


1SILAB Inc., East Brunswick, NJ, USA, 2SILAB, R&D Department, Brive, and 3Clinreal Online, Toulouse, France
Atopic dermatitis is a chronic relapsing inflammatory skin disease that affects 15–20% of children and 2–10% of adults worldwide. Topical treatments include corticosteroids and calcineurin inhibitors, despite frequently observed adverse events, such as skin atrophy, itching and burning sensations. Alternative treatments that can prolong disease relief between flare-ups are therefore needed. A randomized, single-blind, placebo-controlled, multicentre clinical trial was conducted in a cohort of 90 Caucasian children and 144 adults with mild-to-moderate atopic dermatitis. Tested products were applied twice daily for 60 days. A natural active ingredient from Ophiopogon japonicus, which improves atopic dermatitis symptoms in vivo, was successful in reducing SCORing of Atopic Dermatitis (SCORAD), including erythema, pruritus and body surface area, in both cohorts. The active ingredient also improved patient’s quality of life and significantly reduced the number of patients relapsing compared with placebo. In conclusion, this treatment could be effective to help control mild-to-moderate atopic dermatitis between flare-ups.
Key words: atopic dermatitis; SCORAD; quality of life; relief; Ophiopogon japonicus; clinical trial; oligofructans.
Accepted May 22, 2019; E-published May 23, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Carine Mainzer, SILAB Inc., One Tower Center Boulevard, Suite 2203, East Brunswick, NJ 08816, USA. Email: scientificom@silab.fr
Atopic dermatitis is a common inflammatory skin disease that affects both children and adults worldwide. Topical corticosteroids are regularly used to treat these patients, despite frequently observed adverse events. Alternative treat-ments that can prolong disease relief between flare-ups are therefore needed. This study found that oligofructans derived from Ophiopogon japonicus improved atopic symptoms and patient’s quality of life, and restored skin barrier components known to be reduced in this disease. This active ingredient could be used together with a moisturizing treatment to prolong patients’ remission phase.
Atopic dermatitis (AD) is a common skin inflammatory disease that affects 15–20% of children and 2–10% of adults in industrialized countries worldwide. AD can occur at different stages of life, but is mostly prevalent in children before the age of 6 years (1–3). AD is characterized by a breach in the skin barrier, which is weaker in individuals with AD due to lack of essential structural components (stratum corneum lipids and structural proteins), along with a heterogeneous immune response that can vary from type-1 to type-2/17/22 depending on the subtype of the disease (4, 5). Genetic predispositions (loss-of-function variants in the FLG gene), endogenous factors (e.g. psychological stress) and exogenous factors (e.g. pollution, allergens and irritants, hygiene practices) can trigger AD (6–9).
Clinically, AD is identified by the presence of erythema, oedema/papulation, oozing and crusting, excoriation, lichenification, and skin dryness, along with pruritus and sleep loss (10). These objective and subjective parameters define the SCORing of Atopic Dermatitis (SCORAD), which helps quantify the intensity and severity of this chronically relapsing disease. Moreover, AD can affect large body surface areas, especially in children, and thus greatly affects the quality of life (QoL) of both the patient and their family (11, 12).
AD is often treated using topical corticosteroids (TCS) and topical calcineurin inhibitors (TCI), which help to reduce inflammation. However, these widely prescribed and effective treatments are often linked with adverse events, such as skin atrophy, striae and telangiectasia, systemic absorption (for TCS) or stinging and burning sensations (for TCI) (10, 13) and do not address repair of the skin barrier. Moisturizers are used to hydrate the skin with some proven efficacy in terms of barrier repair (14), but are not helpful enough to promote long-term relief. Herbal medicine, including plants derived from the Chinese tradition, is also widely used to treat AD, particularly among patients seeking natural alternative treatments (15). Herbal medicine, which contains blends of different herbs, have been shown to be effective in the treatment of oxidation, inflammation, allergy and microbes present in AD (15, 16), but must be used with care to avoid any adverse events (17).
Ophiopogon (O.) japonicus, a plant used in traditional Chinese medicine (TCM) has been shown to correct the Th1/Th2 imbalance in mice models mimicking AD features (18), but has not been studied in humans.
The aim of this study was to examine the effect of O. japonicus, which was processed to extract specific active molecules, identified as oligofructans (OF) (AD-RESYL®, SILAB, Brive, France), on decreasing the frequency and intensity of AD flare-ups in Caucasian children and Caucasian adults with atopic skin. The mode of action of OF, derived from O. japonicus, was examined in vivo using a previously established molecular signature of AD (19), before studying its efficacy in Caucasian children and Caucasian adults with mild-to-moderate AD in a randomized, single-blind, placebo-controlled, multicentre clinical trial.
