


1Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 2Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, and 3Center for Global Health, School of Public Health, Nanjing Medical University, Nanjing, China
To identify the microorganism distribution, clinical characteristics, and management of cutaneous Mycobacterium tuberculosis and nontuberculous mycobacterial infectious diseases in the past 10 years, we collected and analyzed the patient records of all cutaneous M. tuberculosis and nontuberculous mycobacterial infection cases diagnosed by culture and/or PCR from 2008 to 2017 in the Hospital of Dermatology, Chinese Academy of Medical Sciences. Among 203 cases, including 89 M. tuberculosis infections and 114 nontuberculous mycobacterial infections, M. tuberculosis was the most common species in all patients, and M. marinum predominated among the nontuberculous mycobacterial, followed by M. abscessus. Cases of cutaneous mycobacterial infection, especially nontuberculous mycobacterial infection increased in the past 10 years, and infection with rapidly growing mycobacteria significantly increased in the last 5 years in this national hospital in Southeast China. Injuries were common causative factors. Approximately 91.3% of patients responded well to longstanding antibiotic therapy.
Key words: infectious skin diseases; Mycobacterium; Mycobacterium tuberculosis; nontuberculous mycobacteria; retrospective study.
Accepted Aug 8, 2019; E-published Aug 9, 2019
Acta Derm Venereol .
Corr: Hongsheng Wang, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, Jiangsu, 210042, China. E-mail: wanghs@ncstdlc.org
Cutaneous tuberculosis or nontuberculous mycobacteria infections are frequently underdiagnosed. Although the high burden of tuberculosis and increasing incidence of nontuberculous mycobacteria infections have been recently reported, cutaneous infection caused by tuberculosis and nontuberculous mycobacteria occur rarely and remain unnecessarily reported in most regions of the world. This group of diseases shares many similarities on their histopathology such as granulomatous reaction pattern and their nonspecific clinical presentations. However, the severity, treatment, and prognosis may vary among species and patients. We focused on cutaneous tuberculosis and nontuberculous mycobacteria infections, determined their prevalence, species distribution, and clinical characteristics in the same period, and presented a view of these diseases in Southeast China.
Mycobacterium can be simply divided into 3 main groups: Mycobacterium leprae, M. tuberculosis complex, and nontuberculous mycobacteria (NTM). Although the high burden of tuberculosis and increasing incidence of NTM infections has recently increased public health concerns, cutaneous M. tuberculosis (MTB) and NTM infections are rarely analyzed and are unnecessarily reported in many regions of the world (1–3). These diseases share many similarities in their histopathology, such as the granulomatous reaction pattern and nonspecific clinical presentations, though the severity, treatment, and prognosis may vary by species and patient (2).
Cutaneous MTB or NTM infection is frequently underdiagnosed because of unawareness of mycobacterial infections and limited laboratory facilities and examinations. The available data on cutaneous mycobacterial infection mostly originate from scattered reports separately focusing on MTB or NTM (4–7). The present study aimed to describe the epidemiological and clinical aspects of cutaneous MTB and NTM infections in the outpatient department of the Hospital for Skin Diseases, Chinese Academy of Medical Sciences in Southeast China in the past 10 years.
Composition of the population
We searched the database of the Laboratory for Mycobacteria research in this hospital for the records of patients diagnosed with cutaneous MTB or NTM infection based on clinical characteristics and etiological examinations over a 10-year period from January 1, 2008, to December 31, 2017. The Hospital for Skin Diseases, Chinese Academy of Medical Sciences in Jiangsu Province is the national center for leprosy control and prevention. From 20 years ago, when the diagnosis of cutaneous mycobacterial infections with culture and PCR started, new species have been identified several times in this hospital. The hospital is also a referral center accepting more than 870,000 patients per year from surrounding mixed rural and urban areas in Southeast China. Hence, we believe that the population of our study is a remarkable model for residents in the local region.
