treat AD requiring systemic treatment in a real-life setting in the Netherlands. Recently, new therapies targeting specific immune pathways have become available for patients with AD, indicated for systemic treatment. Dupilumab is one of the first biologics that has been developed for AD and has been approved for the treatment of moderate to severe AD, indicated for systemic treatment. Besides dupilumab, other biologics and small molecule therapies are currently under investigation. As the new therapies targeting specific immune pathways will be rather expensive (27), more information on the economic burden of patients indicated for these new drugs is important.
Several studies have attempted to quantify the economic burden of AD. However, costs vary widely and comparing absolute costs across healthcare systems and different countries is difficult (4–10). The economic burden in patients with AD requiring systemic treatment has not been previously described; therefore this study provides new and important data.
Costs due to lost productivity and work absenteeism made up the largest portion of the total costs due to impairments in work and daily activities associated with AD. Reduced work productivity and activity in patients with AD was also demonstrated in a study performed by Eckert et al. (4). In this study, data from the 2013 US National Health and Wellness Survey was used to establish the burden of AD in US adults. Eckert et al. showed that compared with employed matched non-AD controls, employed patients with AD reported significantly higher absenteeism (9.9% vs. 3.6%, p < 0.001), presenteeism (21.1% vs. 16.1%, p = 0.037) and overall work impairment (25.6% vs. 18.1%, p = 0.004). The mean annual costs of productivity loss for employed patients were estimated at $8,907 (vs. $6,517 for non-AD controls, p = 0.024). However, the diagnosis of AD in this study was patient-reported (mainly mild to moderate) and therefore this population is not completely comparable to our population of patients with difficult to treat AD requiring systemic treatment. Nevertheless, the overall conclusions are comparable with the findings of our study indicating substantial impairment in work productivity and absenteeism in patients with AD with associated costs due to lost wages. These findings provide an indication of the potential societal burden of AD due to productivity losses. It is expected that the introduction of new, effective therapies, such as dupilumab, will reduce the burden of the disease and will lower costs caused by the absence from work and reduced productivity while at work (27–30).
This study categorized patients based on their level of disease control (measured with IGA score) in patients with controlled AD and uncontrolled AD. Despite adequate treatment with topical corticosteroids or oral immunosuppressive drugs, 39% of the included patients had an uncontrolled AD at the moment of inclusion, emphasizing the as yet unmet need for safe and effective therapies in patients with difficult to treat AD. Remarkably, patients with controlled AD also had relatively high scores for work productivity and activity impairment measured according to the WPAI and substantial costs of productivity loss as well as direct costs. A possible explanation might be that clinicians often have to search for the optimal oral immunosuppressive drug, which regularly requires a period of trial and error. Therefore, in patients with controlled and uncontrolled AD, frequent consultations are often necessary for monitoring and dose adjustments.
This study has several limitations. Costs of productivity loss were calculated by using scores for work productivity and activity impairment measured according to the WPAI. The WPAI was completed once, at the moment of inclusion, no repeated measurements were available. Weekly costs due to reduced productivity and missed work time were extrapolated to calculate yearly lost wages. The extrapolation of weekly data may have influenced the reliability of the estimated costs of productivity loss. However, the WPAI was completed at different time-points within the inclusion period (between January 2016 and September 2017), which should have minimized the risk of bias due to seasonal influences.
The number of outpatient visits and hospitalization days were available only if they took place in UMCU. There was no data available concerning the number of visits to the physician or other healthcare professionals at other hospitals or clinics. In addition, no data were available addressing out-of-pocket costs for patients (e.g. emollients). The literature shows that AD is associated with considerable out-of-pocket costs for healthcare, which can contribute substantially to total AD-associated costs (7). A US population-based study demonstrated that adults with AD had $371 to $489 higher out-of-pocket costs per person-year compared with patients without AD. The missing data concerning outpatient visits and hospitalization days outside the UMCU and missing out-of-pocket costs in our population may have led to an underestimation of the total AD related costs.
The current study illustrates that patients with moderate to severe AD indicated for systemic immunosuppressive treatment incur considerable direct costs as well as costs of productivity loss, with patients with uncontrolled AD incurring significantly higher direct costs than patients with controlled AD. Costs due to productivity losses were the major cost contributor. In addition, moderate to severe AD presents a substantial burden on QoL among patients indicated for systemic treatment. Further research is needed to study whether the introduction of the new therapies targeting specific immune pathways can reduce the negative impact on quality of life and costs of productivity loss, which may, in part, compensate the expected increase in drug acquisition costs of these new treatments.
The study was financially supported by Sanofi Genzyme/Regeneron.
MdBW: Regeneron Pharmaceuticals, Inc., Sanofi Genzyme – principal investigator, advisory board member, and consultant; AbbVie – principal investigator, advisory board member. MS is an employee of Sanofi. HvO-M has been reimbursed by Sanofi for a study and meeting in AD care. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize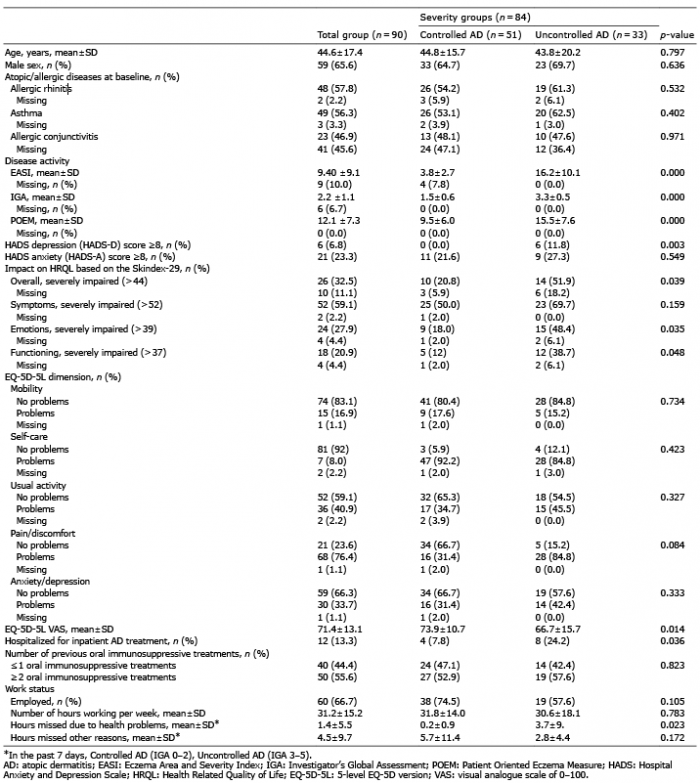 Click to show fullsize
Click to show fullsize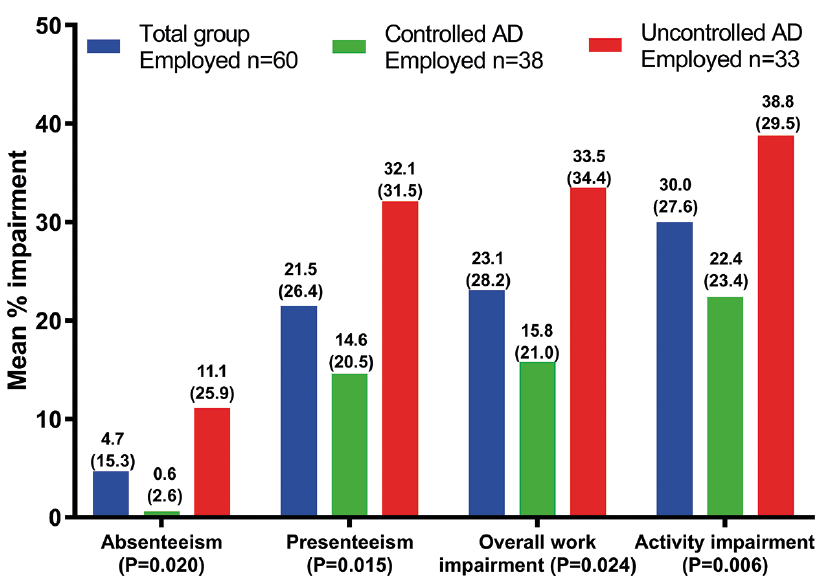 Click to show fullsize
Click to show fullsize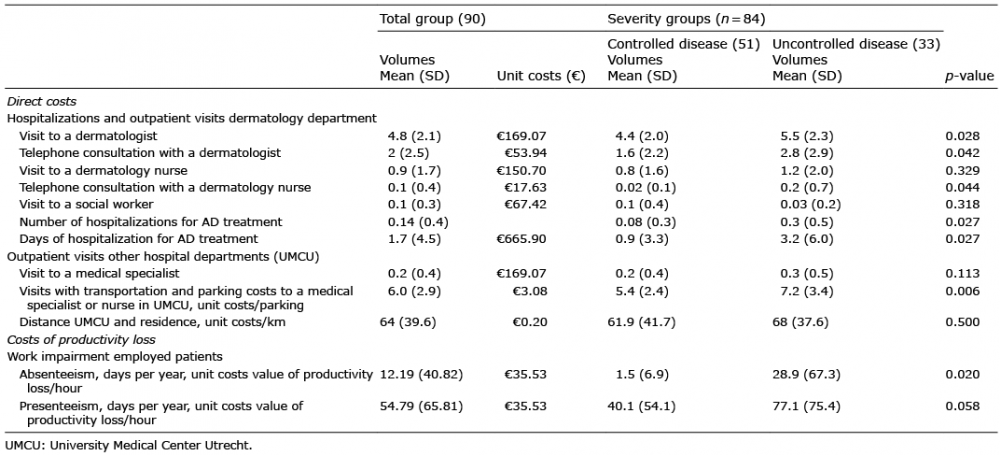 Click to show fullsize
Click to show fullsize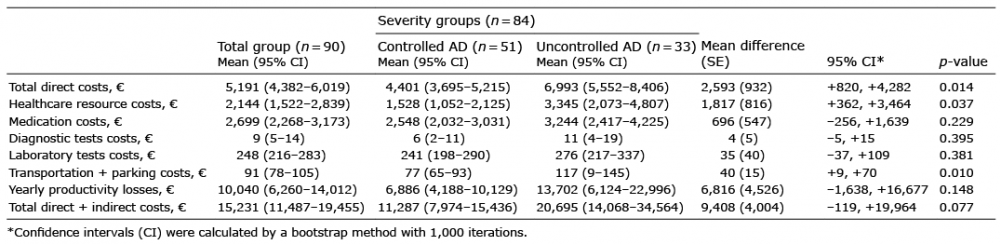 Click to show fullsize
Click to show fullsize