This randomized, single-blind, placebo-controlled clinical trial was conducted in Poland and outsourced to Clinreal Online (Toulouse, France) under the supervision of Bernard Chadoutaud who coordinated the study in collaboration with 12 dermatologists who evaluated in their private practice the efficacy and safety of the natural active obtained from O. japonicus, in slowing down the recurrence of mild-to-moderate AD in 90 children and 144 adults.
Patients were randomly assigned to apply either the active compound or a placebo twice daily over the whole body for a period of 60 days. Patients also received a body hygiene product in its marketed form (Pediatril Cleansing Foam, Laboratoires Dermatologiques Avène, Boulogne-Billancourt, France) to be used at least once a day. The use of topical steroids, immune-suppressors and antibiotics was prohibited during the entire time of the study. Patients were examined on day 0 (D0), day 30 (D30) and day 60 (D60). Tolerance and safety were assessed according to the reported incidence of adverse events and by physical examination. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the institutional review board of SILAB.
Patients were in the age range 4 months to 4 years old (children) and 17–76 years old (adults), with mild-to-moderate AD, defined as SCORAD < 40. Enrolled patients had the classical form of AD over their whole body or some body parts, with flares at least once every 2 months, and with no excessive infection or other dermatological disorder (i.e. prurigo form or nummular form), as assessed by dermatologists involved in the study. To be included in the study, patients had to have undergone relief from AD rashes, (namely the sum of the following criteria: erythema, oedema/papulation, oozing/crusting, excoriation, pruritus, had to be close to zero) 10 days after treatment with TCS (Table SI). Patients treated systemically with corticosteroids/ antibiotics/ immuno-suppressors or having used topical dermocorticoids/ antibiotics/ antihistamines or calcineurin inhibiting type immunosuppressors within the preceding 3 weeks were excluded. Patients with superinfected AD or presenting other dermatological disorders or a chronic or advancing disease were also excluded. Additionally, for the children cohort, patients with antihistamines treatment were excluded except for children chronically treated with antihistamines for asthma or allergic rhinitis; whereas for the adult cohort, patients had to have no history of an allergy or hypersensitivity reaction to a cosmetic product or for an ingredient of the product supplied for the test. Two children, aged 5.1 and 5.2 years, were included in the study despite being above the age limit, with no consequence on interpretation of the results. All patients provided written informed consent before inclusion. For the children (figures in black in Fig. S1), the first patient was screened on 20 March 2014 and the entire study was concluded on 9 July 2014; whereas for the adult group (red in Fig. S1), the first patient was screened on 29 October 2015 and the entire study was concluded on 10 February 2016 (Fig. S1).
Diprobase® cream (Schering-Plough, Kenilworth, NJ, USA) was used as the placebo. For the active treatment, the active ingredient derived from O. japonicus was included in Dipobrase® cream at 0.5% (V/V).
The primary efficacy variable was the change in AD clinical severity index (SCORAD) from baseline to D60. SCORAD combines objective assessments of the extent of body surface area involvement in AD, the severity of erythema, oedema/papulation, oozing and crusting, excoriation, lichenification, and skin dryness, with subjective measures, such as pruritus and sleep loss. Secondary efficacy end-points included the QoL of subjects: Infant’s Dermatitis Quality of Life index (IDQOL) and Dermatology Life Quality Index (DLQI), and of families with children with AD (Dermatitis Family Impact (DFI)) (11, 20, 21). The percentage of patients relapsing was examined throughout the study and the mean time to relapse was assessed. Flare-ups of AD were assessed by investigators at D60. Five questions were answered, including “the treatment reduces the severity/intensity of AD flares” and “the treatment reduces the frequency of AD flares”, with answer scaled from 1 to 4 (1 = strongly agree, 2 = agree, 3 = disagree, 4 = strongly disagree) or without opinion. Improvement in the intensity and frequency of AD flare-ups was considered when questionnaire answers were close to 1. Data are presented as means ± standard errors of the mean (SEM).
The skin of 27 adult atopic patients included in this study (14 for the placebo arm, 13 for the active arm) was analysed at D0 and D60 using an in vivo confocal Raman microspectroscopy. Raman experiments were carried out using an in vivo confocal Raman flexible microprobe (Horiba Jobin Yvon, Villeneuve d’Ascq, France) enabling measurement of each body part. The probe is equipped with a 660-nm Nd-YLF, 25 mW, pumped diode laser source. A long focal microscope objective MPlan FLN 100X/NA 0.75 WD 4.7 (Leica, Mannheim, Germany) (3-μm in-depth resolution) was coupled to a piezoelectric system, allowing “z” movement of 100 μm with adjustable increment. The collected signal was filtered through an edge filter and dispersed with a 3 cm−1 spectral resolution using an 830 grooves/mm holographic grating.
Two different points were analysed for each subject. For each analysed point, Raman profiles were acquired at depths from 0 to 40 μm in 3-μm steps. Spectral data pre-processing was performed with Matlab® 7.2 (MathWorks, Natick, MA, USA). Selected profiles, with good signal-to-noise ratio, were submitted to a succession of corrections included specific correction of the optical signal, smoothing by a Savitzky-Golay algorithm (9 points, second order), baseline correction (polynomial third order). The axial offset position of the Raman profiles was then corrected; and finally, the area under the curve on all the spectral range of Raman spectra was normalized to 1. Spectral data analysis was focused on the stratum corneum layer (22), then compared between healthy and atopic skin.
Statistical tests included the Mann–Whitney U test for inter-group analysis and the Wilcoxon test for intra-group analysis. The number of patients included in both treatment arms of the study (n = 42 and n = 43 for children; n = 68 and n = 71 for adults) justifies the choice of non-parametric tests to analyse statistical differences between treatment arms and within treatment arms at several time-points. The statistical significance threshold was 0.05.
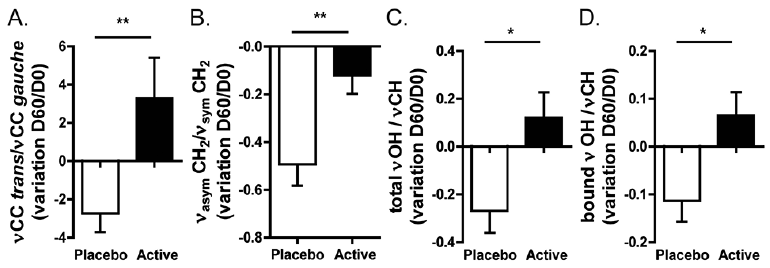
This study examined the mechanism of action of OF extracted from O. japonicus (themed hereafter as the “active treatment”) on a previously identified molecular signature of AD highlighted through in vivo confocal Raman microspectroscopy (19). When the active treatment was applied topically to the skin of atopic patients, an improvement in skin lipid conformation and organization (increase in the proportion of trans and asymmetrical chains, respectively) was observed compared with placebo, which depicted a prevalence of gauche and symmetrical chains (Fig. 1A–B, p < 0.01). Active treatment also improved the total and bound water, as depicted by a respective increase in the total νOH /νCH and in the bound νOH/νCH ratios compared with placebo (Fig. 1C–D, p < 0.05).
Together, these results show significant efficacy of OF from O. japonicus on the molecular signature of AD.
Fig. 1. Efficacy of topical treatment with oligofructans (OF) from Ophiopogon japonicus on atopic dermatitis (AD) hallmarks in vivo. Analysis of the effect of treatment on: (A) epidermal lipids conformation, (B) epidermal lipids organization, and (C–D) water content through in vivo confocal Raman microspectroscopy. *p < 0.05, **p < 0.01.
The study then investigated the efficacy of the active treatment derived from O. japonicus in decreasing the frequency and intensity of flare-ups of AD during a clinical study conducted on children and adults with mild-to-moderate AD.
Enrolment and characteristics of the patients are shown in Fig. S1. A total of 104 children and 150 adults were assessed for eligibility in the children and adult groups, respectively. Of these, 90 and 144 patients were randomized 1:1 to active or placebo arms. The demographic and clinical characteristics of the patients at baseline were similar between each intervention group (Table SI). Throughout the study, 64 patients presented protocol violation (lost to follow-up, lack of efficacy, discontinuation of product usage) (Fig. S1). For the children group, 42 patients in the active arm and 43 patients in the placebo arm completed treatment and reached the primary end-point (D30); 35 patients in the active arm and 33 patients in the placebo arm remained in the study until completion at D60 (Fig. S1). For the adult group, 68 patients in the active arm and 71 in the placebo arm completed treatment and reached the primary end-point (D30); 64 patients in the active arm and 65 patients in the placebo arm remained in the study until completion at D60 (Fig. S1).
SCORAD. In both age groups, the mean ± standard deviation (SD) SCORAD was decreased by the active treatment at D60 (4.0 ± 1.3 children, p = 0.015; 6.6 ± 1.1 adults, p < 0.0001) compared with baseline (5.8 ± 5.1 children, 13.7 ± 0.8 adults) (Fig. 2A/B). This effect was already seen at D30 for the adult group (10.0 ± 1.2 adults, p = 0.0004). The placebo had no effect on the mean SCORAD in the children group, whereas it decreased the mean SCORAD in the adult group at D60 (8.5 ± 1.3, p = 0.0005) compared with baseline (13.3 ± 0.8) (Fig. 2A/B). No significant difference was observed between active and placebo arms at D30 and D60 in both age groups.
Improvements were also noticed in 3 of the SCORAD items (body surface area (BSA), erythema, and pruritus) judged as relevant criteria to highlight active efficacy. In the children group, the mean BSA decreased throughout the study under active treatment (0.3 ± 0.1 at D60 compared with 0.7 ± 0.2 at baseline) and was significantly lower than placebo at D60 (0.3 ± 0.1 vs. 1.0 ± 0.3, p = 0.02) (Fig. 2C). Similar observations were made for mean erythema (0.1 ± 0.1 vs. 0.5 ± 0.1, p = 0.01) and pruritus (0.5 ± 0.2 vs. 1.2 ± 0.3, p = 0.04) with the active treatment significantly improving these criteria compared with placebo at D60 (Fig. 2C). The active treatment was also effective in significantly improving erythema at D30 and pruritus at D30 and D60, respectively, compared with baseline (p < 0.01). Conversely, the placebo significantly failed in maintaining low erythema and pruritus levels at D30 and D60, compared with baseline (p < 0.001).
In the adult group, both active treatment and placebo improved the mean BSA, erythema and pruritus at D30 and D60 compared with baseline (p < 0.05, Fig. 2D). Although no statistical differences were observed between active treatment and placebo arms at D30 and D60 (apart from D60, where the active treatment significantly improved pruritus compared with placebo, 0.6 ± 0.1 vs. 1.4 ± 0.3, p = 0.02), we noticed that the active treatment induced a 1.4- to 1.6-fold higher improvement on these parameters than did placebo.
Fig. 2. Evaluation of treatment efficacy on SCORing Atopic Dermatitis (SCORAD) and related parameters in children and adults with mild-to-moderate atopic dermatitis. Mean SCORAD, body surface area (BSA), erythema and pruritus were evaluated under 60 days’ active (solid line with squares) and placebo (dotted line with circles) treatments in (A, C) children and (B, D) adults. Black asterisks next to each curve indicate significant change from baseline for each arm. Black asterisks at the bottom indicate differences between active and placebo arm. ns: non-significant, *p < 0.05, **p < 0.01, ***p < 0.001.
Quality of life. QoL was assessed with the IDQOL and DFI indexes for the children group and DLQI for the adult group. Although no significant differences were identified between active treatment and placebo arms on IDQOL, DFI and DLQI throughout the study, significant improvements in QoL were demonstrated under active treatment, compared with baseline (Fig. 3).
The active treatment significantly improved children’s and parent’s QoL, as depicted by a decrease in IDQOL and DFI at D30 (2.3 ± 0.3 IDQOL, p = 0.009) and D60 (1.6 ± 0.4 IDQOL, 1.7 ± 0.4 DFI, p < 0.01) compared with baseline (4.3 ± 0.7 IDQOL, 4.0 ± 0.8 DFI) (Fig. 3A/B). The placebo did not improve the QoL of children with AD; however, parents reported improvement in their family’s QoL at D60 with placebo (2.1 ± 0.5, p = 0.03) compared with baseline (3.4 ± 0.7) (Fig. 3A/B).
In the adult group, both active and placebo were reported as significantly improving QoL at both D30 (4.3 ± 0.6 active, 4.4 ± 0.7 placebo) and D60 (2.4 ± 0.4 active, 2.8 ± 0.5 placebo) compared with baseline (7.8 ± 0.9 active, 7.8 ± 0.7 placebo, p < 0.001) (Fig. 3C).
Fig. 3. Evaluation of treatment efficacy on quality of life parameters in children and adults with mild-to-moderate atopic dermatitis. (A) Infant’s Dermatitis Quality of Life index (IDQOL) and (B) Dermatitis Family Impact (DFI) were assessed in treated children, while (C) Dermatology Life Quality Index (DLQI) was assessed in treated adults at D0/30/60. Solid lines with squares: active arm; dotted lines with circles: placebo arm. ns: non-significant, *p < 0.05, **p < 0.01, ***p < 0.001.
Flare-ups and relapses of atopic dermatitis. The intensity and frequency of flare-ups of AD were evaluated by investigators at D60 in both age groups. Active treatment was considered to reduce both parameters in children compared with placebo (1.1 ± 0.1 active, 1.5 ± 0.1 placebo for flare-up intensity; 1.1 ± 0.1 active, 1.4 ± 0.1 placebo for flare-up frequency, p < 0.05), whereas no differences could be detected between both treatments in adults (1.2 ± 0.1 active, 1.3 ± 0.1 placebo for flare-up intensity; 1.2 ± 0.1 active, 1.3 ± 0.1 placebo for flare-up frequency).
Moreover, in both age groups, the number of patients relapsing was 1.9-fold lower in the active arm compared with placebo (Table I). Interestingly, it appeared that patient’s mean SCORAD at the time of relapse was lower under active treatment compared with placebo, although it did not reach statistical significance (14.9 ± 4.1 active vs. 15.9 ± 3.1 placebo, children group; 20.4 ± 3.6 active vs. 27.5 ± 3.4 placebo, adult group).
Table I. Evaluation of the percent and time to relapse in patients
Tolerance and safety were assessed in 85 children (42 in the active arm and 43 in the placebo arm) and 139 adults (68 in the active arm and 71 in the placebo arm) participating in the study. Overall, tested products were well tolerated. The number of adverse events was similar between treatment arms and within age groups. Four adverse events (children: 1/42 for the active arm; adults: 2/68 for the active arm and 1/71 for the placebo arm) were identified but considered as mild in severity. Three of these events (erythema and pruritus) were judged to be possibly related to active or placebo treatments. One of these events, which occurred in the adult group, was not related to the active treatment and was attributed to food allergy.
This study demonstrated the efficacy of a natural active from O. japonicus in reducing AD severity and frequency in both children and adults with mild-to-moderate AD.
No clinical trials of the active treatment in humans have been reported previously. One study used a herbal formula from TCM containing O. japonicus in mice models with house dust mite-induced AD (18), which differs from human AD (23). Studies of the efficacy of natural extracts on atopic children (14, 24, 25), have mostly been carried out in children, since they are more prone to AD than adults. The current study aimed to develop an active ingredient that could help both children and adults with mild-to-moderate AD. To evaluate the long-term relief, active efficacy was assessed during a 2-month period of application, which was considered to be a more relevant time-frame when focusing on the remission phase than shorter periods mentioned elsewhere (14, 24, 25).
AD is thought to be driven by breaching of the skin barrier (26), whereby barrier dysfunction is the trigger for underlying uncontrolled inflammation. The active treatment in this study improved several skin barrier parameters in vivo in atopic patients. Of note, the active treatment restored a compact barrier function through rearrangements in lipid conformation and organization. As a probable consequence of this barrier improvement, the current study also observed water retention in the skin of atopic patients on the active treatment, as evidenced by in vivo confocal Raman microspectroscopy measures and increases in bound and total water. These results provide possible directions regarding the efficacy depicted by the active treatment during the clinical study.
Indeed, the active treatment was found to be effective in providing long-term relief of atopic symptoms in both cohorts, with a better effect on the cohort of children. Interestingly, paediatric and adult AD share a similar pathophysiology, including defects in the barrier function, which are attributed to dysregulated expression and organization in skin barrier lipids and proteins, and high immune responses (19, 27). Nonetheless, paediatric AD displays a reduction in specific lipid-barrier components, which has been correlated with increased transepidermal water loss (TEWL), as well as a larger decrease in tight junction protein claudin-1 compared with adult AD. Immune responses are also differential, with paediatric AD being Th2/Th17/Th22-centred, while adult AD displays Th1/Th2/Th17 inflammation (27). In addition, the current study also found a difference in the extent of AD lesions, which was higher in adults and correlated with higher pruritus compared with children at baseline. These differences might explain the variable efficacy observed for the active treatment in the different age groups.
In the present study, SCORAD index was preferred over the Eczema Area and Severity Index (EASI) score, because SCORAD measures demonstrate a better ability to discriminate between patients who improved and those who did not (28). Moreover, the active treatment presented a favourable safety profile with balanced adverse events and similar discontinuation rates between treatment arms.
Lastly, an aim of this study was to provide a natural solution that would delay the use of TCS, a primary therapy used to treat inflammation in AD (10). Despite their efficacy in reducing flare-ups of AD, TCS are often used in an inappropriate way and patients develop adverse events, such as skin atrophy, striae and telangiectasia or adrenal failure due to systemic absorption. These risks are especially higher in children, whose skin demonstrates a weaker barrier function than in adults, including thinner epidermis, lower surface lipids and natural moisturizing factor (NMF) content and reduced capacities in holding water (29). Thus, improving the remission phase between AD flare-ups would potentially be helpful in reducing the need for corticotherapy. Emollients or moisturizers have demonstrated efficacy in treating AD and reducing relapses (30), mostly by improving skin hydration and reducing TEWL (31). However, this transient effect is not sufficient to provide repair of the barrier function (31), therefore requiring combination with an active substance, as presented here.
To conclude, the study demonstrated the clinical efficacy of a natural active ingredient derived from O. japonicus, which improves patient’s atopic symptoms and QoL in mild-to-moderate AD. This active ingredient restored the molecular signature of AD and, of note, important skin barrier components. The active ingredient could be used in combination with a moisturizing treatment in order to prolong patients’ remission phase.
The authors would like to thank all the patients, dermatologists and investigators who participated in this study and colleagues from SILAB for useful suggestions.
Polish dermatologist investigators: Beata Imko-Walczuk, Adam Wilczek, Lucyna Woliczko, Katarzyna Szmigiel-Michalak, Agata Liebert, Aneta Drozdzewska, Marek Brzewski, Anna Omernik, Maria Brzeska, Dorota Prandecka, Ewa Sieroslawska and Joanna Wantuch-Oszczak.
Funding sources: SILAB.
Conflicts of interest: CM, MLG, RV, SB and BrC are full employees of SILAB. BeC is a full employee of CLINREAL Online.


 Click to show fullsize
Click to show fullsize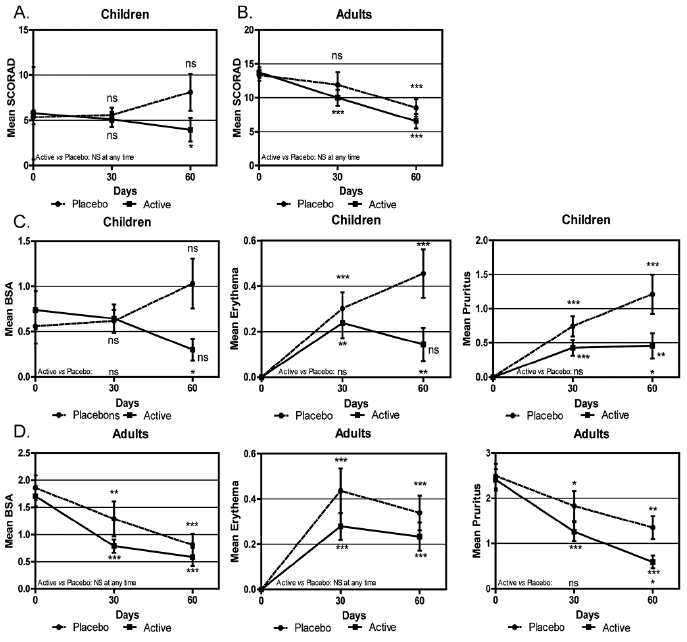 Click to show fullsize
Click to show fullsize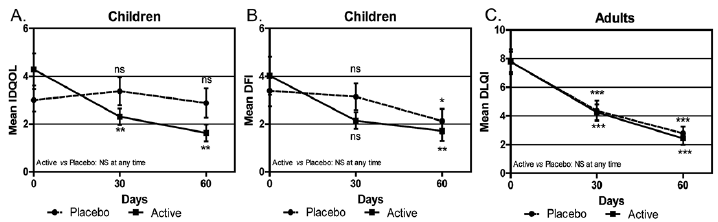 Click to show fullsize
Click to show fullsize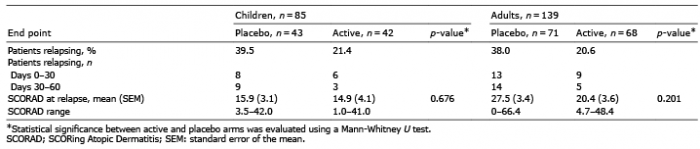 Click to show fullsize
Click to show fullsize