


1Department of Plastic and Reconstructive Surgery, Rikshospitalet, Oslo University Hospital, 2Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, 3Department of Microbiology and Infection Control, Akershus University Hospital, 4Multidisciplinary Laboratory Medicine and Medical Biochemistry, Akershus University Hospital, and 5Akershus Dermatology Center, Lørenskog, Norway?
Infectious pseudochromhidrosis is a rare dermatological disorder, characterized by a change in colour of the sweat from normal skin, caused by pigments from microorganisms. Such pigments are a result of evolutionary competition among microorganisms, which appears to be a decisive factor in their survival, patho-genicity, and virulence. Four bacteria are known to be involved in infectious pseudochromhidrosis: Bacillus spp. (blue colour), Corynebacterium spp. (brown/black colour), Serratia marcescens (red/pink colour), and Pseudomonas aeruginosa (blue-green colour). Infectious pseudochromhidrosis seems to be triggered by certain drugs and conditions causing physiological alterations and/or changes in microflora on the skin surface. The condition can be treated by addressing potential triggers and/or prescribing antibiotic/antiseptic therapies. We report here a case of blue infectious pseudochromhidrosis caused by pigment-producing Bacillus cereus and the results of a literature review.
Key words: chromhidrosis; pseudochromhidrosis; infectious pseudochromhidrosis; coloured sweat; pigment.
Accepted Oct 14, 2019; E-published Oct 14, 2019
Acta Derm Venereol 2020; XX: XX–XX.
Corr: Christoffer Ingvaldsen, Department of Plastic and Reconstructive Surgery, Rikshospitalet, Oslo University Hospital, Postboks 4950 Nydalen, NO-0424 Oslo, Norway. E-mail: c.a.ingvaldsen@medisin.uio.no
Microorganisms may produce pigments to increase the likelihood of survival. Under favourable conditions such pigments can result in coloured sweat and/or atypical skin discolouration in patients. This is a rare dermatological disorder named infectious pseudochromhidrosis. We report here a case of blue infectious pseudochromhidrosis caused by the bacteria Bacillus cereus and a literature review. The potential triggers, causative microorganisms, diagnostic approaches, and suggested treatments for infectious pseudochromhidrosis are addressed.
Chromhidrosis (from Greek: chroma [colour] and hidros [sweat]) is a rare dermatological disorder characterized by coloured sweat (1). Three different conditions can result in chromhidrosis (2):
Apocrine chromhidrosis is an intrinsic condition limited to areas with apocrine glands (e.g. face, axillae, anogenital area, and breast areolae) that excrete small amounts of oily sweat (1, 3). Oxidation of lipofuscin, as well as the increase in number of lipofuscin granules, are thought to cause the skin discolouration (4, 5). Lipofuscin is an intra-lysosomal polymeric material that gains colour as it oxidizes, with higher oxidation states resulting in a darker colour (1, 6–8). The oxidation may be triggered by chronic exposure to copper (e.g. from an intrauterine device or drinking water) and ammonium (9). There are reports of orange (9), red (10), blue (8, 9, 11–20), green (13, 21), and brown/black (22–26) sweat.
Eccrine chromhidrosis is generalized discolouration that occurs secondary to ingestion of water-soluble drugs (2, 27, 28), dyes (29–31), or due to breakdown products from eccrine glands (2, 32–35). Eccrine glands are distributed with varying density over almost the entire integument and excrete large amounts of sweat, containing mostly water and electrolytes (1, 3).
Pseudochromhidrosis is a condition where colourless, eccrine sweat becomes coloured by exogenous factors on the skin surface, such as chromogenic microorganisms (1, 2, 15, 36–38) and chemical agents (39–42). The reported colours are yellow (5), red (43–45), pink (46, 47), blue (2, 37, 38), green (36, 48), brown (39, 40), and black (44, 49, 50), most commonly localized on the face, neck, and palms (2).
Since bacteria are potential causative agents of pseudochromhidrosis; infectious pseudochromhidrosis (IPCH) is becoming an increasingly used term in literature (1, 15). To our knowledge, no definition of this disorder has been proposed. Moreover, there is no clear consensus in terms of disease triggers, causative microorganisms, and factors contributing to the clinical presentation of coloured sweat. The scope of this article was, therefore, to report another case of IPCH and to review the literature.
Case report
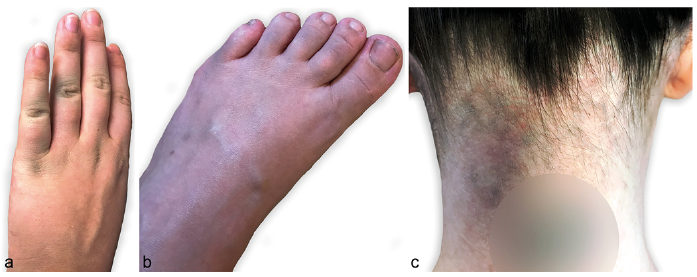
A 24-year-old woman presented with a 1-year history of an asymptomatic and odourless blue discolouration covering her hands, feet, and neck (Fig. 1). Her past medical history was insignificant and she had not been diagnosed with any underlying dermatoses. On the contrary, the patient reported daily attacks of cholinergic and dermographic urticaria, and hypohidrosis even after strenuous exercise and emotional stimuli. Her symptoms resemble acquired idiopathic anhidrosis; however, this was not investigated further.
Fig. 1. Clinical photographs. (a) Blue discolouration on dorsal side of the hand primarily covering the joints. (b) Diffuse blue discolouration with an ashen hue on dorsal side of the foot. (c) Diffuse blue discolouration on the neck. Blurred circle covering tattoo.
At the time of presentation, the patient was approximately 7 months pregnant with her first child. She had started daily 25 mg promethazine due to pruritus 6 months earlier. Promethazine was stopped 1 month after presentation with no change in colour intensity. The blue colour was present continuously, but was more obvious after physical activity. It could be removed with soap and water; however, it was more easily removed with alcohol wipes (Fig. 2). The patient also reported staining of her clothes, towels, furniture, and shower. Urine, stool, saliva, and tears were normal coloured.
Fig. 2. Alcohol wipes from (a) hands and (b) neck easily removed the discolouration and revealed its blue colour.
Initially, 2 blood samples were performed at her general physician’s office with a 1-month interval. These blood samples were normal, apart from slightly increased copper values (35 and 37 µmol/l), yet values were within reference range in pregnancy (19–47 µmol/l).
Retrospectively, her husband also recognized slight blue discolouration located on his right pectoral and deltoid region. He had no significant past medical history, underlying dermatoses, and did not use any medication. The blue discolouration appeared 2–3 weeks after his wife’s. No blood samples or other diagnostic tests were performed.
The first and senior author of this study saw the family of 3 approximately one year after presentation. An ashen hue was observed primarily on hands, feet, and neck (female patient), and right pectoral region (male patient). The underlying skin was normal. No skin discolouration was seen on their child. Dermoscopy of the discoloured areas revealed diffuse superficial pigmentation and an unmodified skin pattern (as postulated by Pistone et al. (51)). Skin examination with a Wood lamp revealed fluorescence on hands, feet, and hair (Fig. 3).
Fig. 3. Fluorescent material on dorsal aspects of the feet (especially interdigitally).
Multiple bacteriological and mycological swabs were taken from all 3 family members. Skin scrapings for dermatophyte PCR identification were taken from the female and male patient. All bacteriological swabs of female patient (neck, upper arm, axilla, hand, and foot) had heavy growth of 2 strains of Bacillus cereus. Two out of 5 swabs from the male patient (pectoral region and foot) yielded the same bacteria. The child’s swabs grew no microorganisms other than normal microflora. One of the B. cereus strains found produced blue pigments on blood agar, but the other did not (Fig. 4). All swabs and skin scrapings were negative for fungi. See below for methods for culture and identification of bacteria, and results. No skin biopsy was performed.
Fig. 4. Bacillus cereus: 2 isolates; one with a blue tint and one without.
We hypothesized that the female patient was the source. In order to assess for a potential underlying cause of B. cereus growth, she was scheduled for a second appointment. Additional investigations were performed, including blood and urine analyses. All tests were normal, apart from a slightly increased alkaline phosphatase (ALP) of 122 U/l (reference range 35–105 U/l). ALP had also been above upper reference limit prior to the presentation of blue discolouration (with no known or suspected cause). Copper was normalized in this blood sample.
Due to her reports of hypohidrosis, a sweat provocation test with following sweat pH measurements (Jenway pH meter, Model 3510, Cole-Parmer, Staffordshire, UK) were performed. The patient performed 15 min of indoor cycling and 15 min of treadmill running. During this exercise she produced some sweat. However, this was less than was subjectively expected. Her scalp, hair, anterior and dorsal trunk, palms, and feet were surprisingly dry. pH measurements of sweat were considered normal (mean/min–max: 5.6/5.1–6.5). No wheals were induced during exercise.
Both adults were treated with oral erythromycin, 250 mg 3 times a day, and topical clindamycin 2 times a day for 10 days. As the female patient still had a slight discolouration on her feet, she continued same topical treatment for 7 days. Complete remission of blue discolouration was achieved in both patients, and it did not return during an observation time of 6 months.
Bacteria culture and identification
The samples were cultivated aerobically, anaerobically, and for fungi. The isolates were initially identified by morphology, Gram stain, haemolysis on blood agar, penicillin susceptibility, and motility. The isolates were then subject to matrix-assisted laser desorption ionisation time of flight mass spectrometry (MALDI-TOF MS, Bruker Daltonik GmbH, Bremen, Germany) and 16S rRNA gene sequencing with primers based on MicroSEC® 500 16S rDNA bacterial sequencing kit (Life Technologies, Paisley, UK).
Results
Two different isolates were cultured; a greyish culture and a greyish culture with a blue tint (Fig. 4). Both were penicillin resistant, motile, and produced haemolysis on blood agar. As neither MaldiTOF nor 16S rRNA can distinguish properly between the B. cereus, B. anthracis and B. thuringiensis, it was concluded that the isolates belong to the B. cereus group and are non-anthracis. The B. cereus strains are referred to as B. cereus in the following text. PCRs for dermatophytes were negative.
Literature search
This is a narrative review. A literature search of PubMed, Cochrane Library, and Google Scholar was performed in the period November 2018 to January 2019. Search terms included “chromhidrosis”, “pseudochromhidrosis”, “coloured sweat”, “lipofuscin”, “bacterial pigment”, “fungal pigment”, and “promethazine sweat”. Articles in English, German, French, Dutch, and Danish were included. Full texts and reference lists were reviewed.
Case reports of infectious pseudochromhidrosis and causative microorganisms
Based on the literature review, there are only 4 bacteria that are confirmed to have resulted in cases of IPCH (Table I):
Bacillus species – blue IPCH (2, 37, 38): Bacillus is a genus of Gram-positive, sporulating rods that are aerobic or facultatively anaerobic and are widely distributed in the environment (soil, dust, water, food, and plants) (52, 53). In terms of pathogenic Bacillus spp., B. anthracis is the only obligate pathogen (where cutaneous anthrax represents 95% of cases worldwide) (53). B. cereus is an occasional pathogen that can cause various infections mostly associated with its secreted toxins (52–55). The B. cereus found in the current case report colonizes human skin and the intestinal tract (54), yet infections in immunocompetent patients are rare (56).
Corynebacterium species – brown/black IPCH (44, 49, 50): Corynebacterium is a genus of Gram-positive and (mostly) aerobic rods that is widely distributed in nature. Corynebacterium spp. are also found in the human microbiota and are, in general, innocuous (57, 58). The genus, however, which currently has more than 110 validated species, constitutes a very heterogeneous group (59). From a medical perspective, the pathogenic species C. diphtheriae (diphtheria), C. ulcerans (diphtheria-like infections), C. tenuis (trichomycosis axillaris), C. minutissimum (erythrasma), and C. striatum (endocarditis) might be of greatest interest.
Serratia marcescens – red/pink IPCH (45–47): S. marcescens is a Gram-negative, facultatively anaerobic, and saprophytic bacteria belonging to the Enterobacteriaceae family (60, 61). The ubiquitous bacteria have a predilection for starches and are rarely found in bacteriological skin cultures. Due to its production of red colour, the presence of S. marcescens has often been mistaken for sweating of blood (hematohidrosis) (45).
Pseudomonas aeruginosa – blue-green IPCH (36, 48, 62): P. aeruginosa is a Gram-negative, aerobic coccobacillus, which is widespread in nature (63). It is well known that the bacteria can colonize moist skin surfaces and can cause a greenish discolouration of skin, nails, clothes, and surgical dressings (48, 62, 64, 65).
There are also several case reports where IPCH has been suspected despite negative cultures (5, 43, 44, 51, 66). This tentative diagnosis has been strengthened by complete remission after antibacterial treatment, combining systemic and topical erythromycin in all cases.
Table I. Case reports of infectious pseudochromhidrosis and causative microorganisms
The pigments of microorganisms
The literature review revealed a repeated theme of micro-organisms producing pigments. Such pigments have, in some cases, been the suggested or documented reason for coloured sweat. In fact, research reveals hundreds of different pigment-producing microorganisms; bacteria, fungi, and parasites. The pigments described comprise a heterogeneous group of carotenoids (terpenoid pigments) (67–72), melanins (73–77), alkaloids (78, 79), porphyrins (80, 81), siderophores (65), and flavins (82).
Moreover, pigment production seems to be a decisive factor determining survival, pathogenicity, and virulence among microorganisms. Pigments do this by interfering with the host immune system and/or provoking inflammatory damage to cells and tissues (83). As such, some microorganisms invest heavily in pigment production, producing up to 30% of their dry weight as pigments (84). Many of these pigments are extracellular, and thereby able to colour the skin surface and/or stain clothes (85).
Concerning the 4 bacteria described above, the pigments have been chemically extracted and characterized in 2 of them: Serratia marcescens and P. aeruginosa.
The colour of S. marcescens IPCH is explained by its production of a red pigment, named prodigiosin, which gives the red/pink colour on the skin surface (46). Williamson et al. reported that the production of prodigiosin is highly dependent on temperature, pH, and other environmental factors (86).
P. aeruginosa may produce multiple water-soluble pigments, most commonly pyocyanin (blue) and pyoverdine (dim muddy yellow with a green fluorescence) causing the distinguishing blue-green hue (36, 64, 65, 87). “Aeruginosa” derives from the Latin word for copper rust, referring to the characteristic, pseudomonal discolouration (65).
Pigment production is known to occur in Bacillus spp. and Corynebacterium spp. However, studies do not mention the exact pigments causing blue and brown/black discolouration:
B. cereus has been shown to produce both a green (84, 88) and a red pigment (85). One study from Hiroshima reported large amounts of intracellular, purple pigment (copper coproporphyrin III) in a B. cereus strain (81, 89). To date, none of the previous studies have specifically reported a blue pigmentation as a result of colonization with B. cereus. Referred Bacillus spp. IPCH case reports (Table I) did, however, have blue-coloured sweat (which could potentially be pigments from B. cereus). Apart from B. cereus, previous studies have also described pigment production in many other Bacillus spp. (90–94).
Oliveira et al. reviewed pigment production in Corynebacterium spp., and reported that carotenoid production is one of many important virulence factors (59). Lycopene, the bright red pigment found in tomatoes, is one of the carotenoids produced (95). Only a few species, however, have been identified to produce carotenoid pigments (e.g. C. glutamicum, C. michiganese, C. erythrogenes, C. fascians, and C. poinsettiae) (59, 95). Leonard et al. also described a single strain of C. striatum that produced a soluble, brown pigment (96). Interestingly, this brown pigment production was enhanced when grown in the presence of tyrosine, which suggests that it is a melanin. Shulka et al. reported a novel Corynebacterium spp. that produced black pigment (with the proposed name C. nigricans) (97). This bacterium also hydrolysed tyrosine.
IPCH is a rare dermatological disorder characterized by a change in sweat colour on normal skin due to microorganisms’ pigments. The infectiousness of this disorder has been exemplified in other studies (36, 44) as well as by the current case report. The pigments causing the colour palette seen in this disorder appear to be of major importance for microorganisms. They are a result of evolutionary competition to overcome hosts, other microorganisms, and environmental challenges. Despite determining survival, pathogenicity, and virulence among microorganisms, we hypothesize that most pigments are mainly produced only under favourable conditions (of pH, temperature, hydration levels, metabolism rate, oxygen tension, growth substrates, etc.). This hypothesis is strengthened by the observations found in some of the IPCH case reports.
Castela et al. reported blue skin discolouration due to Bacillus spp. triggered by topiramate (an antiepileptic drug) (38). They recorded a slightly decreased pH on the surface of the skin of their patient and proposed that this could be a result of the treatment provided. Topiramate inhibits carbonic anhydrase isoenzymes, which are also found in kidneys and eccrine glands. Inhibition of this enzyme may alter the primary sweat composition and reduce water formation. The authors also suggested that topiramate reduces aquaporin-5 expression in the skin. Together, these effects could lead to altered sweat pH and hypohidrosis (38). This theory is strengthened by studies indicating that hypohidrosis could be an adverse effect of topiramate (38, 98–100).
Combined use of ranitidine (H2-recepter antagonist) and lansoprazole (proton pump inhibitor) may trigger Bacillus colonization, as reported by Hill et al. (37). The same authors also described resolution of both the blue skin discolouration and the Bacillus spp. overgrowth upon stopping ranitidine. Alongside Hill’s et al., the current case report presents a patient who might be affected by blue Bacillus spp. IPCH following administration of an antihistamine.
Interestingly, our patient’s unspecified hypohidrotic condition could, in fact, have been intensified by the use of promethazine: Zahejsky & Rovensky reported a significant reduction in palmar sweating after administration of promethazine in their clinical study (101). The same authors reported that palmoplantar sweat gland activity is regulated in other neuroanatomical centres (most likely limbic structures) than eccrine sweat gland activity elsewhere on the integument. Promethazine influences these sweat regulatory centres in a way that is not fully understood (101). As sweat production on the hands and feet are similarly controlled, a comparable worsening of hypohidrosis might have been the case at both sites (3). As stated in the methods section, hands and feet were the first regions to show blue-coloured sweat. Whether promethazine is the sole trigger is currently unknown. Pregnancy is another possible trigger. Table II sums up potential triggers of IPCH based on the literature review.
Another important observation in the current case report was that B. cereus colonized and produced pigments in both adults, but not in the newborn. There are documented differences in the pH and hydration between paediatric and adult stratum corneum (102). The lack of discolouration in the newborn may reflect the absence of the specific requisite milieu for this pigment-producing Bacillus spp. to grow or to produce its pigment.
Based on the literature review, bacteriological tests should be the first diagnostic step when dealing with coloured sweat and/or atypical skin discolouration. Oral erythromycin and topical erythromycin/clindamycin appear to be the most effective treatment in both identified and unidentified IPCH (2). If cultures are negative, and antibiotic treatment does not lead to remission of symptoms, an in-depth medical history and broad diagnostic approach are of importance in determining an alternative cause for chromhidrosis.
Table II. Potential triggers of infectious pseudochromhidrosis (IPCH)
The authors thank Dr Maria Ulvestad (Department of Dermatology, Stavanger University Hospital, Stavanger, Norway) for valuable comments.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize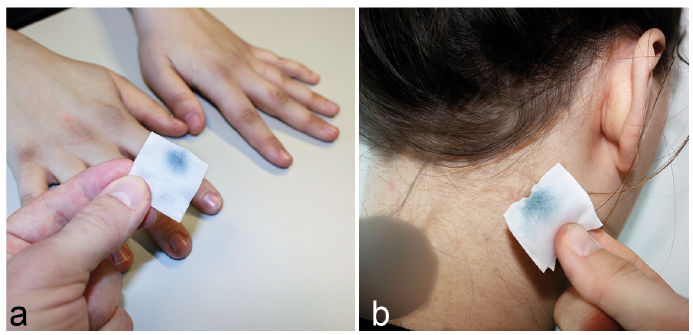 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize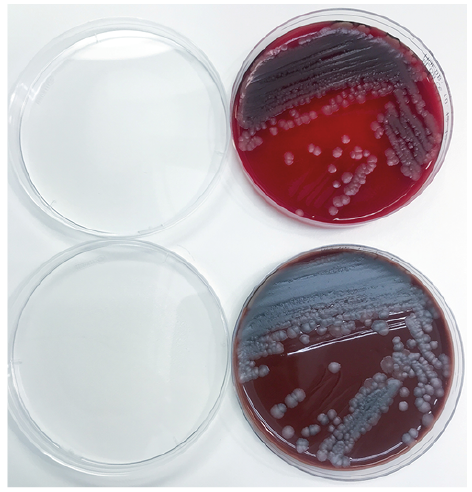 Click to show fullsize
Click to show fullsize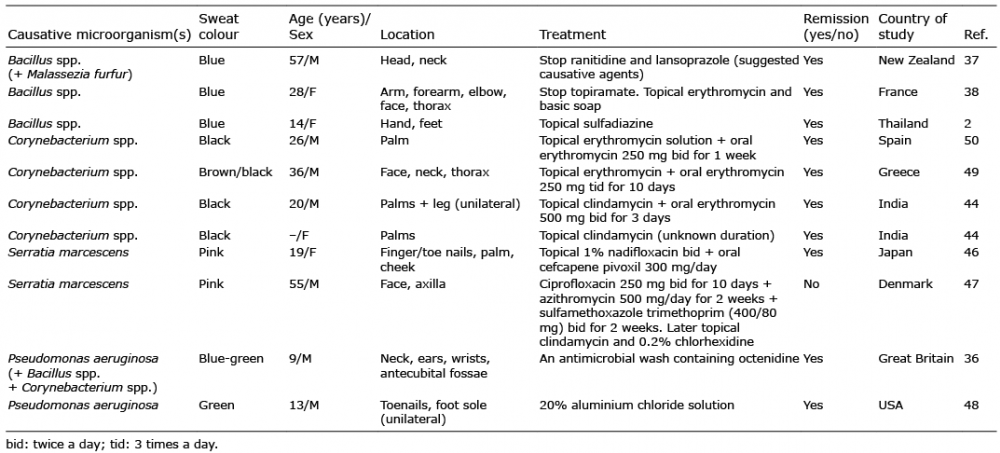 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize