


1University of Tours, 2Department of Dermatology, Unit of Pediatric Dermatology, 6Department of Neuroradiology and Interventional Radiology, CHRU Tours, 3Center of reference for genodermatoses and rare skin diseases (MAGEC), Tours, 4Department of Dermatology and Center of reference for genodermatoses and rare skin diseases (MAGEC), University Paris Descartes – Sorbonne Paris Cité, Institute Imagine, 5Department of Maxillo-Facial Surgery and Stomatology, University Hospital Necker-Enfants Malades, Paris, 7Clinical Investigation Center-INSERM 1415, Tours, and 8INSERM 1246-SPHERE, University of Tours and Nantes, France
#These authors contributed equally and should be considered as first authors.
Managing extracranial arteriovenous malformations is challenging. Sirolimus (rapamycin) is increasingly being used when surgery and embolization are not advised. Because of its anti-angiogenic properties, here we report all extracranial arteriovenous malformation cases treated with sirolimus in 2 French tertiary centers for vascular anomalies. The outcomes were efficacy (complete, partial, no response) based on arteriovenous malformation volume and necrosis/hemorrhage and side effects. We retrospectively included 10 patients (7 children). The sirolimus dose ranged from 0.6 to 3.5 mg/m2. Median (interquartile range [IQR]) treat-ment time was 24.5 (4.5; 35) months. Five patients showed no response, and 5 showed partial response at a median (IQR) of 3 (1; 5) months, followed in 2 cases by therapeutic resistance (i.e., progressive disease after 9 and 24 months of treatment). The most frequent side effect was mouth ulcers. This study shows poor efficacy of sirolimus for treating extracranial arteriovenous malformations.
Key words: vascular anomaly; arteriovenous malformation; sirolimus; rapamycin.
Accepted Aug 6, 2019; E-published Aug 6, 2019
Acta Derm Venereol
Corr: Prof. Annabel Maruani, CHRU Tours, Clocheville Hospital, 9 Boulevard Béranger, FR-37044 Tours, France. E-mail: annabel.maruani@univ-tours.fr
Managing extracranial arteriovenous malformations is challenging. Sirolimus (rapamycin) is increasingly being used in all kinds of vascular anomalies. In this study, we report the largest series of arteriovenous malformations treated with sirolimus, which included 10 patients (7 children). Results suggest a poor efficacy of sirolimus for this condition, with only partial response in 50% of patients, which was transient and lasted several months in 2 of 5 patients, with further worsening.
Extracranial arteriovenous malformations (AVMs) are rare, potentially aggressive, congenital, fast-flow vascular anomalies (1). They are characterized by a red, warm, pulsative swelling, mostly located on the extremities and head and neck and that might be asymptomatic or painful (2). The degree of severity is classified by Schöbinger stages: stage I, quiescent forms; stage II, growing phase; stage III, tissue destruction, ulceration, pain and hemorrhage; and stage IV, cardiac overload (3).
Management of extracranial AVMs is challenging, and we lack guidelines for treatment. The evolution of AVMs is unpredictable, even though trauma and hormonal changes during life are risk factors for rapid aggravation (2). When AVMs are not complicated, the “wait and see” attitude might be relevant. If necessary, therapeutic management results, at best, after multidisciplinary consultations (4, 5), considering arterial embolization alone or followed by radical surgery of the lesion (5, 6). In some cases, embolization and surgical intervention are not possible or are not sufficiently effective, and we lack efficient background drugs.
Sirolimus (rapamycin) is an inhibitor of mammalian target of rapamycin (mTOR), a serine/threonine kinase regulated by phosphoinositide-3-kinase (PI3K) and AKT. Once activated, the PI3K-AKT-mTOR pathway stimulates protein synthesis, cell proliferation and angiogenesis (7, 8). Sirolimus was tried in almost 170 published cases of vascular anomalies, mainly lymphatic and/or venous malformations and also tumors complicated by Kasabach–Merritt phenomenon (9–11). Sirolimus was efficient in most cases. Very few cases of AVMs treated with sirolimus have been reported, with controversial results (9, 10, 12).
In this study, we assessed the efficacy and tolerance of oral sirolimus for extracranial superficial AVMs in children and adults.
Study design and setting
This retrospective, observational study was performed in 2 French tertiary centers for vascular anomalies (university hospitals of Paris-Necker and Tours) and was conducted according to the Declaration of Helsinki ethical guidelines.
Participants
We included data for all children and adults with superficial AVMs in whom treatment with sirolimus was initiated from January 2010 to December 2018. AVM was diagnosed by clinical and MRI signs and by consensus of our multidisciplinary consultations dedicated to vascular anomalies (involving a dermatologist, a radiologist and a surgeon). Imaging criteria for diagnosing AVM included color Doppler ultrasonography showing arteriovenous waveforms and high vascular flow as well as MRI and magnetic resonance angiography, which were systematically performed and allowed for visualizing flow voids without parenchymal staining, enlarged feeding and draining veins and early contrast enhance (13). Sirolimus had been proposed to patients for pain, ulceration or evolution of the AVM and when embolization and/or surgical intervention were not possible or sufficiently effective or not accepted by patients.
Data collected
We collected the following data from clinical records: demogra-phic data, characteristics of the AVM (location, Schöbinger stage, triggering factors for worsening), associated signs, modalities of sirolimus management, previous treatments, and clinical and imaging data on AVM evolution.
Outcomes
Efficacy of treatment was classified by the investigators of each center (RG, AM, OB) as complete response (the condition was considered resolved or almost resolved; i.e. > 90% decrease in AVM volume on clinical and imaging assessments), partial response (> 25% decrease in AVM volume and/or healing of hemorrhage and necrosis) or no response (stabilization, < 25% decrease in AVM volume or worsening). Time to response was collected. Also, the patients subjectively assessed the overall evolution of the AVM on a 5-point Likert scale: 1, major improvement; 2, minimal improvement; 3, stabilization; 4, minor worsening; 5, major worsening. Side effects were collected and classified by the toxicity grading scale, defined as 1, mild; 2, moderate; 3, severe; or 4, potentially life-threatening (14).
Statistical analyses
Continuous variables were described with median (interquartile range [IQR]). Categorical variables are summarized with number (%).
Participants and descriptive data
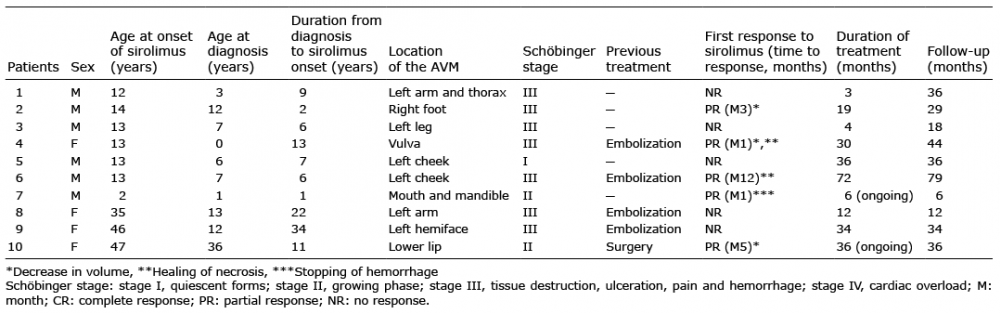
We included 10 patients (7 children, including 6 boys); all 3 adults were women. No patients were excluded from the analysis. Characteristics of patients and AVMs are summarized in Table I. The median (IQR) age at diagnosis was 7 years (2; 12.5). Seven patients had Schöbinger stage III AVM at the time of sirolimus onset. AVMs were located on the face in 5 patients and a limb in 4 and genital organs in 1 patient (Fig. 1). Patient 1 presented a syndromic segmental AVM associated with epidermal nevus syndrome (segmental epidermal nevus, aortic coarctation, and scattered lymphangiectasias). Triggering factors for AVM worsening included puberty in 5 children and pregnancy in 1 adult. Four patients had received arterial embolization and 1 had undergone surgery.
Table I. Characteristics of patients with superficial arteriovenous malformations (AVMs) and response to sirolimus
Fig. 1. Arteriovenous malformations (AVM): clinical features in patients 2 (a, b), patient 4 (c, d) and patient 10 (e, f). a (M2) and b (M10): AVM of the right foot that first showed partial response to sirolimus, then a worsening (increase in volume and necrosis after 9 months’ treatment). c (month [M] 0) and d (M2): AVM of the vulva that showed major improvement after sirolimus (decrease in volume and healing of necrosis). e (M0) and f (M5): AVM of the lower lip that showed minor improvement after sirolimus (slight decrease in volume).
Sirolimus treatment
The median (IQR) age at sirolimus onset was 13.5 (13; 40.5) years. The starting dose of sirolimus ranged from 0.6 to 3.5 mg/m2. For 8 patients, the residual blood level of sirolimus ranged from 5 to 10 ng/ml; for 1 patient, the level was <5 ng/ml (no available data for 1 patient). The median (IQR) treatment time was 24.5 (4.5; 35) months. Two patients were still receiving treatment at last follow-up, after 6 and 36 months of treatment.
Efficacy outcome
Among the 10 patients, none showed complete response (decrease > 90% of volume), 5 partial response and 5 no response (< 25% of decrease of volume). Among patients who showed partial response, 4 were children; AVMs were Schöbinger stage II in 2 patients and stage III in 3. Three of these AVMs were located on the face. The median (IQR) time to response was 3 (1; 5) months (range 1 to 12) (Fig. 2). Patients 2 and 4 experienced a relapse after 9 and 24 months, respectively, characterized by an increase in volume of the AVM and skin necrosis; 1 patient reported major improvement of the AVM on the 5-point Likert scale and 4 minor improvement (Fig. 2). Among the 5 non-responders, AVMs were first stabilized in 3 cases, then showed progressive worsening, and for 2, AVMs immediately became worse.
Fig. 2. Patients’ subjective assessment of efficacy of sirolimus over time on a 5-point Likert scale: 1, major improvement; 2, minor improvement; 3, stabilization; 4, minor worsening; 5, major worsening.
Tolerance outcome
All 7 children experienced side effects (n = 8), graded 1 or 2, which were attributed to sirolimus and consisted of mouth ulcers or oral mucositis (n = 6), acne (n = 1), and transient proteinuria (n = 1). After 18 months of treat-ment, lymphedema developed on the left lower limb in one adult. We found no infections, no cytopenia and no significant biologic anomalies.
Main results
This study of 10 patients suggests that sirolimus is poorly effective for superficial AVMs, with partial response in 50% of patients, which was transient in 2 of the 5 patients. This is the largest series because the condition is very rare.
Limitations
Limitations are linked to the retrospective design of the study: missing data, heterogeneous times to assessment of efficacy, and assessments of efficacy based on radiological and clinical data mentioned in patient records.
Interpretation
Although a therapeutic response to sirolimus was reported for half of the patients, the qualitative responsiveness was low, with partial response only, and considered minor for 4 patients, with heterogeneous time to treatment response. AVMs were treated at advanced stages (≥ stage II in all patients), so these results cannot be extrapolated to patients with early-stage AVM.
To our knowledge, among more than 100 vascular malformations treated with sirolimus reported in the literature, 6 were extracranial AVMs (9, 10, 12, 15). Their characteristics are summarized in Table II. In the 6 cases, efficacy of sirolimus was heterogeneous (partial response in 3 cases, no response in the 3 others). The criteria for assessing efficacy were based on symptoms (pain), physician assessment of the decrease in volume AVM and/or imaging; time to assessment ranged from 1 to 6 months. The starting dosage of sirolimus was close to ours and was homogeneous in the 6 cases (1.6 mg/m2/day); however, the target levels of serum sirolimus were slightly higher in the 3 cases showing partial response. We hypothesize that this slight difference in dosage was not significant and was not responsible for the difference in response to treatment because as in other VMs, target levels of about 5 ng/ml seem efficient (9, 10). The reason for the efficacy of sirolimus in some cases is more probably linked to differences in molecular basis. In all AVMs for which sirolimus seemed efficient, the AVM was associated with phosphatase and tensin homolog (PTEN) hamartoma syndrome. PTEN is a strong inhibitor of the PI3K-AKT-mTOR pathway and its mutation allows for uncontrolled activation of the pathway leading to the development of hamartomas (16). Sirolimus would partially restore control over the pathway.
Table II. Characteristics of patients with arteriovenous malformation (AVM) and response to sirolimus in previous publications
In sporadic AVMs, as in the 10 cases we report, somatic variants of several genes of the renin-angiotensin system–mitogen-activated protein kinase (RAS-MAPK) pathway were recently identified (17, 18). This pathway interacts via RAS with the PI3K-AKT-mTOR pathway; while inhibiting the latter, sirolimus may lead to overactivation of the RAS-MAPK pathway, which explains the clinical worsening we observed. Thus, therapies targeting the RAS-MAPK pathway might have potential for superficial AVMs (18).
Conclusions
Sirolimus was only slightly efficient in half of our patients with AVMs. None of our 10 patients experienced severe side effects. New drugs targeting other pathways need to be developed for this rare and aggressive condition.


 Click to show fullsize
Click to show fullsize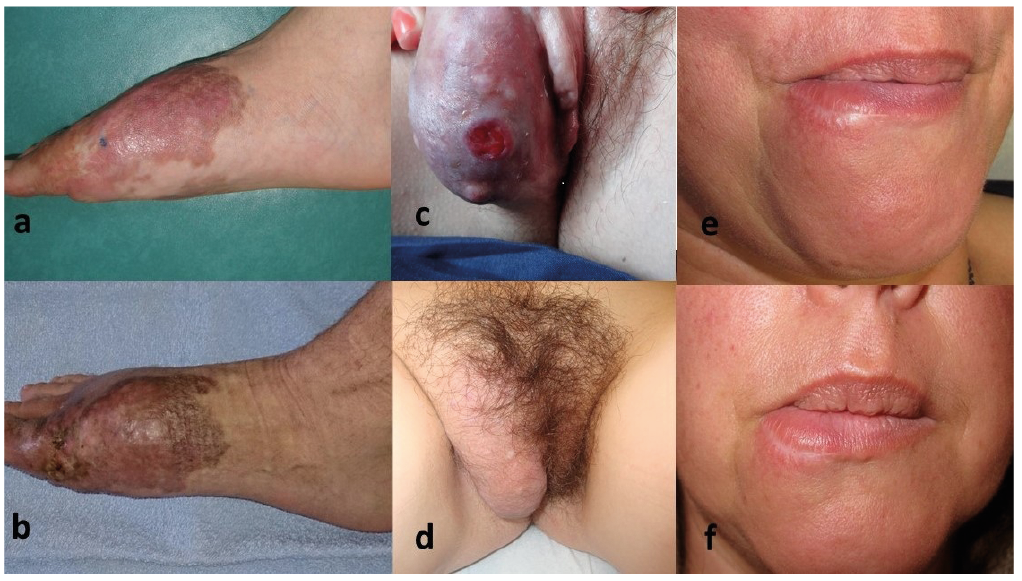 Click to show fullsize
Click to show fullsize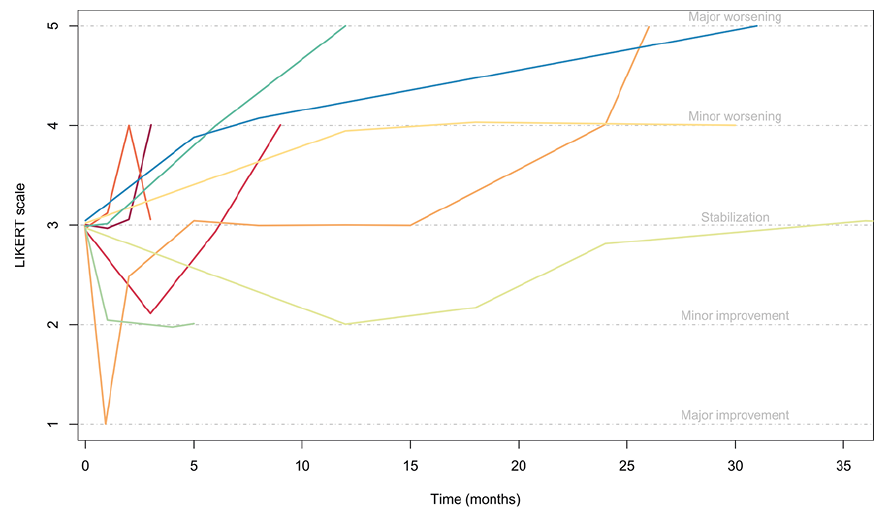 Click to show fullsize
Click to show fullsize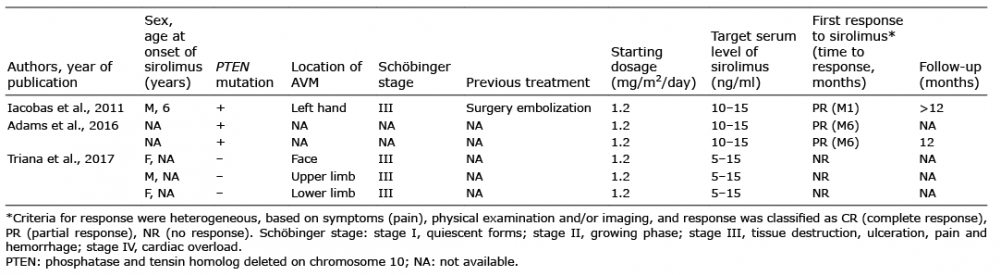 Click to show fullsize
Click to show fullsize