


1Allergy and Asthma Care of Long Island, Rockville Centre, NY, 2Asthma and Allergy Foundation of America, Washington, DC, 3Allergy & Asthma Network, Vienna, VA, 4Flince Research and Design, Brooklyn, NY, 5Insights and Analytics, 6Medical Affairs, 7Health Economics and Outcomes Research and 8Advocacy and Strategic Alliance, Novartis Pharmaceuticals Corporation, East Hanover, NJ, and 9Department of Medicine/Dermatology, University of California Los Angeles, Los Angeles, CA, USA. #Affiliation at the time the study was conducted.
Chronic spontaneous urticaria is challenging to manage and substantially affects quality of life. This US, non-interventional qualitative study examined patients’ clinical journeys and emotional burden from symptom onset through disease management. Chronic spontaneous urticaria patients participated in interviews and completed diaries focusing on disease and treatment history/perspectives, impact on personal/family life, and relationships with physicians/other healthcare providers. Physicians were interviewed about their views on disease management and patient care. Twenty-five patients, previously or currently receiving chronic spontaneous urticaria treatment(s), and 12 physicians participated. Key stages following symptom onset were identified: Crisis (associated with feelings of torment/disorientation/shock); Searching for answers (puzzlement/frustration/anxiety); Diagnosis (relief/satisfaction/fear/isolation); and Disease management (frustration/hope/powerlessness). Findings revealed patients’ perceptions and experiences of chronic spontaneous urticaria, including living with a ‘skinemy’, experiencing their ‘own personal hell’ and feeling ‘like an experiment’. Awareness of unmet needs in patient care/management identified in this study may ultimately improve patient support and enhance physicians’ understanding of disease burden.
Key words: urticaria; hives; quality of life; urticaria psychology; qualitative research.
Accepted Aug 8, 2019; E-published Aug 9, 2019
Acta Derm Venereol
Corr: Dr Stanley Goldstein, Allergy and Asthma Care of Long Island, Suite 401, 242 Merrick Road, Rockville Centre, NY 11570, USA. E-mail:
drsgoldstein@gmail.com
• Chronic spontaneous urticaria has a substantial impact on patients’ quality of life. This study’s findings can help physicians recognize both the emotional and physical burden of chronic spontaneous urticaria.
• Patients’ frustration with time taken to reach diagnosis, and with cycling through different treatments (and some-times clinicians) until treatment success achieved, was commonly experienced. Physicians also experienced frustration with the patient care pathway.
• Greater support and further education are needed for patients and physicians.
• Maintaining open channels of communication and engaging in shared decision-making may benefit the patient–physician relationship, ease frustration and encourage a more collaborative approach to long-term disease management.
Chronic spontaneous urticaria (CSU), formerly known as chronic idiopathic urticaria, is characterized by the spontaneous occurrence of itchy and sometimes painful wheals, which may have a burning sensation, and/or angioedema; and persist for at least 6 weeks without a specific external trigger (1).
CSU is estimated to affect 1.6–3.3 million people in the USA (2, 3). Disease presentation varies, and it is difficult to predict how long a patient may be affected and whether or not they may experience a relapse after remission (2). The duration of the disease is generally 1–5 years but is likely to be longer in more severe cases (2).
The extent to which patients’ quality of life (QoL) can be affected by CSU has been demonstrated in numerous studies (1, 2, 4–8) and goes beyond effects on skin (e.g. itching), with many patients reporting fatigue, pain, and sleep disturbances. Patients also experience a substantial psychological burden; many develop anxiety and depression after diagnosis, which significantly impacts their QoL (6, 7, 9, 10). Patients also report dissatisfaction with their treatment and their relationship with their physician (5, 8, 11). Highlighting the value of the physician acknowledging the emotional element of CSU, one study found that patients whose physician had discussed the emotional impact of the disease with them were significantly more satisfied with their treatment and also more trusting of their physician (8).
CSU also carries a high socioeconomic burden through a combination of direct healthcare costs and indirect costs from loss of work productivity. Patients with CSU experience high levels of work impairment and are frequent users of healthcare resources (4, 6). These observations are supported by the experience of physicians, with many reporting that the time and cost spent on care, plus the frequency of follow-up visits, are above average (12). The physicians in this study also commented that patients with CSU represent a group with a sizeable emotional burden and high expectations, and they found it difficult to satisfy their patients’ needs (12). Although the approach to management of CSU can vary, treatment pathway recommendations do exist. In the 2017 revision and update of the European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European Network/European Dermatology Forum/World Allergy Organization (EAACI/GA²LEN/EDF/WAO) guideline (1), the first recommended line of treatment for CSU is second-generation, non-sedating H1-antihistamines. In cases of inadequate response to first-line treatment, the guideline suggests increasing the dosage up to 4 times the standard dose as a second-line option. In patients who are refractory to the higher dose H1-antihistamines, a third-line treatment option includes omalizumab as an add-on therapy (1, 13, 14). Cyclosporine A is not approved by the Food and Drug Administration (FDA) for urticaria but has shown efficacy in combination with second-generation H1-antihistamines and is recommended in the 2017 EAACI/GA2LEN/EDF/WAO guideline only for patients with severe disease refractory to combination therapy with antihistamine and omalizumab (1).
Consideration of patients’ perspectives is important in the provision of high-quality healthcare and can promote patient–physician shared decision-making (SDM). This qualitative study examined the perspectives and experiences of patients with CSU and identified stages of their journey from symptom onset through diagnosis and disease management. In addition, the study explored the views of physicians who manage patients with CSU. While this study was conducted prior to the publication in 2018 of the 2017 revision of the EAACI/GA2LEN/EDF/WAO guideline, the guideline is referred to here for clinical relevance in current context.
Study objectives
This was a non-interventional, qualitative study conducted in the USA, with the following 5 objectives: (i) To understand patients’ perspectives and experiences of CSU and the challenges they face as they move through the medical system, from diagnosis through treatment and disease management; (ii) to understand how physicians approach the management of patients with CSU and to explore their relationship with patients, from diagnosis through treatment and monitoring; (iii) to examine the relationships between patients and healthcare providers for a better understanding of the degree of SDM in disease treatment and management; (iv) to understand patients’ network of information, support and advice; and (v) to uncover the unmet needs of patients and physicians.
Recruitment and eligibility
Patients were recruited between June and August 2017 with the assistance of two patient advocacy organizations (the Asthma and Allergy Foundation of America, and the Allergy & Asthma Network) and a patient-led CSU support group on Facebook. Market research recruiters identified eligible physicians, using national databases and a series of short questions asked by telephone.
Eligible patients had a formal diagnosis of CSU, were between 18 and 74 years old, were under the care of an allergist, dermatologist, or primary care physician (PCP), and had previously or were currently receiving treatment(s) for CSU. Eligible physicians included allergists and dermatologists who had previous experience managing ≥10 patients with CSU, and of treating with biologics.
Study design and data collection
Data were collected in 3 ways: (i) Semi-structured interviews with patients. Researchers conducted telephone interviews (duration 1.5–2 h) with patients (sample questions are presented in Table SI), based on an interview guide that included an outline of conversation themes, topics and questions. The interview guide was intended as a flexible tool to facilitate patient–researcher conversation yet allow researchers to adapt inquiries to explore insights shared by participants that researchers had not previously contemplated. Interviews were designed to provide the opportunity for patients to discuss the impact of their disease within the context of their personal and family life, as well as talk about their disease history and experiences with treatment. Relationships with their medical team, and the support and available resources for managing their disease, were also covered. (ii) Patient diaries. Patients documented their experiences in a diary comprising 3 sections: ‘Living with CSU’, ‘Your 3-day diary’, and ‘Reflections on CSU’ (Table SII). In the diary, patients submitted written responses to questions, created pictures, and recorded video clips of themselves to document what the disease has meant to them, how it affected them, and their decisions regarding medical support and treatment. Patients also developed a timeline of their personal journey with CSU. (iii) Semi-structured interviews with physicians. Researchers conducted interviews with physicians by telephone (sample questions are presented in Table SIII). Interviews were conducted in a one-to-one setting and lasted 1 h. As with patient interviews, the interview guide was intended as a flexible tool to facilitate conversation and researchers explored additional topics as they arose.
For both patient and physician interviews, researchers documented interactions by taking notes during interviews; these notes were then used to develop descriptive and analytic accounts. Audio recordings of interviews were transcribed.
Data analysis
Researchers analyzed interview notes, audio transcriptions, and patients’ diaries to identify key topic areas and themes. The researchers then interpreted these themes, as well as perceptions, practices, and sociocultural contexts of participants’ experiences, to generate data findings.
Adverse event reporting
All patient and physician interviews, and patient diary submissions, were monitored by the research agency for adverse events. Any adverse events that were raised during the course of the study were reported to Novartis Patient Safety for subsequent submission to the FDA.
Ethics
The study was performed in accordance with the relevant principles of the Declaration of Helsinki, and all participants provided written, informed consent prior to participation. The study was also conducted in accordance with all pertinent privacy laws and regulations, including the Pharmaceutical Marketing Research Group/Insights Association guidelines. To maintain confidentiality, researchers had limited access to respondents’ personal information. Owing to the nature and design of the study, ethical approval by an Institutional Review Board was not required.
Patient participants
In total, 25 patients (19 females and 6 males), aged 23–66 years, took part in the study. All had previously, or were currently, receiving H1/H2-antihistamines. Medications taken by patients were as follows: prednisone (n = 22, 88% of patients); omalizumab (n = 16, 64%); montelukast (n = 13, 52%); doxepin (n = 7, 28%); cyclosporine (n = 6, 24%); sulfasalazine and/or hydroxychloroquine (n = 3, 12%); and dapsone (n = 2, 8%).
Stages of the patient journey
Study findings reveal 4 key stages of the patient journey following symptom onset. The emotional, experiential, and medical considerations relating to each stage of the patient journey are presented in Fig. 1. The 4 stages include:
(i) Crisis
As symptoms appeared on different parts of the body (e.g., arms, legs, back, groin, buttocks, scalp), patients experienced a ‘Crisis’ stage. This was associated with feelings of torment, disorientation and shock. Patients felt as though their life had been interrupted by something that they could not control. They and their families struggled to understand what was happening.
(ii) Searching for answers
The second stage was ‘Searching for answers’ and reflected patients’ frustration and anxiety as they tried to find the cause of their symptoms and made repeat physician visits. Patients analyzed their habits and routines and frequently turned to the Internet for possible causes, further information/education and coping strategies.
(iii) Diagnosis
For some patients, a diagnosis provided a sense of relief and hope, and patients who joined a CSU support group found it helpful to connect with others with the same symptoms and experiences. However, these positive experiences were accompanied by continued anxiety surrounding the prospect of symptom return and difficulty grappling with the concept of idiopathy. The time taken to reach this stage was variable, as was the availability of support for patients.
(iv) Disease management
Following diagnosis, patients entered the ‘Disease management’ stage. As with the Diagnosis stage, patients had a mix of positive and negative experiences. When treatment was effective, they felt relief and hope but this was tempered by anxiety about future symptom breakthrough; when symptoms flared up again, other medications were tried, or alternative specialist physicians were sought. Patients reported experiencing a repetitive pattern of cycling through different treatments and seeing different physicians in their quest for symptom relief.
Fig. 1. A map of the emotional, experiential and medical aspects of the patient journey, from chronic spontaneous urticaria (CSU) symptom onset through disease management. aNot Food and Drug Administration (FDA)-approved for CSU (15–21); bRecommended in the revised 2017 European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European Network/European Dermatology Forum/World Allergy Organization (EAACI/GA2LEN/EDF/WAO) guideline only for patients with severe disease refractory to combination therapy with antihistamine (AH) and omalizumab (1).
Study findings across the different stages revealed patients’ experiences with CSU, which included bewilderment prior to diagnosis, the impact of CSU on their sense of identity, mixed feelings of relief and confusion at diagnosis and the effects on daily life. Sample narratives are presented in Table I.
(i) “What the heck is going on?”
At disease onset, patients were stunned to confront hives and, for some, disfiguring swelling (angioedema). Patients and their families were often frightened and struggled to understand what was happening (“What the heck is going on?”), driving them to self-analyze and attempt to determine disease triggers through a process of eliminating, for example, certain foods from their diet or products from their domestic environment. Patients commonly conducted extensive Internet research on their symptoms, leading them to wonder if they had an allergy, gout, lupus, rheumatoid arthritis or cancer. Attempts to self-medicate were frequent, typically with over-the-counter oral antihistamines or, in some cases, using someone else’s prescription for prednisone.
(ii) “Living with my ‘skinemy’”
Patients expressed the feeling that their bodies were turning against them, becoming an enemy, hence the term ‘skinemy’. Many patients felt exasperated with their body (“I wanted to rip my skin off”) and characterized the itching and swelling as being alive (“It grows, spreads and moves”). Patients used metaphors to express unrelenting symptoms (“It’s like wading in a pile of red ants, with fiberglass and poison ivy”). As symptoms changed over time, patients commonly experienced anxiety and frustration at the unpredictable nature of the disease, and conveyed a sense of helplessness, which remained even after their physical symptoms had improved. This sense of powerlessness was often shared by the partner or spouse of the patient, who felt unable to help or make a difference.
Patients reported feeling a loss of normalcy and identity, and that they were stigmatized socially by others (“People look at you like you’re diseased; you’re contagious”). Reluctance to be seen in public was common. Confronting other people’s curiosity was a painful experience, and some patients tried to hide their symptoms with make-up, growing their hair, or wearing clothes that covered affected areas of their body. Patients often struggled to explain to others what was happening to them and offered simpler explanations, such as saying they had poison ivy or an allergic reaction. Other patients gave up trying to explain to others. For many patients, shame and distress prevented them from actively engaging as parents, partners, professionals and community members.
(iii) Relief and confusion at diagnosis
The time between symptom onset and the patient seeking medical care ranged from several weeks to 2 years. Time to diagnosis after symptom onset was variable. Many patients were diagnosed from 1 week to 6 months after symptom onset, while for other patients, time to diagnosis ranged from 1 week to as much as 15 years, suggesting there may be barriers to reaching a timely diagnosis, such as a lack of disease awareness or intermittent symptoms causing a delayed approach to seeking care. Some patients received a prompt diagnosis with their allergist or dermatologist. Others saw a number of different healthcare providers (e.g., allergist, dermatologist, endocrinologist, general practitioner, rheumatologist) before receiving a confirmed diagnosis.
Patients experienced mixed feelings at diagnosis. Relief and satisfaction at the validation of their disease (“I could finally put a name to what I had”) were common emotional responses. However, some patients found the medical terminology used by their specialist confusing and recalled receiving inadequate information about their disease. Patients perceived education around CSU to be limited and sought educational materials and support online.
Many patients wrestled with the concept of idiopathy, which they found confusing. They felt that, if only a cause could be found, effective treatment would follow, and so continued to search for a cause, believing it was their responsibility to find a reason now that their physician had stopped looking for one. Many questioned whether a disease with no identified cause was in fact a real, legitimate disease.
(iv) “My own personal hell”
Patients often continued to suffer with symptoms after diagnosis. Reduced participation in activities around the home and with childcare meant a patient’s partner/spouse needed to take on additional tasks. Patients also reported decreasing their work hours or changing the amount of time they worked in the public eye. One patient summed up the cumulative impact on her QoL by stating, “I feel like my entire life has been hijacked by CIU; I just want it back”. Mental health issues, such as depression and anxiety, were reported by many patients, some of whom had sought the assistance of counselors, psychologists or psychiatrists. Fatigue was also experienced, attributed by patients to night-time symptoms and sleep challenges.
Support from family and friends varied. Some patients encountered empathy and encouragement, others admitted feeling stress in their relationships, particularly if they felt they were a burden to others. Some found family to be sympathetic initially but that this diminished over time.
Patients described being caught in an ongoing cycle of events relating to their CSU (Fig. 1). They experienced the anxiety of not knowing when their symptoms would flare up, sometimes with a sensation of tingling or heat as a precursor to their urticaria, followed by emotionally taxing hypervigilance (e.g., paying close attention to what they were eating, what their bodies were exposed to and how they were feel-ing). The presence of physical symptoms triggered more anxiety and frustration, leading patients to believe that their suffering could continue indefinitely: “There’s no relief in sight. It feels like it’s never going to end”. During symptom flare-ups, it was common for patients to have a high number of repeat Emergency Room visits. Patients reported changing the specialist physician whom they had been seeing and trying out different treatments/treatment combinations, for which they needed each time to evaluate the potential benefits against the possible side effects. Patients who had been referred to specialists sometimes returned to their PCP in distress when their treatment was considered ineffective and suffering persisted. Patients felt increasingly frustrated and discouraged and began to lose confidence each time they tried a different healthcare provider or alternative treatment. These factors, together with the high costs of medical care, led to patients experiencing healthcare fatigue.
(v) “I feel like an experiment’’
Patient experiences of the physician care they received were widely variable. While some patients were re-lieved to find a physician who appreciated the physical and emotional toll of the disease and worked with them to manage its impact, other patients had less favorable experiences with their physicians, feeling that their distress and the severity of their disease were not taken seriously. Some patients felt that their physician lacked awareness of CSU and reported that the approach to their treatment felt like a case of trial and error, with the perception that error was more commonly experienced. CSU treatment tended to follow a common pathway, starting with a single-agent H1-antihistamine and moving to H1/H2-antihistamine combinations if first-line treatments were ineffective. Often, additional drugs were added to the regimen in an effort to control symptoms and improve QoL. Many treatments did not decrease symptoms or only worked for a while before breakthrough symptoms occurred. When this happened, patients’ treatment expectations were lowered, from hoping for remission or a cure to hoping for reduced symptoms. Some patients were seen to take a more active role in treatment decisions over time but the general pattern of searching for answers, regularly feeling frustrated, and wanting more information persisted.
On a practical level, CSU presented a financial burden that, in some patients (e.g., those with inadequate or no health insurance), affected their decision-making about medical care, such as when to engage a specialist physician and how long to pay for on-going treatment. Medication costs were felt to be high, particularly in patients taking a combination of drugs daily. Several patients experienced difficulties with Medicaid access and chose to stretch out intervals between physician visits or take breaks from care, when costs became onerous or when their financial situation was compromised through loss of earnings owing to days missed from work as a result of CSU symptoms.
Table I. Key themes associated with living with chronic spontaneous urticaria
Physician participants
Six dermatologists and 6 allergists took part in the study. In the 3 months prior to the study, these physicians reported seeing between 10 and 128 patients with CSU, for whom they had prescribed drug therapy, including biologics, for the control and management of their disease.
Study findings revealed 3 common themes: concerns about the patient’s care pathway and the challenges inherent in treating an idiopathic disease; the need for better education on CSU; and the difficulties of managing symptoms in a disease where breakthroughs regularly occur. Sample narratives are presented in Table II.
(i) The care pathway
Some physicians expressed frustration at not having a clear care pathway or formal procedure for disease classification. They acknowledged the difficulties of treating and managing patients with a disease where the cause or trigger may be unknown and for which diagnosis involved excluding other possible causes. Physicians also recognized that their patients had often seen a number of other healthcare providers already, without diagnosis or treatment success. Approaches to conducting tests differed among physicians; some agreed when patients asked for them, believing it to be reassuring if the patient expected them, while others considered this unnecessary and that it could lead the patient to expect an answer or cause when this was in fact unlikely.
Some physicians showed considerable empathy for the frustration and sense of urgency expressed by patients and recognized the emotional and physical impact of the disease on patients’ QoL. Other physicians admitted that they struggled with CSU patients, who required more clinical time and more reassurance. Referring patients to a mental health professional for psychological support was perceived as potentially beneficial by some physicians. Other physicians felt that this was not necessary.
(ii) CSU education
Physicians understood that patients often came to them having received unhelpful advice or misleading information about their disease from friends and family. They also understood that other members of the medical profession, including general physicians, may not have been equipped with the appropriate information on CSU and thus some clarification was necessary. Physicians recognized that patients regularly used the Internet but advised them to be careful about what they found online, owing to the wide availability of information that is not validated or evidence-based.
(iii) Symptom management
Physicians expressed frustration with treating patients while being aware that therapy may be ineffective. Physicians felt concern over the best course of treatment for patients, commenting that it sometimes kept them awake at night. They were also conscious of the cost and insurance implications of treatments.
Table II. Key themes associated with the treatment and management of chronic spontaneous urticaria (CSU)
This study offers important insights into patients’ experiences and physicians’ perspectives on the management of CSU in the USA. It provides a better understanding of how support could be improved for patients and physicians, in order to advance knowledge and education of the disease and improve patient–physician communications. The findings also identified unmet needs in the management of CSU and concerns relating to the physical and psychological burden of disease.
Although many patients visited a physician soon after symptom onset, others waited up to 2 years, suggesting that further research of the barriers to accessing timely care would be valuable. Some patients reported months or even years of frustration, anxiety and/or depression before finding the ‘right’ physician to meet their needs. Patients were frustrated by the time it took to reach a diagnosis, with repeated physician visits and different treatments, often without success. Physicians experienced frustration as they sought to help patients understand the concept of idiopathy, which they recognized was distressing to patients in search of an identifiable cause.
Our study highlights how important it is for patients to have their concerns taken seriously. Being actively included in treatment decisions may help to build patient confidence and potentially alleviate some of the psychological sense of powerlessness that many patients reported in this study. Utilizing motivational interview-ing techniques, in which the autonomy of the patient is respected (22), asking open-ended questions and engaging in active listening may help to strengthen the patient–physician relationship and encourage patients to see their physician as an ally, working with them to achieve better outcomes in disease management.
Qualitative studies such as ours complement data from quantitative studies (23, 24) and can be used to guide the management and support offered to patients. The updated EAACI/GA²LEN/EDF/WAO 2017 guideline acknowledges the effects of CSU on QoL, and the burden of the disease for patients, their family and friends, and for the healthcare system (1). As part of managing CSU, the guideline recommends that physicians devote more time to SDM with patients (1). SDM is particularly important in chronic diseases and the benefits of a collaborative approach to patient care are becoming increasingly recognized in the medical community (25). In SDM, patients and physicians provide valuable sources of information, supplying different – but equally valuable – contributions (25).
Many patients used the Internet as a key source of information in their quest to find a cause of their disease. As not all sites contain accurate, reliable information, this can lead to patients being misinformed. However, the benefit of the Internet is that it allows patients to connect, through social media, to others with chronic conditions. Patients value the knowledge of others living with the same condition (26) and social media allows them to share disease management strategies, and offer and receive emotional support (27). There is clearly an opportunity for patient advocacy organizations to improve CSU education and such organizations can also play a role in moderating the discussions that happen at the peer-to-peer level.
We suggest that the psychosocial impact of CSU warrants further study and that the next step for all stakeholders (including advocacy groups, physicians, industry and payors) should be to examine further the social and emotional aspects of living with CSU. The gaps in knowledge and support identified from our study may be addressed through effective partnerships. Additional research on referral for counseling could also be of value, as this is something that is not covered in depth in the available guidelines.
Although our study provides important findings that may help to improve the care of patients with CSU, there are some limitations. The qualitative nature of the study and small sample size (25 patients, 12 physicians) limit generalization of the results. In addition, as many patients in this study had severe CSU (based on the medications they received), the population does not fully reflect the heterogeneity of the disease and diversity of patients with CSU. As such, our results cannot be extrapolated to the full population of patients with CSU. Similarly, as only a small number of physicians were surveyed, we cannot be certain that their responses reflect the approaches and perspectives of the wider medical community. Nevertheless, our findings regarding US patients with CSU correspond with those of a European study that assessed the perspectives of patients and healthcare professionals on CSU using a narrative medicine methodology (11). Similar to our study, the Italian study found patients experienced a range of negative emotions, with frustration common in the period leading to diagnosis and a high proportion of patients reporting impairment to QoL (11). Other studies have also reported patient dissatisfaction with their treatment and physicians (5, 8). However, patients whose physicians had discussed the emotional impact of CSU were significantly (p < 0.001) more satisfied with treatment and more trusting of their physician. From the physician’s perspective, treating patients with CSU can be challenging. In one survey, physicians (dermatologists, pediatricians and general practitioners) viewed patients with CSU as having a considerable emotional burden combined with high expectations, which could be difficult to meet (12).
For patients with CSU, the journey to diagnosis and appropriate treatment can be a slow and challenging path to tread, and the reasons why some patients wait up to 2 years before seeking medical advice could be examined further. The unmet needs identified from this study include the requirement for better support and further education, for both patients and physicians, to improve awareness of CSU and facilitate earlier diagnosis and suitable treatment. Maintaining open channels of communication and engaging in SDM may benefit the patient–physician relationship and improve patient outcomes.
Financial support statement: This study was sponsored by Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. Heather St Michael, of Fishawack Communications Ltd, Abingdon, UK, provided manuscript drafting, editorial and medical writing support, funded by Novartis Pharmaceuticals Corporation.
Conflicts of interest: SG has received an honorarium for acting as a speaker for Genentech. SE is an employee and LM a past employee of a not-for-profit patient advocacy organization, the Asthma and Allergy Foundation of America, which has re-ceived educational grants for non-branded activities, and funding from pharma for education and awareness initiatives. TAW is an employee of Allergy & Asthma Network, a non-profit patient advocacy organization, which has received grants for unbranded awareness and education initiatives. LK works for Flince Research and Design. DD, BP, AK and VD are employees of, and hold stocks in, Novartis Pharmaceuticals Corporation. HLS has provided consultancy, speaker and clinical investigator services, for which he has received honoraria from Genentech and Novartis.


 Click to show fullsize
Click to show fullsize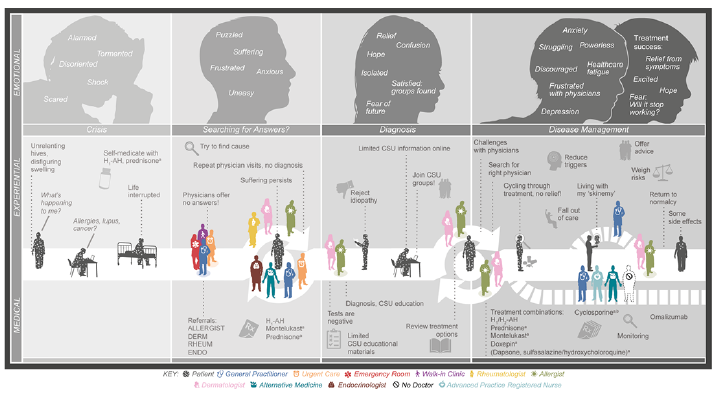 Click to show fullsize
Click to show fullsize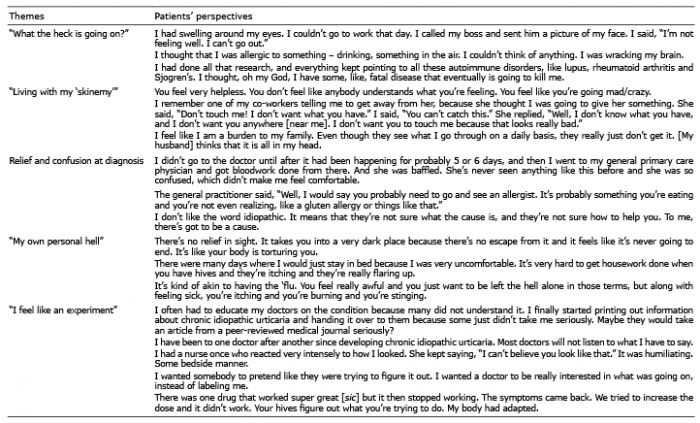 Click to show fullsize
Click to show fullsize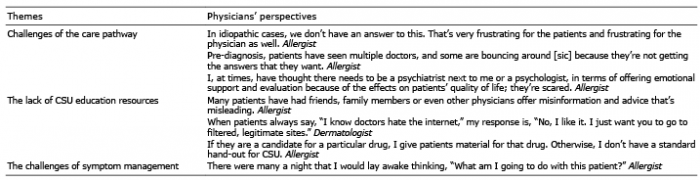 Click to show fullsize
Click to show fullsize