Confirmation of cases
The diagnosis of cutaneous MTB or NTM infection was based on a combination of clinical and microbiological evidence, starting from a clinical presentation of cutaneous MTB or NTM infection. The skin tissue, then homogenates, and exudate or pus were collected from the patients and inoculated on a solid substrate: Lowenstein Jensen slopes at 32°C and 37°C for at least 1 month and up to 3 months or were immediately sent for PCR amplification. The cultured organisms were confirmed by Ziehl-Neelsen staining as acid-fast bacilli. Mycobacterial genomic DNA was extracted from clinical specimens directly or from those colonies growing on the medium. The diagnosis was evaluated by PCR amplification of specific hsp65, 16S, or rpoB ribosomal RNA coding sequences for rapid identification. The species was confirmed by DNA sequencing, followed by comparison through the Basic Local Alignment Search Tool of the National Center for Biotechnology Information.
Data analysis
Data on the diagnosis, clinical features, medical and disease history, antimicrobial drug therapy, and prognosis were obtained and analyzed. The data were described as the number, ratio, and mean value according to different types, and the statistical analysis for categorical variables was performed using the chi-square test or Fisher’s exact test, when appropriate. A p-value of < 0.05 was considered statistically significant. All the analyses were performed using SPSS 20.0.
Microorganism distribution
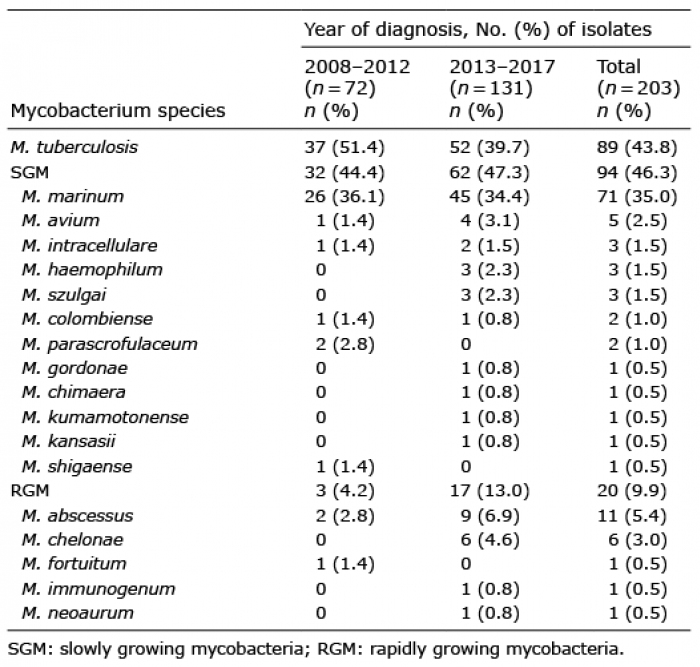
In a total, 203 cases diagnosed as cutaneous MTB or NTM infection from January 1, 2008, to December 31, 2017, were enrolled. The number of cases was generally increased during the study period (Fig. 1). In summary, 18 species, including 17 NTM species, were identified (Table I). The most common isolated species was MTB (43.8%). However, NTM infection accounted for 56.2% of cases and had exceeded MTB since 2014. The most common NTM species was M. marinum (35.0%), followed by M. abscessus (5.4%), M. chimaera, M. gordonae, M. kansasii, M. kumamotonense, M. shigaense, M. fortuitum, M. immunogenum, and M. neoaurum were each only isolated once. Over the last 5 years (2013–2017), 17 of the 79 (21.5%) NTM strains (including M. abscessus, M. chelonae, M. immunogenum, and M. neoaurum) were rapidly growing mycobacteria, and only 3 of the 35 (8.6%) strains (including M. abscessus and M. fortuitum) were isolated in 2008–2012 (χ2 = 2.81, p = 0.09). No patient was infected by more than one Mycobacterium species. In total, 74 had the T-SPOT. TB test (Oxford Immunotec Ltd., Abingdon, UK), a representative interferon-gamma release assay, was performed. The test was positive in 48 cases, including 93.5% (29/31, 3 with pulmonary tuberculosis) with cutaneous tuberculosis and 58.1% (19/31) with RD1-region sharing NTM infection (M. marinum, M. kansasii, and M. gordonae).
Table I. Comparison of mycobacterium species by year for 203 cases of cutaneous M. tuberculosis and nontuberculous mycobacteria infection
Fig. 1. Cases of cutaneous tuberculosis (MTB)/nontuberculous mycobacteria (NTM) infection in the outpatient department of the Hospital of Dermatology, Chinese Academy of Medical Sciences (2008–2017).
Population
A total of 78 men (46.2%) and 91 women (53.8%) of 6–86 years of age (median: 53, mean ± SD: 52 ± 16 years) were enrolled (Table I). The patients mainly work on agriculture (23.3%, 24/103) and aquatic industry (fishers, fish farmers, fishmongers) (13.6%, 14/103). The patients who worked in the aquatic industry were overrepresented in those infected with M. marinum (34.2%, 13/38).
Clinical characteristics
A total of 103 patients with intact clinical records were available for further study. The species included MTB (33), M. marinum (38), M. abscessus (10), M. chelonae (4), M. intracellulare (3), M. haemophilum (3), M. szulgai (3), M. colombiense (2), M. avium (1), M. parascrofulaceum (1), M. gordonae (1), M. kumamotonense (1), M. shigaense (1), M. fortuitum (1), and M. immunogenum (1).
NTM can be divided into the following 2 categories based on their speed of forming mature colonies on media: rapidly growing mycobacteria (RGM) or slowly growing mycobacteria (SGM). In the current study, M. marinum predominated and was separated from other NTM infections. The clinical characteristics of different infections were examined separately and are presented in Table II. NTM infected more females than males, and MTB infected more males than females (χ2 = 5.68, p = 0.02).
Table II. Characteristics of patients with cutaneous M. tuberculosis (MTB) and nontuberculous mycobacteria (NTM) infectious disease (2008–2017)
The time lapse between onset and diagnosis ranged from 1 month to 30 years. The mean course of MTB infections was much longer than other infections. A short interval of RGM infection was observed. An interval period of less than 1 year was significantly different between RGM and MTB infections (χ2 = 7.67, p < 0.01). The difference between RGM and M. marinum and other SGM infections in this period was not significant.
An apparent injury history, including trauma (26.2%), aquatic contact (14.6%), cosmetic procedures (4.9%), and iatrogenic procedures (1.9%), was found in 49 (47.57%) cases. Ratios and reasons for the injury differed in various groups. The M. marinum infections had a higher rate of injury than other infections, 55.6% of which were caused by aquatic animals, and the remaining 44.4% were caused by trauma. The occupations of the M. marinum infection patients included 3 fishers, 5 fish farmers, 5 fishmongers, 1 sailor, 1 aquarist, 2 housewives, 1 cook and 6 farmers. Nineteen had daily contact with fresh water, and the remaining 5 had more access to seawater and marine animals. Among the 39.5% (15/38) that had a stab or bite history, 2 were caused by marine fish and 13 were caused by freshwater organisms. An especially high ratio of cosmetic or vaccine injection history was observed in RGM infections (31.3%, 5/16; i.e., 3 patients with M. abscessus infection underwent a botulinum toxin injection, one underwent BCG vaccination in related institutes and one patient was infected with M. immunogenum after undergoing facial care in a beauty center.
Impaired immunity was found in 10.7% of patients, 10 of whom suffered from autoimmune disease, including rheumatoid arthritis (4/11), systemic lupus erythematosus (3/11), or renal insufficiency (3/11), with oral administration of glucocorticoid or immunosuppressant for more than 1 year. Only one patient showed a low CD4+ T-cell percentage (25.7%). No patients were seropositive for HIV.
The following skin presentations were documented: nodule (51.5%), plaque (49.5%), erosion or ulcer (34.0%), erythema (20.4%), crust (16.5%), papule (14.6%), scale (9.7%), verrucous hyperplasia (4.9%), and abscess (2.9%). Lesions were frequently found on the hands (35.9%), face (22.3%), and forearms (20.4%). Approximately 28.2% of infections involving multiple sites were found. Most patients showed exclusive skin involvement without associated constitutional symptoms, and 4 patients (1 M. shigaense, 1 M. colombiense, and 2 M. abscessus) suffered from disseminated cutaneous lesions. A total 5 patients showed organ or system involvement, i.e., intestinal infection with M. colombiense, paranasal infection with M. gordonae, pulmonary and marrow infection with M. intracellulare, and hematogenous dissemination of M. abscessus and M. shigaense. Few patients complained of obvious pain (9.7%, 10/103) or pruritus (13.6%, 14/103) in the study.
Treatment and outcome
Treatment and prognosis information were available for 103 patients. All patients received antimicrobial therapy. In several M. abscessus and MTB infection cases, plastic surgery was also conducted for cosmetic improvement or the removal of infected tissue after the infection was controlled. Except in some of the M. marinum infections treated with clarithromycin or moxifloxacin alone (4 cases), all patients received combined antimycobacterial therapy. The improvement was addressed according to visible scarring or recovery of the lesions, with or without the conversion to a negative etiological examination. The infection was considered clinically cured when the lesions were completely recovered or scarred and no relapse was observed during the study period.
Until April 2018, 91.3% of patients were satisfactorily treated. Approximately 48.5% were completely cured (Table II, Fig. 2). A total of 9 patients exhibited a poor prognosis, 7 of whom did not respond well to antimicrobial therapy and 2 of whom died due to systematic infection or infective complications (1 M. avium and 1 M. shigaense). Among these 9 patients, 4 underwent a change in the primary drug therapy because of unendurable drug side effects, including dizziness, blurred vision, low platelets, and exfoliative epidermal necrolysis, 2 patients were infected with multidrug-resistant strains, and 3 patients did not take the drug regularly. Patients who suffered from unendurable drug reactions (14.6%, 15/103) were more likely to show poor outcomes (26.7%, 4/15) compared with the others (χ2 = 4.69, p = 0.03). No significant difference in prognosis was found between people with different immune statuses.
Fig. 2. Cutaneous tuberculosis (TB)/nontuberculous mycobacteria (NTM) infection after antibiotic treatment. (A, B) Tuberculosis verrucosa cutis for 4 months and after 9 months of standard antituberculosis treatment. (C, D) Lupus vulgaris for 5 months and after 3 months of standard antituberculosis treatment. (E, F) Tuberculosis cutis orificialis for 20 years and after 3 months of antituberculosis treatment. (G, H) Mycobacterium marinum infection treated with clarithromycin and moxifloxacin for 6 months. (I, J) Mycobacterium abscessus infection treated with clarithromycin and moxifloxacin for 1 month. (K, L) Mycobacterium chelonae infection treated with clarithromycin and moxifloxacin 2 months.
Epidemiology
Given the growing rate of HIV infection, widespread immunosuppressant use, population aging, and improved detection methods, cutaneous mycobacterial infection appears to be increasing in recent years (5, 8). Although culture and a series of biomolecular testing are very helpful in limiting confusion and formally identifying the mycobacterium species, PCR-based DNA sequencing and homology comparisons are considered the best for pathological organism identification (9). Our present study involving MTB and NTM infection confirmed by the combination of the clinical spectrum and etiological examination identified a total of 203 cases over 10 years in Southeast China. The medical literature notes a temporal trend in which the prevalence of NTM infection generally rose while the prevalence of MTB declined, although the burden of these diseases is often poorly investigated (10). In the Hospital of Dermatology, Chinese Academy of Medical Sciences, cases of cutaneous MTB and NTM infection generally increased from 2008 to 2017, and the number of NTM infections has doubled in the past 5 years. In the past 10 years, although cutaneous MTB infection was still the leading cause of cutaneous mycobacterial infection in all cases (43.8%, 89/203), which is consistent with the prevalence of tuberculosis, the incidence of cutaneous NTM infection had exceeded that of MTB since 2014 and was identified in more than half of all patients. These findings demonstrated an increasing number of NTMs isolated not only in pulmonary infections but also in skin and soft tissue infections. NTM species composition was diverse in different geographical areas, as suggested in the literature (4–6, 8). In pulmonary infections, the NTM prevalence rate and RGM composition in South China were much higher than in Northeast China, emphasizing the importance of building a knowledge base of mycobacterial infections from local studies (11). In cutaneous NTM infection, the proportion of M. marinum (62.3%) was always the highest in NTM species over 10 years, which was similar to that described in other studies (5, 6, 8). However, RGM were the most common species in some regions (12). Compared with that in the past 5 years, the number of RGM isolates increased in 2013–2017, which shows a tendency suggested in the literature (8), and M. abscessus became the second most common NTM species (9.65%, 11/114).
Clinical settings
In the present study, cutaneous infection often occurred in elderly patients. However, only 10.7% (11/103) were in an immunosuppressed state, which could partly be ascribed to the good physical condition of the patients in specialized hospitals. Although immunocompromised individuals are at particular risk and the increase in mycobacterial cutaneous infections is related to the growing immunosuppressed population (5, 8), our findings suggest that these infections mainly occurred in immunocompetent people.
A history of injury is an identified risk factor, as minor wounds on the skin may constitute the portal of entry of mycobacteria from the environment (13). The population with M. marinum infection showed a high frequency of injury history and occupational exposure. RGM are relatively resistant to standard disinfectants, such as ethyl alcohol and chlorhexidine and potentially cause infections through improperly sterilized instruments (2). RGM infection outbreaks with transmissions from tattoos, acupuncture, pedicures, liposuction, and injections have been widely reported and suggested as the cause of increasing RGM infections in recent years (14–17). However, these cases have been sporadic, and the absence of an outbreak infection observed in the study time may suggest the universality of mycobacteria in the natural environment.
Cutaneous MTB or NTM infection is suspected on the basis of the clinical spectrum. However, lesions owing to cutaneous MTB and NTM infection were highly variable (18). The wounds commonly presented as long-lasting painless lesions and have been misdiagnosed for a long time because of the limited medical condition in local areas (19). The delay between the onset and diagnosis of M. marinum (55.3%) or RGM infection (68.8%) was often less than one year, whereas patients infected with MTB (72.7%) and other SGM (68.8%) usually suffered for more than one year. Considering that the injury history was more common in M. marinum and RGM infections, we suspect that the short intervals correlate with a stronger tendency to visit a hospital. The NTM infections mostly occurring on the extremities (80.9%, 93/115) also suggest the importance of the injury history before onset. SGM infection was more likely to involve multiple locations, similar to a previous study (20), but the difference was not statistically significant. Two cases of M. abscessus infection may suggest the potential spread of RGM infections.
Treatment and prognosis
Cutaneous MTB infection treatment following the recommendations of the WHO comprises an intensive phase for 2 months, followed by 4 months of a maintenance phase (21). Quinolones or macrolides are recommended by the WHO for multidrug-resistant tuberculosis with good safety but unclear efficacy (22, 23). In one patient, the first-line drugs were switched to quinolones and macrolides after an intolerable adverse reaction, resulting in a satisfying outcome. Cutaneous NTM infection therapy usually depends on retrospective case series, and no standard guidelines or consensus have been founded until now. The American Thoracic Society and the Infectious Diseases Society of America suggest the combination of clarithromycin and ethambutol to treat M. marinum infections without the need for susceptibility testing (24). In the present study, most M. marinum infections were treated with clarithromycin combined with rifampicin, moxifloxacin, or levofloxacin, yielding good results, although a few patients were cured with clarithromycin alone, similar to our earlier report (25). The therapy continued for 3–6 months and usually extended another 1–3 months after the lesions markedly improved. M. abscessus exhibits a natural multidrug resistance pattern to most antituberculous drugs but is often sensitive to clarithromycin, amikacin, and cefoxitin (26). However, the results of the in vitro drug sensitivity test for M. abscessus may be quite different. As these infections rapidly progress, suspected patients are recommended to start empirical therapy immediately after diagnosis and ideally adjusted by culture and susceptibility testing (26). In the present study, most of our patients responded well to a combination therapy containing at least 2 drugs, including clarithromycin.
In general, primary treatments responded well in most patients, and some were adjusted later with the support of in vitro drug sensitivity testing. Reasons for poor outcomes included drug resistance, immunocompromise status, intolerable side effect, pretreatment history, and irregular treatment. The intolerable drug side effects were considered a major risk factor for poor outcome, so physicians must be aware of potential reactions and change the therapy in a timely manner during treatment.
The limitation of the study is that although the in vitro culture and PCR detection are considered a better choice for identifying the pathogen and making a confirmed diagnosis of cutaneous mycobacterial infections, there may be some patients with consistent clinical manifestations or biopsies but negative microbiological tests results who were excluded from the study according to our criteria, which may have caused a comparably incomplete or skewed picture of the disease.
Conclusion
This study presents a view of cutaneous MTB and NTM infection in the patients of the Hospital of Dermatology, Chinese Academy of Medical Sciences, the number of whom has risen in the past 10 years. The number of NTM infections has exceeded that of MTB infections since 2014, and RGM infections have increased in the latter 5 years. M. marinum was the most common NTM, followed by M. abscessus. The infection often occurred in elderly people. Numerous differences were observed between different mycobacterial infections in sex, natural course of disease, causative factors, and clinical presentations. For indistinguishable characteristics and different treatment strategies, infections with cutaneous MTB and NTM must be frequently suspected and cautiously diagnosed. This disease is generally efficiently managed with long-term antibiotic treatment. Further attention must be drawn to related clinical and epidemiological research. Doctors must be aware of cutaneous MTB and NTM infection to facilitate prompt diagnosis and correct treatment.
Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (CIFMS-2016-I2M-1-005), National Natural Science Foundation of China (81371751), Natural Science Foundation of Jiangsu Province of China (BK20141065) for Hongsheng Wang.
The authors have no conflict of interests to declare.


 Click to show fullsize
Click to show fullsize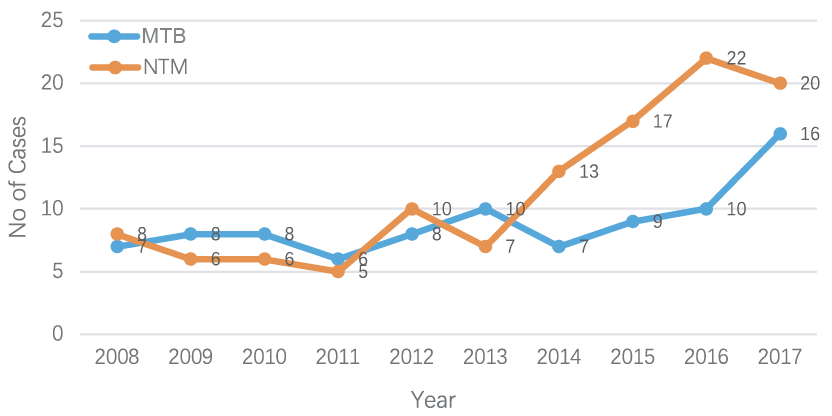 Click to show fullsize
Click to show fullsize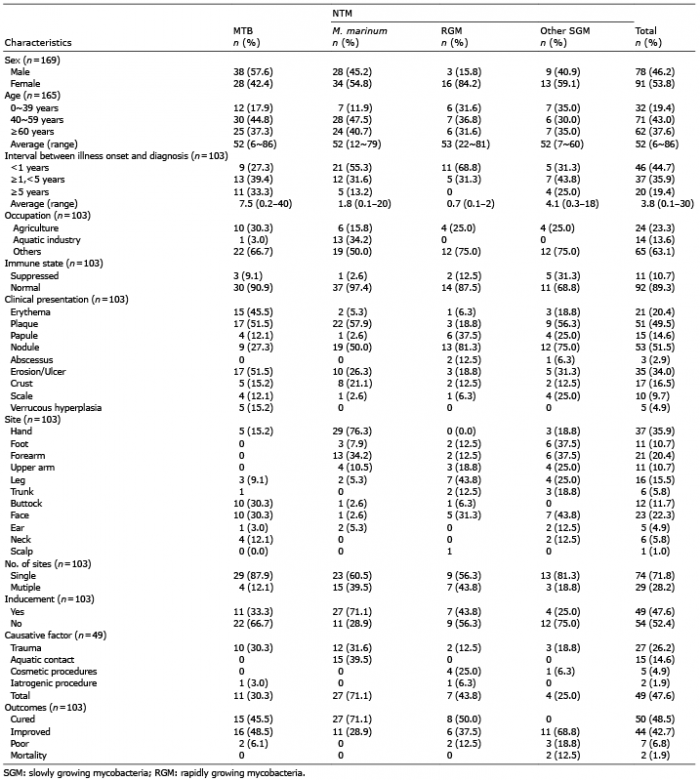 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize