


1Unit of Dermatology, Department of Medicine – DIMED, University of Padova, Italy, 2Ben Gurion University of the Negev, Beer Sheva, Israel, and 3OUC of Histopathology, University of Padova, Padova, Italy. *E-mail: michael.dennis.linder@gmail.com
#These authors contributed equally.
A 17-year-old Caucasian girl presented with a 1-year history of an eczematous, persistent, slowly growing, pruritic lesion on her left nipple and areola. Clinical examination revealed a well-demarcated brownish plaque sprinkled with multiple punctate vascular spots, slightly scaling on the surface (Fig. 1a). There were no relevant anamnestic data to report. The right breast was not affected.
As fungal and bacterial cultures were negative and clinical features were consistent with nipple eczema, she was initially treated with topical steroid, but with no improvement.
A 6-mm punch biopsy revealed a spongiotic and markedly acanthotic epidermis with proliferation of pale keratinocytes easily distinguished from normal ones. The epidermal ridges were elongated in a psoriasiform manner and fused, the granular layer was almost absent and the stratum corneum showed parakeratosis and serous exudate (Fig. 2a). Clear cells stained positively with the routine periodic-acid-Schiff, indicating the presence of glycogen (Fig. 2b). Intraepidermal portions of the annexes were normal. The underlying dermal papillae showed dilated capillaries and a scarce inflammatory cell infiltrate with predominantly lymphocytes and some granulocytes.
What is your diagnosis? See next page for answer.
Fig. 1. (a) Eczematous, pruritic, brownish plaque on the left nipple and areola of a 17-year-old girl. (b) Complete regression after 6 months of 0.05% topical tretinoin.
Fig. 2. Histological features: (a) Epidermal acanthosis with elongation of the rete ridges and loss of granular layer. Proliferation of pale keratinocytes (clear cells) with bright cytoplasm and normal nuclei (haematoxylin-eosin ×4). (b) Clear cells are rich in glycogen and stained positively (periodic acid Schiff (PAS) ×10).
Acta Derm Venereol 2020; 100: XX–XX.
Diagnosis: Clear cell acanthoma
Clear cell acanthoma (CCA) is a relatively rare benign epidermal lesion mostly affecting middle-aged to elderly individuals. It was first described by Degos et al. in 1962 as presenting the “stuck on” appearance of seborrhoeic keratosis, the vascular look of a pyogenic granuloma, the scaling and exudation of eczema and the advancing round border of an epithelioma (1).
CCA typically presents as an asymptomatic reddish dome-shaped papule or nodule with a scaly or bloody surface. It usually occurs on the lower limbs as a solitary lesion, but can be multiple (2). Dermoscopy is characteristic, showing a linear serpiginous “string of pearls” vascular pattern.
Its aetiology is still under debate. Although it was initially considered a benign tumour, the frequently reported overlap with inflammatory skin diseases, such as psoriasis or atopic dermatitis, suggested a reactive origin, secondary to chronic inflammation (2, 3).
CCA of the nipple or areola is a very rare finding. To date, CCA seems to have been reported in no more than 12 patients, with 5 cases from Korea, 2 from the Philippines, 2 from Brazil, 1 from Spain, 1 from Italy and 1 from Cuba (4–9). Only one male case has been described (9).
Nearly all of these cases of CCA of the nipple and areola have occurred in patients with a long-lasting history of atopic dermatitis, supporting the hypothesis that CCA is a reactive dermatosis. Moreover, the higher frequency among Asian patients in the few published cases of CCA of nipple and areola, could be explained by the greater incidence of nipple eczema in this population than in Caucasians (6).
CCA of the nipple is reported to present clinically as an eczema of nipple and areola, associated with pruritus (5). A case of polypoid CCA has been reported (6).
The differential diagnosis of CCA on the nipple or areola may include basal cell carcinoma, squamous cell carcinoma, Paget’s disease, eczema, psoriasis, seborrhoeic keratosis, syringadenoma papilliferum and pemphigus vegetans (1).
The histopathology is quite distinctive. It shows well-defined psoriasiform acanthosis, composed of clear cells with bright cytoplasm and normal nuclei associated with loss of the granular layer. Clear cells are rich in glycogen and stain positively with periodic acid Schiff (PAS). The papillary dermis presents dilated capillaries and rare mixed inflammatory infiltrate (4). Poromas might also be considered in the histological differential diagnosis.
Although CCA is considered a benign lesion, appropriate treatment may be required to stop its progressive growth. No recurrences were observed with surgical resection and cryotherapy (8). Only 4 cases were reported to show remission with topical corticosteroids (7). Oral non-steriodal anti-inflammatory drugs, topical antibiotics and tacrolimus cream appear to be ineffective (1). Topical retinoids occasionally proved effective, as for instance in a case involving an eyelid (10). Also in the current case the lesion showed complete regression after application of 0.05% topical tretinoin over 6 months (Fig. 1b).


 Click to show fullsize
Click to show fullsize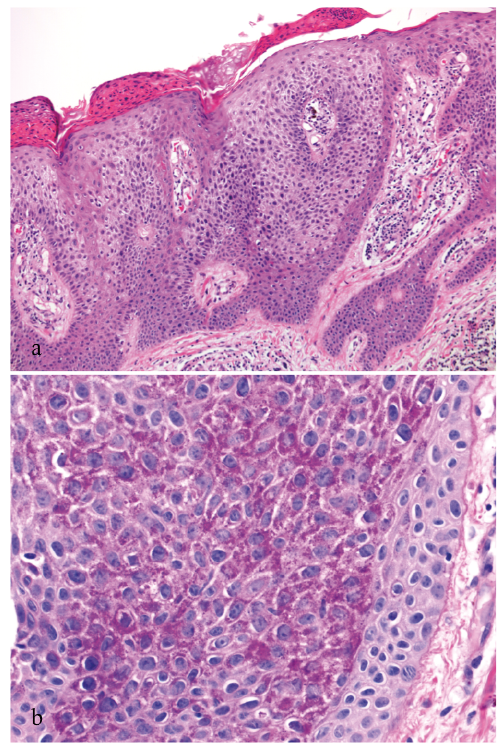 Click to show fullsize
Click to show fullsize