


1Department of Clinical Sciences Malmö, Faculty of Medicine, Lund University, Malmö, 2Clinical Epidemiology and Biostatistics, School of Medical Sciences, Örebro University, Örebro, 3Clinical Epidemiology Division, Department of Medicine, Karolinska University Hospital Solna, Karolinska Institutet, Stockholm, Sweden, 4Department of Epidemiology and Public Health, University College, London, UK, 5Department of Planning and Economics, Region Värmland, Karlstad, 6HTA-Unit CAMTÖ, Örebro University Hospital, Region Örebro County, 7Department of Clinical Sciences Örebro, Faculty of Medicine, Örebro University, Örebro, Sweden
The burden of atopic dermatitis (AD) was assessed. A population-based, cross-sectional questionnaire study was performed among 34,313 Swedish adults in 2017. The prevalence of AD was 14%. Adults with mild AD had an increased relative risk ratio (RRR) of severe depression (aRRR 1.78, 95% confidence interval (95% CI) 1.50–2.12) and anxiety (aRRR 1.97, 95% CI 1.69–2.30), which was higher for severe AD (aRRR 6.22 95% CI 4.60– 8.42, aRRR 5.62 95% CI 4.10–7.71, respectively). Persons with severe AD were less likely to have a university degree (aRRR 0.55, 95% CI 0.34–0.90) and more likely to have a lower annual income (238,000–324,000 SEK: aRRR 0.51, 95% CI 0.39–0.77; 325,000 SEK or more 0.36; 0.25–0.58) compared with individuals without AD. These results suggest that AD implies an increased prevalence of comorbid mental conditions and an adverse impact on academic achievement and work. These adverse associations increase substantially for patients with severe AD and comorbid asthma.
Key words: atopic dermatitis; epidemiology; educational status; global burden of disease.
Accepted Jul 9, 2019; E-published Jul 10, 2019
Acta Derm Venereol 2019; XX: XX–XX.
Corr: Grigorios Theodosiou, Department of Dermatology-Venereology, Skåne University Hospital (SUS), SE-205 02 Malmö, Sweden. E-mail: gregtheodosiou@yahoo.com
In this population-based questionnaire study the burden of atopic dermatitis in terms of mental comorbidity, educational attainment and ability to work was investigated. Among the 34,313 participants the reported prevalence of atopic dermatitis was 14%. Adults with atopic dermatitis had an increased risk for severe depression and anxiety. We report, for the first time that persons with severe atopic dermatitis are less likely to have a university degree and have a lower income compared to persons without atopic dermatitis. Atopic dermatitis is common and has a large impact on patient´s life. Clinicians should be vigilant for increased mental comorbidity.
Atopic dermatitis (AD) is a common inflammatory skin disease. The prevalence of AD is estimated as up to 20% among children and approximately 5% among adults in the industrialized world, although differences occur across countries (1–5). AD causes an itchy rash and dry skin and can have a substantial impact on quality of life (6, 7). AD can lead to substantial financial burden that affects the patients, their families, and society as a whole (8, 9). Furthermore, AD can have a profound impact on mental health and may also have social consequences.
Globally, it has been shown that AD accounts for the largest burden of disability due to skin diseases (9). In a study by Hay et al. (10), the global burden of AD was assessed based on the impact of skin symptoms due to AD (measured as “disability-adjusted life years”; DALY) (9, 10). Knowledge about the burden of AD and risk groups will be an important policy tool for health professionals and decision-makers regarding prevention and treatment of AD in future global health strategies. In Sweden, how-ever, the burden of AD, measured as DALY based on population-based data, is unclear.
There is increasing evidence that AD is not only a skin disease involving epidermal barrier dysfunction, but a complex condition involving broader immune system dysregulation. This might promote systemic inflammation and inflammatory-driven mental health comorbidity, such as depression (11–13). However, other pathways, such as shared risk factors influencing mental health, should be considered. The visible impairment and sleeping problems of patients with AD may also influence their mental health. Mental health comorbidity, in addition to the impact of skin symptoms, might add to the burden of AD (10–21).
AD, especially when severe or poorly controlled, may be associated with psychosocial distress and psychiatric comorbid diseases driven by multiple factors, including disabling pruritus, loss of sleep, social embarrassment, and possible effects on neuromodulators (22, 23).
Recent studies have not revealed any adverse association with educational attainment. A systemic review by von Kobyletzki et al. (24) highlighted the lack of evidence on this subject, and the only study that met the authors’ inclusion criteria could not find an association between AD and educational attainment (24, 25). A recent cohort study including only men in the age range 17–20 years with a current or previous history of AD found an association with lower stress resilience in late adolescence, but no association with lower cognitive function or poorer educational attainment (26). Cultural and lifestyle factors, which might change over time and affect a child’s ability to achieve at school, may explain the differences between different studies. In a study by Sybilski et al. (27) AD was more frequent in individuals with higher maternal education and higher parental income, which might promote successful education of the offspring. However, previous studies contain no data on patients with severe AD (24–27). It is plausible that those with mild AD might not experience an adverse impact of AD on academic attainment.
In patients with severe pruritus, skin pain, extensive skin involvement and the need for a large amount of time for skin treatment, there might be an impact on academic achievement. Comorbid depression might further decrease educational and work performance, potentially via decreased cognitive function (28).
The aim of this study is to assess the prevalence, symptoms and severity of AD. The burden of AD is assessed using the framework of DALY. Also, the association of AD with mental health, educational attainment and occupation in Sweden, as well as social consequences of the disease, are assessed.
A postal survey was conducted during March to June 2017 among a general population-based sample of 78,004 adults 18 years of age and older in 5 Swedish counties (Södermanland, Uppsala, Värmland, Västmanland, and Örebro). The sample was stratified by sex, age, and city (and parts of the city for larger cities). The items in the questionnaire include measures of physical and mental health, education, employment, work environment, and social support. The response rate was approximately 45%. Attrition analyses have been performed and have shown that more women and persons with higher education completed the questionnaire compared with men and persons with lower education. Persons who were older than 49 years were more likely to participate in the survey compared with adults younger than 50 years (29).
The question battery was, whenever possible, derived from international questionnaires. The 5-item World Health Organization Well-Being Index, WHO5, is among the most widely used questionnaires assessing subjective psychological well-being (30).
Exposures and characteristics of interest include AD, and severity of AD, assessed with “Do you have any of the following symptoms or symptoms: eczema, no, yes mild symptoms, yes severe symptoms.”
Health variables. Self-rated health status was derived from “How would you describe your health in general?” on a 4-level scale. Diagnosis of depression was assessed as follows: “Do you have any of the following diagnosed illnesses: depression”. Symptoms anxiety, depressive mood, tiredness, sleep disturbance and stress were assessed using a 3-level scale. Sick leave due to mental ill health was assessed separately for burnout, depression, and stress, each using: “Have you been consistently ill 29 days or longer in the last 12 months?” General mental wellbeing was estimated using the measure WHO5. It was also assessed whether individuals used medication prescriptions of and how many of these.
Educational attainment and occupational status. Current employment was assessed with “What is your current employment?” (employed, self-employed, on parental leave, student, unemployed, retired, on long-term sick leave). The working hours per week were also assessed. Highest educational attainment, occupation, country of birth, sex and age was assessed using data from Statistics Sweden, which were linked to the questionnaire data. The covariates were sex, age groups, highest educational attainment, financial constraints during childhood, and country of birth (Sweden, other Nordic countries, other countries).
DALY. DALY was assessed by combining estimates of the burden of symptoms of AD with the prevalence and severity of AD data in the current study (9). In a previous study, disability index was derived from an analysis of the comparative impact of the direct disabling consequences of AD due to the skin symptoms, mild and severe itch and disfigurement, against other conditions, through a survey that involved the use of international panels of volunteers, a telephone-based survey, and a web-based tool (9). In the previous study, the disability index was combined with the severity distribution of AD, as assessed by experts and based on a literature review to a weighted average disability weight. The prevalence of AD assessed in the current study in combination with the previously developed weighted average disability index was used to determine the DALY of AD in Sweden. DALYs per 100,000 in Sweden in our study was calculated as: DALYs per 100,000=prevalence rate of the current study * weighted average disability weight of the WHO study. For sensitivity analysis, the weighted average disability index based on the severity distribution of our own dataset was used and the prevalence of AD was assessed using data from another Swedish study (31).
All variables were assessed by questionnaire (Appendix S1).
Cross-tabulation and means were used to describe the study population. The association between AD and the outcomes were examined using logistic and multinomial regression, as applicable. In addition to the unadjusted models, the independence of AD and each outcome was assessed by adjustment for covariates based on theoretical considerations. Education, parental financial difficulties during childhood, age, sex, and comorbid asthma were considered as potential confounding factors. Potential confounding factor variables were kept when confounding was evident and were based on theoretically important considerations, such as education. For all objectives the relationship between study outcomes and AD was assessed according to the severity of AD.
Analyses of depression, anxiety, mental, and socioeconomic factors were stratified by sex and a diagnosis of asthma. It was assessed whether sex or asthma were an effect modifier, using multiplicative and additive interaction testing, if applicable, for the relationship of AD and the outcomes. It was assessed whether the effect size for the AD/depression and AD/anxiety relationship increased when the individuals had asthma in addition to AD; this was assessed by calculating the relative excess risk (RERI). For the continuous variable working hours, linear regression analyses were performed and 10-year age group variables were used for adjustment in addition to education and sex.
Additional analysis was performed for the relationship of AD, highest educational outcome and occupation including individuals aged 30 years and older, adjusted for sex, age group, and parental economic situation during childhood. A p-value lower than 0.05 or 95% confidence intervals (95% CI) not including 1.00 was used to indicate statistical significance.
Multinomial regression compares each outcome category with a reference category and produces a RRR by exponentiating the regression coefficients. If there were only 2 categories this would be equivalent to an odds ratio, but as there are more than 2, the statistic is termed a RRR.
The analysis was conducted using Stata MP15 statistical software.
Ethical approval from Uppsala regional ethics committee has been obtained at the regional research ethics committee Uppsala, registration number 2015/417.
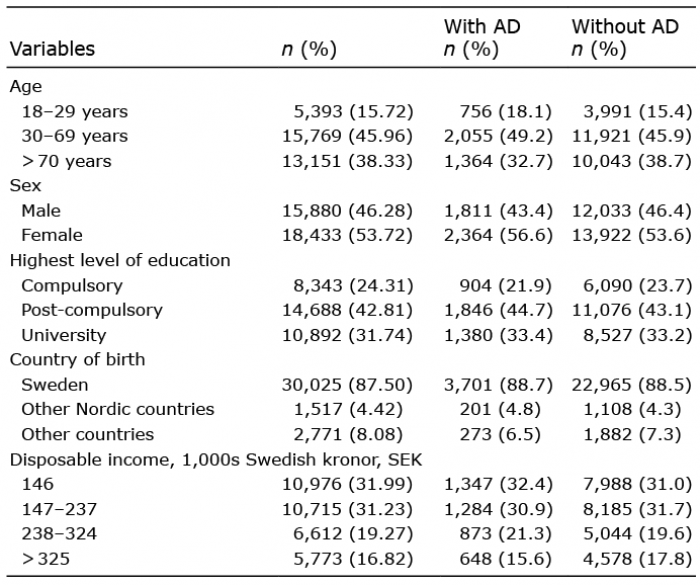
A total of 34,313 answered the questionnaire; 54% females and 46% men. Table I presents the characteristics of the studied population. The median age was 62 years; most individuals were born in Sweden, although being born in other Nordic countries, Asia or other European countries was also common. The total income from both employment and benefits was, for most adults, less than 24,000 Euros per year. The prevalence of AD was 14%, (95% CI 13.5–14.3%) and it decreased with increasing age. Of those with AD, approximately 10% had severe AD. As seen in Table II, the RRR of severe sleeping problems (RRR 1.76) and severe tiredness (RRR 2.62) were increased in adults with AD compared with adults without AD. Adults with severe AD had those conditions in an even higher proportion (RRR 7.90 for severe sleeping problems and RRR 10.18 for severe tiredness, respectively). Adjustment for sex and age group did not considerably alter the relationships.
Table I. Population characteristics of adults with and without atopic dermatitis (AD) diagnosis among 34,313 randomly selected adults in central Sweden
Table II. Atopic dermatitis (AD) and sleep in a cross-sectional random sample of adults in mid-Sweden in crude and adjusted analyses
People with AD, especially with severe AD, were more often never married and they more often felt lonely than adults without AD (aRRR daily loneliness in mild AD 2.04, 95% CI 1.52–2.74, in severe AD aRRR 4.37, 95% CI 2.05–9.33).
DALYs per 100,000 in Sweden are calculated using the prevalence, severity distribution and “disability weight”. We chose not to estimate both the prevalence and the weighted average disability weight based our study results, as this would infer a double impact of the severity distribution and, subsequently, an overestimation of the DALYs calculation. Therefore, we calculated the DALY taking the prevalence and severity distribution of the current study into account and using the standard disability weight, which is used by WHO burden of disease studies (10). This approach revealed a DALY of 526.68 (uncertainty interval 305–826) for the Swedish. The results were compared with an analysis using the prevalence rate of AD from the Swedish part of the population-based study by Svensson et al. (31) and a weighted disability weight, calculated based on the current data, which showed a DALY of 593.67 (uncertainty interval 388–834).
Adults with AD had 30% decreased odds of higher mental wellbeing in analyses adjusted for education, sex and age (OR 0.67 95% CI: 0.63–0.72 for mild AD and OR 0.30 95% CI 0.23-0.38 for those with severe AD. All mental health symptoms and conditions increased in severe AD (Table III). The associations for severe depressive symptoms (aRRR 5.62, 95% CI 4.10–7.71) and severe anxiety (aRRR 6.22, 95% CI 4.60–8.42) were stronger when adjustments were performed for age, sex and highest achieved education.
Table III. Risk of depression and anxiety among adults with atopic dermatitis, presented as relative risk ratios in a sample from mid-Sweden in crude and adjusted analyses
The odds of depression were somewhat higher in men with AD compared with women with AD; and for symptoms of mental conditions, such as anxiety and depressive mood, there were slightly higher odds in women with AD compared with men, but no effect modification by sex was found. Interestingly, the odds of mental symptoms and conditions did not vary across age groups. The odds of diagnosed depression increased for people born in non-Northern countries and was 1.97 (95% CI 1.64–2.31) in adjusted analysis.
For individuals with both AD and asthma, the relationship with both diagnosed depression (OR 1.94, 95% CI 1.25–3.00) and anxiety (OR 2.24, 95% CI 1.93–2.59 for mild disease, OR 6.2, 95% CI 5.05–7.61 for severe anxiety) was of higher magnitude compared with those with AD only. Adjustment for educational status and age group attenuated the relationships for depression (aOR 1.52, 95% CI 1.35–1.72 for mild depression; aOR 3.51, 95% CI 2.87–4.30 for severe depression) and anxiety (aOR for mild disease 1.60, 95% CI 1.48–1.73; and aOR 2.31, 95% CI 1.96–2.72 for severe disease), but the relationships remained. There was an increased excess risk for anxiety (RERI c 0.26, p < 0.001) and depression (RERI c 1.07, p < 0.001) for those having both AD and asthma.
For all persons with AD, crude analysis showed an increased RRR of highschool education and having a university degree; potentially due to socioeconomic advantage during childhood. In adjusted analysis, the magnitude of association was attenuated (Table IV). Persons with severe AD, in both crude and adjusted analysis, were less likely to have a university degree or higher, and had a lower income, compared with persons without AD and with mild to moderate AD. Adults with AD were more often unemployed, and the RRR increased with severe AD. Adults with severe AD were more often on sick leave and more often had a blue-collar occupation. For all results regarding education and occupation, there were no differences for the whole group and for individuals age 30 years and older. Persons with AD were more often working fewer hours (coefficient –0.62, 95% CI –1.13 to 0.12).
Table IV. Association of atopic dermatitis (AD) and socio-economic factors, presented as relative risk ratio (RRR) among adults in mid-Sweden in crude and adjusted analyses
People with AD were more likely to be on sick leave for mental health conditions as well as for stress/burn- out (Table V).
Table V. Association of atopic dermatitis (AD) and mental health in a cross-sectional random sample of adults in mid-Sweden, presented as odds ratios in crude and adjusted analyses
Adults with AD were more often on sick leave for more than 29 days, long-term sick leave/on “activity stimulation” and taking an early pension due to disease, compared with adults without AD (Table IV).
Adults with AD more often had prescribed medication compared with persons without AD and had a higher number of different prescribed medications than persons without AD (Table VI). They had difficulties paying for their medications in a higher percentage, compared with adults without AD. Healthcare utilization increased with severe AD (odds ratio 1.85, 95% CI 1.19–2.90). The results are statistically significant.
Table VI. Atopic dermatitis (AD) and medication in a cross-sectional random sample of adults in mid-Sweden in crude and adjusted analyses
This is one of the few comprehensive population-based studies assessing the prevalence of AD as well as the burden of AD in Sweden with the DALYs measure (32). This large general population-based study showed an adverse effect of AD, particularly when severe, on educational attainment and a negative impact on working performance. Furthermore, there was a substantial impact on mental health, an association with tiredness and sleeping problems and increased healthcare utilization.
This study adds new findings on the relationship between AD and educational attainment, occupational status as well as socioeconomic position. In contrast with the results reported by Ruijsbroek et al. (25), we found that individuals with AD less often had a university degree. Individuals with severe AD less frequently had an income of 238,000 Swedish kronor (SEK) per year, and were more often on sick leave or unemployed, and slightly more often had an occupational status of industrial worker or lower. This study showed, for the first time, that more severe AD reduces the individuals’ socioeconomic position. Furthermore, the current study showed that individuals with AD were more often on sick leave due to stress and burn-out, which is in line with the results of Smirnova et al., reporting a lower ability to cope with stress in individuals with AD (26).
DALY is a population health metric. It is a measure of the overall disease burden, expressed as the sum of years lost due to ill-health, disability or early death on a general population level. The DALYs in our study was high, with approximately 500–600 days lost due to disability per 100,000 persons on a population level in Sweden. This is comparable to diabetes; for example, in Germany and Italy the DALYs due to diabetes were 590 and 580 per 100,000 inhabitants, respectively (33). In line with the current results, a WHO study using the concept of DALYs reported that the leading cause of skin condition causing disability is AD (10). The authors explain that a high value of DALY may be attributed to the high prevalence of AD across countries, in addition to itch, skin pain and disfigurement, and were attributed relatively high disability indexes. The DALYs in our study were even higher compared with the DALYs in Western Europe, as reported by Hay et al. (10), reflecting a high prevalence of AD in Sweden. It has been reported previously that the DALYs can differ when using different data sources. The Global Burden of Disease methodology has limitations, as it depends on what is published plus some hospital figures for attendance where the diagnosis may be suspect when assessing the disability weight. In addition, the estimate of disability weight refers only to what is relevant to the skin symptoms related to AD, i.e. disfigurement and itch. It does not take into account impact on mental health, for instance, as this is recorded under the appropriate mental health diagnosis, e.g. depression.
The dataset used in this study is cross-sectional and does not allow assess of temporality. However, the dataset is large, which allows the assessment of less common outcomes and analysis of subsets of the population. The following facts strengthen the current findings: the magnitude of the association after adjustment for education was high for mental health outcomes and working conditions. All relationships showed a greater magnitude for severe AD compared with mild-to-moderate AD. The findings were consistent across different Swedish counties of birth. The survey comprised large populations and allowed for sub-analysis. The population-based design aimed to minimize selection and ascertainment bias; however, the low response rate might have introduced some selection. Attrition analysis shows that this should not influence the results. Prospective longitudinal studies are needed.
The measurement of disease severity was used previously in population-based studies (29). The self-reported measurement of disease severity was simple, easy to use, and should reflect severity well. In the current study, the question related well to sleeping problems and number of prescriptions. However, this measurement was not validated for AD.
This study showed an adverse effect of AD on educational attainment and work performance. We speculate that it is possible that AD might lead to poor concentration and inadequate sleep, which may cause absenteeism from school or work. Furthermore, the visibility of AD and the accompanying stigma might affect social interactions and school/work performance. Another possible pathway is a potential linkage to attention-deficit hyperactivity disorder (34).
It was found that these adverse consequences increased for individuals with severe AD. Mild short-term pruritus and visible flares might impact less educational attainment compared with frequent and intense signs and symptoms. In addition, inflammation and cytokine response might hypothetically be stronger in patients with severe AD and have a greater impact on mental health compared with in patients with mild AD.
The randomly chosen population-based study allows for generalizability of the study results in similar settings. National data are important for clinicians and decision-makers, but even internationally there are only sparse data. Knowledge of the variability of AD, potential association with mental health and socioeconomic position will add to improving equality. Knowledge of the excess risk of AD and asthma on depression and anxiety adds important knowledge and can be an important policy tool for healthcare professionals and decision-makers, especially for gaining most effect of interventions when resources are limited (27).
From a Swedish perspective, since the prevalence and impact of AD, as well as treatment preferences, can differ across counties, it is important to gain knowledge of AD, and its association with mental comorbidity, impact on education and work, and healthcare utilization on the national level. The impact of AD on labour market participation in Sweden has not been assessed previously in a population-based study.
AD is associated with an increased prevalence of mental conditions and an adverse impact on academic achievement and work. These adverse consequences increase substantially for individuals with severe AD and comorbid asthma. In particular, severe AD is associated with lower socioeconomic position. AD is also associated with high DALY and should be a focus of public health policy and resources. Effective treatment of AD has implications for mental health and social consequences, indicating its relevance to policymakers and healthcare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize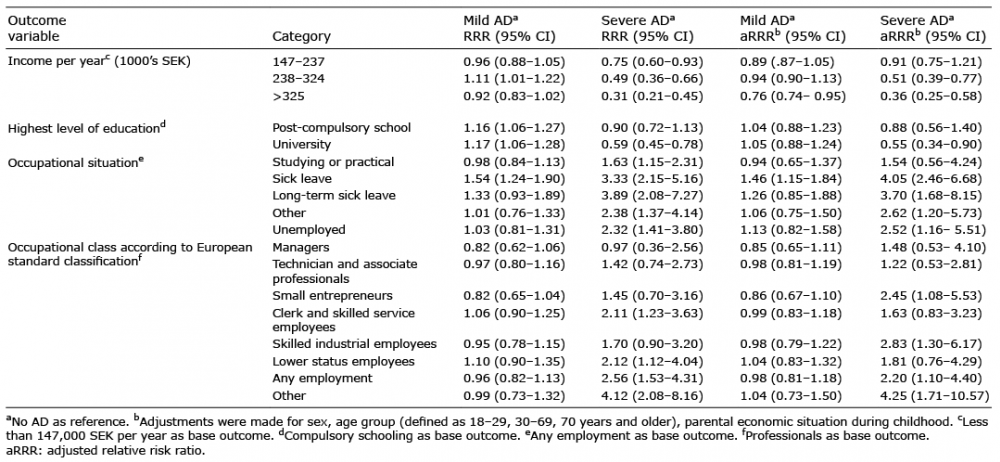 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize