


1Department of Medicine 1, Friedrich-Alexander-University Erlangen-Nürnberg, Erlangen, 2Department of Nephrology, DKD Helios Clinic, Wiesbaden, and 3Occupational Dermatology, Department of Dermatology, Ruprecht-Karls University Heidelberg, Heidelberg, Germany
Chronic itch occurs in many skin diseases, but also in a variety of systemic, neurological, and psychogenic/psychosomatic disorders, or is caused by drug intake. When several diseases or causes co-exist, chronic itch is categorized as “mixed origin”. These patients present with unaltered skin or with chronic scratch lesions including chronic prurigo. Precise diagnostics are necessary to evaluate the underlying aetiology, to enable identification of the best treatment available, and to improve patients’ quality of life. This is of particular relevance in elderly people in whom chronic itch is often of systemic or mixed origin. Xerosis cutis is a frequent cofactor contributing to chronic itch of non-dermatological origin. Treatment is frequently multimodal, considering age, comorbidities, current drug intake, quality and intensity of itch. With regard to the demographic situation of the population, characterized by increasing life expectancy and polypharmacy, itch of non-dermatological origin will represent an increasing medical challenge in the future.
Key words: cholestasis; chronic kidney disease; liver; pruritus; systemic disease; uraemic itch.
Accepted Oct 15, 2019; Published Jan 9, 2020
Acta Derm Venereol 2020; 100: adv00025.
Corr: Andreas Kremer, Department of Medicine 1, Friedrich-Alexander-University Erlangen-Nürnberg, Ulmenweg 18, DE-91054 Erlangen, Germany. E-mail: andreas.kremer@uk-erlangen.de
Itch (medical term: pruritus) is an unpleasant sensation occurring in many skin diseases, but also in a variety of systemic, neurological, and psychogenic/psychosomatic disorders, or is caused by drug intake. These patients usually present with normal-looking skin or chronic scratch lesions of variable degree, including the clinical picture of chronic prurigo. This review focusses on the systemic causes of chronic itch, in particular liver disease, chronic renal failure, haematological disorders and adverse reactions of drug use. Furthermore, a diagnostic approach is presented, and effective, multimodal treatment options for the different systemic causes are summarized.
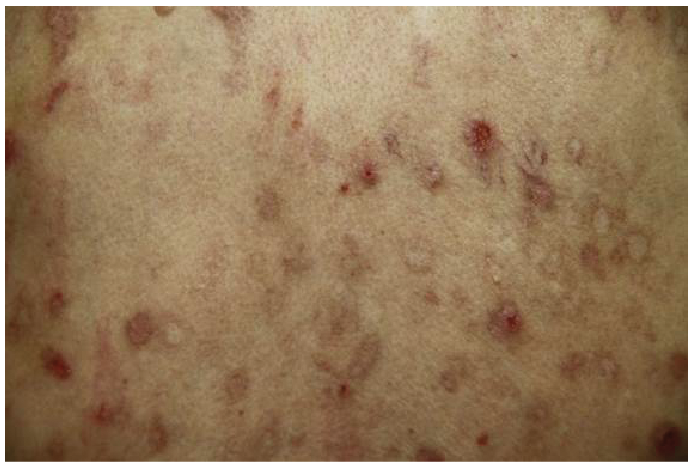
Pruritus or itch is an unpleasant sensation that can evoke scratching even in patients who do not currently have a skin disease. These patients usually present with normal-looking skin or chronic scratch lesions of variable degree, including the clinical picture of chronic prurigo (CPG; Fig. 1). For a long time it was assumed that itching and scratching must be associated with a skin disease. This may result from previous conditions, in which scratching aimed at extracting mites or other skin infestations. It took medical doctors and researchers some time to realize that chronic itch (CI), aside from dermatological disorders, can also be caused by a number of other diseases/origins. This comprises chronic kidney disease, a variety of hepatobiliary, haematological, and endocrine diseases, as well as so-called drug-induced itch (Table I). To date, it is now known to what extent drug intake and, in particular, polypharmacy contributes to CI. The underlying mechanisms of drugs causing pruritus as adverse events are only partially understood, ranging from mainly type-I and type-IV allergy to several other possible mechanisms (1, 2).
Fig. 1. Chronic prurigo on the upper leg in a patient with haemochromatosis.
Table I. Systemic diseases associated with chronic pruritus
Advanced technical and medical care for chronically ill patients prolongs their life expectancy, albeit with an increased number of patients experiencing non-dermatological pruritus. Chronic pruritus further significantly reduces the quality of life in chronically ill patients. These observations represent an important incentive to increase itch research, with the aim of improving medical care for patients with CI with no underlying skin disease (3).
This review summarizes major non-dermatological aetiologies of CI. It also describes neuropathic itch secondary to brain and spinal cord injuries or peripheral nerve damage, as seen in brachioradial itch and notalgia paraesthetica. Finally, this review emphasizes that diagnosis and treatment is challenged in daily clinical routine by the fact that several origins frequently contribute to the occurrence of CI of non-dermatological origin.
Identifying the underlying disease or itch-causing drug often represents a clinical challenge for the treating physician, but is a major need for the affected patient. A recent cohort analysis of more than 3,000 patients with CI illustrated that it occurs mainly in older patients and in those with many comorbidities (4). In contrast to previous doctrines, there is no correlation between generalized pruritus and a systemic disease as underlying cause. Patients with generalized pruritus suffer comparably often from systemic as from dermatological disorders (5). Thus, careful and detailed medical history taking, clinical examination and interdisciplinary, laboratory and radiological diagnostics are of significant importance (6). For this purpose a structured pruritus questionnaire has been developed (7).
Pruritus on primarily affected skin hints at a dermatological disease. In addition to clinical skin investigations, bacterial, mycological, allergic and autoimmune-serological analyses should be performed. Skin biopsy might further help to establish a clinical diagnosis (6). Pruritus on primarily unaffected skin is often caused by systemic, neurological or psychiatric/somatoform disorders or drug intake (8, 9). If medical history taking and clinical examination are inconclusive a step-wise approach for diagnosis is recommended, including various laboratory diagnostics (6).
It should be noted that CI may occur prior to manifestation and/or clinical diagnosis of the underlying disease. This so-called premonitory itch may present up to several years prior to diagnosis, as seen in polycy-themia vera (10).
In rare cases malignancy is responsible for CI (Table I). Two large cohort studies of 8,744 and 12,813 patients with CI without primary skin changes, respectively, unravelled solely increased rates for haematological and bile duct malignancies (11, 12). In case of CI of unknown origin (PUO) the diagnostic approach should focus on these 2 cancer entities. If no underlying diagnosis could be established an annual repetitive work-up may be performed.
Chronic pruritus is commonly reported by many patients with hepatobiliary diseases, in particular those with cholestatic features. Prevalence of hepatic itch varies considerably between the different underlying diseases, with 100% as defining symptom in intrahepatic cholestasis of pregnancy, up to 70% in primary biliary cholangitis, primary and secondary sclerosing cholangitis, 15–45% in benign and malignant biliary disorders, and 5–15% in chronic viral hepatitis C infections (13). Affected patients often report the highest intensity on their limbs, in particular the palms of the hands and the soles of the feet, albeit CI may often be generalized (14). In female patients pruritus typically worsens premenstrually, during hormone replacement, and in the last trimester of pregnancy. Hepatic itch presents independently of the severity of cholestasis or liver function.
The pathogenesis of hepatic itch is not yet fully understood. In the past, bile salts, histamine, progesterone metabolites and endogenous opioids have been discussed as culprits, albeit a correlation with itch intensity could not be established (15). Interestingly, the semi-synthetic bile salt obeticholic acid, which has been licensed for the treatment of primary biliary cholangitis (PBC) dose-dependently worsens pruritus. Recent data have suggested that bilirubin and bile salts may mediate cholestatic itch via the mas-related G protein-coupled receptor X4 (MRGX4), albeit human data supporting this observation is lacking (16, 17). Cholestatic patients do not present with histamine-induced skin alternations, such as erythema, urticaria or wheals, and antihistamines are largely ineffective (18). Recently, lysophosphatidic acid (LPA) and its forming enzyme autotaxin (ATX) have been identified as potential mediators of hepatic itch (19). However, drugs inhibiting the ATX-LPA axis have not yet been investigated in hepatic itch to prove this pathophysiological concept.
Treatment should focus primarily on adequate therapy for the underlying hepatobiliary disease, which may result in relief of hepatic itch. In this regard, itch due to obstruction of the extrahepatic biliary tree is often efficiently ameliorated by endoscopic biliary stenting, transcutaneous or nasobiliary drainage. In contrast, itch due to intrahepatic cholestasis may represent a significant clinical challenge.
Ursodeoxycholic acid (UDCA) is used as anticholestatic baseline treatment in many cholestatic disorders, such as PBC, primary sclerosing cholangitis, and intrahepatic cholestasis of pregnancy (20). UDCA is a safe and effective anti-pruritic therapy in women with intrahepatic cholestasis of pregnancy (21). However, in randomized placebo-controlled trials UDCA did not significantly improve itch intensity. Topical treatment with rehydrating and cooling (e.g. menthol-containing) ointments may mitigate hepatic itch if mild in intensity. If insufficient, cholestatic itch is recommended to be treated with cholestyramine (4–16 g/day) as first-line therapy, followed by rifampicin (150–600 mg/day), naltrexone (25–50 mg/day) and sertraline (75–100 mg/day) according to the current guidelines (13, 20) (Table II). Bezafibrate or fenofibrate may be used as alternative approaches (22, 23). Future therapies could be based on inhibitors of the ileal bile acid transporter (IBAT) in the terminal ileum, which are currently investigated in placebo-controlled trials (24). In refractory cases invasive procedures, such as plasmapheresis, albumin dialysis (e.g. MARS®, Prometheus®), transcutaneous or nasobiliary drainage, may be performed. After liver transplantation most patients experience relief of CI.
Table II. Therapeutic recommendations for hepatic pruritus
Itch in renal disease, also referred to uraemic pruritus (UP), affects patients with advanced stages of chronic kidney disease (CKD), mostly those on dialysis. Epidemiological studies indicate that up to 50% of patients on haemodialysis have CKD-associated pruritus (CKD-aP) depending on the investigated country (25, 26). The underlying pathological mechanism remains elusive. Increased levels of uraemic toxins and parathormone, as well as xerosis and subclinical skin inflammation have been suggested to play a role in the pathophysiology. Furthermore, the endogenous opioid system may play a role, possibly through upregulation of µ-opioid and/or downregulation of κ-opioid activity (27). This may, at least partially, explain the efficacy of μ-opioid antagonists and κ-opioid agonists in the treatment of CKDaP. Recent experimental data suggested central neuropathic and neuroplastic changes in patients with CKD-aP, which may explain the good response to calcium-channel-blockers in these patients (28).
CKD-aP greatly impacts the quality of life of affected patients (25). Retrospective analyses identified risk factors for UP in dialysis patients even before dialysis has begun. These include male sex and certain comorbidities, such as congestive heart failure, chronic hepatitis C virus infection, neurological diseases, depression and higher serum calcium/phosphorus levels (29). When uraemic itch occurs, skin appearance is normal in most patients, except for common changes in skin colour and a frequently observed xerosis. Scratch lesions, such as excoriations with or without impetigo, may be observed in some patients and, in some cases, chronic prurigo (Fig. 1). Medical therapy for CKD-aP remains a clinical challenge. Emollients for skin care and hydration are essential. In early stages gabapentin and pregabalin, although not licensed for this indication, may be helpful (30). Ultraviolet phototherapy may ameliorate itch in uraemic patients (31). Detailed information about drugs and dosages is given in Table III.
Table III. Therapeutic recommendations for chronic kidney disease associated pruritus
Neuropathic itch is caused by neuronal or glial damage to peripheral neurones, either localized (e.g. nerve compression) or generalized (e.g. nerve degeneration). Damage to the central nervous system, such as by tumours of the brain or in the spinal cord, rarely causes pruritus.
Several entities can be discerned. Patients with notalgia paraesthetica (NP) perceive itch in the subscapular region, associated with a slightly painful or burning character. The pathophysiology of this entity is unclear, but NP is presumed to be a mononeuritic disease affecting thoracic nerve fibres. Patients with brachioradial itch have localized itch within the dorsolateral parts of the forearms and, less frequently, around the shoulders. As in NP, patients report mixed itch and pain sensations. Cervical cord compression or radiculopathies have been observed in these patients (32).
The small fibre neuropathy is a systemic neuropathy of peripheral nerves accompanied by severe pruritus in some patients. This sensory disorder leads to a variety of symptoms, including pain, tingling, numbness, deranged thermoregulation and signs of malfunction of the autonomic nervous system, such as gastrointestinal dysmotility and orthostatic hypotension. The diagnosis is difficult to establish, requiring thermoregulatory sweat testing and skin biopsy with reduced small fibre density (33).
Apart from these entities, neuropathic itch may occur in the course of herpes zoster infections as so-called post-herpetic itch, polyneuropathies and scars induced by trauma or burns.
Treatment of neuropathic itch is difficult. Local treatment with capsaicin or systemic treatment with calcium-channel-blockers, such as gabapentin or pregabalin, may alleviate pruritus (3, 34).
CI may occur in association with several endocrine diseases. Whether patients with diabetes mellitus are more frequently afflicted than those without remains a matter of debate. In one study investigating almost 400 patients with diabetes 27.5% reported on generalized itch (35). In another study truncal itch was most prominent in diabetic patients. Of 2,656 patients with diabetes mellitus, 11.3% reported itch located on the trunk, whereas this symptom was present in only 2.9% of 499 age-matched patients without diabetes (36). Further endocrine diseases associated with the occurrence of CI include Grave’s disease and multiple endocrine neoplasia type II.
Itching is commonly reported in patients with haematological diseases. Aquagenic pruritus is a typical feature in many of these patients, with a pungent itchy character after contact of the skin with water. Polycythaemia vera is a rare myeloproliferative disease with a clonal dysfunction of pluripotent hematopoietic cells. Affected patients report itch in 30–65% of cases. Aquagenic itch is most commonly observed in patients with a homozygous JAK2 617V mutation (37). Inhibitors of the JAK-STAT pathway, such as ruxolitinib, strongly attenuated pruritus in addition to improving the underlying disease (38, 39). Similarly, patients with essential thrombocytosis and primary myelofibrosis often report aquagenic itch.
Hodgkin’s disease belongs to the class of B-cell lymphoma. CI on primarily unaffected skin is reported by 15–50% of patients (40). Severe itch may precede the outbreak of the disease by many years. CI worsens at night, often starts at the lower limbs, and may generalize. After successful anti-tumour therapy, CI may also indicate a relapse of Hodgkin’s disease. In patients with non-Hodgkin lymphoma pruritus may affect up to 30% of patients. In leukaemia patients CI is more commonly observed in lymphatic compared with myelocytic leukaemia and in chronic compared with acute forms. Recommended therapy consists of the calcium channel blockers gabapentin (300–2,400 mg/day) and pregabalin (75–600 mg/day), acetylsalicylic acid (300 mg/day) and mirtazapine (7.5–30 mg/day) (Table IV) (6).
Table IV. Therapeutic recommendations for pruritus of hematopoietic origin
In daily clinical practice the term “paraneoplastic itch” (PI) is used to describe itch in patients with cancer. Itch caused by haematological diseases is described above. In general, PI is considered as a rare disorder. It occurs most commonly in lymphoreticular malignancies, while being rarely reported in patients with solid tumours. Its true frequency remains unknown, as epidemiological data is limited. This may mainly be due to other symptoms receiving more attention and being regarded as more important in cancer patients with paraneoplastic diseases. According to the literature and our own clinical studies CI further impairs quality of life in patients with malignant diseases. In 2012, an interdisciplinary study interest group (SIG) of physicians and researchers was founded, with the aim of generating a clear definition of PI (40).
Previously, several terms have been used to describe the different types of paraneoplastic itch. The SIG states that the term paraneoplastic itch should be used in case itching occurs as a systemic, but not local, reaction in the presence of a solid tumour or haematological malignancy. This term excludes itch induced either by the local invasive growth of cancer cells or by anti-tumour therapy. PI usually disappears with remission of the tumour and may return with its relapse (40).
Diagnosing PI represents a clinical challenge, as it remains difficult to exclude other aetiologies and reasons for CI, such as paraneoplastic skin diseases, skin or non-dermatological diseases occurring in chronically ill patients, as well as adverse drug reactions. The mechanisms of PI are still not understood.
In daily clinical practice the term “paraneoplastic itch” (PI) is used to describe itch in patients with cancer. Itch caused by haematological diseases is described above. In general, PI is considered as a rare disorder. It occurs most commonly in lymphoreticular malignancies, while being rarely reported in patients with solid tumours. Its true frequency remains unknown, as epidemiological data is limited. This may mainly be due to other symptoms receiving more attention and being regarded as more important in cancer patients with paraneoplastic diseases. According to the literature and our own clinical studies CI further impairs quality of life in patients with malignant diseases. In 2012, an interdisciplinary study interest group (SIG) of physicians and researchers was founded, with the aim of generating a clear definition of PI (40).
Previously, several terms have been used to describe the different types of paraneoplastic itch. The SIG states that the term paraneoplastic itch should be used in case itching occurs as a systemic, but not local, reaction in the presence of a solid tumour or haematological malignancy. This term excludes itch induced either by the local invasive growth of cancer cells or by anti-tumour therapy. PI usually disappears with remission of the tumour and may return with its relapse (40).
Diagnosing PI represents a clinical challenge, as it remains difficult to exclude other aetiologies and reasons for CI, such as paraneoplastic skin diseases, skin or non-dermatological diseases occurring in chronically ill patients, as well as adverse drug reactions. The mechanisms of PI are still not understood.
Baseline therapy of PI comprises the treatment of the underlying malignancy. In many cases, cytoreductive therapies are effective. There are no randomized controlled trials (RCTs) for the treatment of PI, which may be explained largely by the rarity and diversity of PI. Topical therapies, including cooling agents, may lead to symptomatic relief. H1-antihistamines are mostly ineffective. PI in lymphoma can improve with oral prednisone (see above) acting via different mechanisms, and longer systemic treatment with prednisone may be considered in PI (3). Serotonin reuptake inhibitors (SSRI), such as paroxetine, up to 20 mg daily, calcium alpha (2)-γ-channel blockers, such as gabapentin and pregabalin, can be used for treating PI as well as thalidomide 50–200 mg daily. Opioid receptor antagonist, such as naloxone (0.8–2 mg i.v./day), naltrexone (50–100 mg/day orally) or neurokinin (NK)-1-receptor-antagonists, e.g. aprepitant, have been used for itch, for example in T-cell lymphoma, solid tumours and itch-related biological cancer treatment (40). It should be considered that patients with cancer frequently receive analgetics that may induce CI as a side-effect.
Itch associated with systemically or locally applied drugs is a common phenomenon (41). Almost every drug may cause localized or generalized itch. Drug-induced itch may emerge as a hypersensitivity reaction towards the drug or, as in many cases, due to another, mostly unknown, pathophysiological process. There is evidence that, with some drugs, the MRGX2-receptor is activated, resulting in a different release of pruritogenic compounds than in IgE-mediated hypersensitivity reactions (42). Identifying the responsible compound remains, for many cases, a clinical challenge, as many patients are taking multiple drugs and there might be a considerable delay between the start of drug intake and the development of itch.
Chloroquine, which is mainly used as an antimalarial drug, can induce itch, probably by activating the MrgprX1-receptor. Interestingly, chloroquine provokes itch mainly in black Africans, while Caucasians are less commonly affected potentially by a strong binding capacity to melanin with significantly higher skin concentrations in Africans (43).
Itching provoked by hydroxylethyl starch (HES) infusion is thought to be caused by HES depositions in peripheral nerves (44). Treatment is cumbersome and mostly frustrating (45).
Opioidergic drugs may cause strong itch, especially when applied epidurally or intrathecally (46) which may be mediated by activation of the isoform D of the μ-opioid receptor (47). It can be treated effectively by µ-receptor-antagonists, such as naloxone.
Along with the expansive development and use of targeted tumour therapies, numerous reports have emerged about therapy-associated chronic pruritus (48–52). The neurokinin-1-antagonist aprepitant seems to have antipruritic potential in such cases (53).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize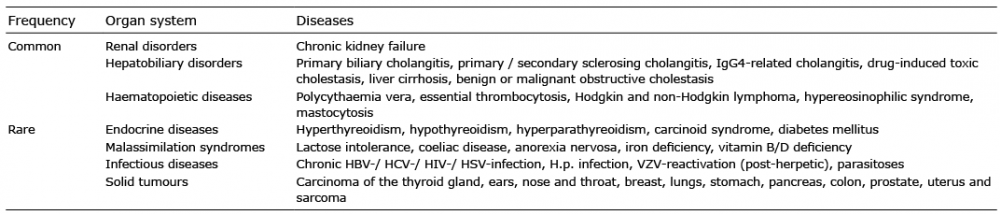 Click to show fullsize
Click to show fullsize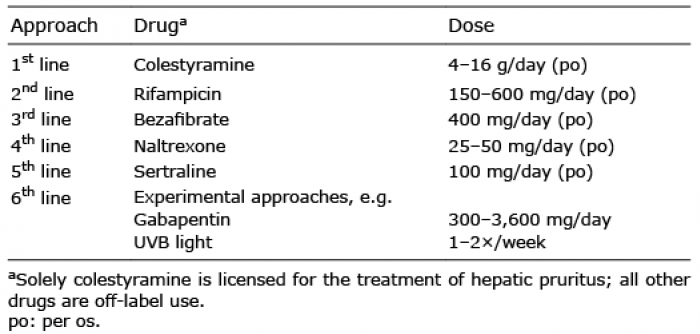 Click to show fullsize
Click to show fullsize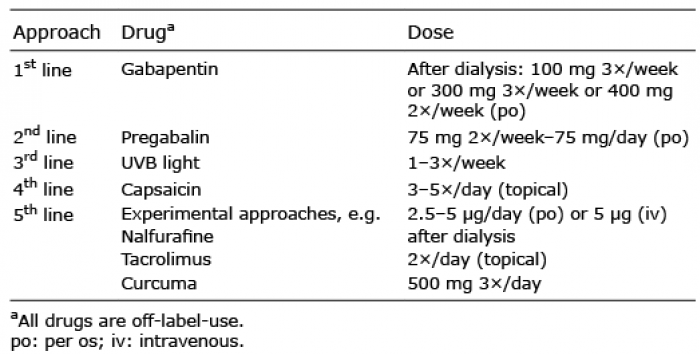 Click to show fullsize
Click to show fullsize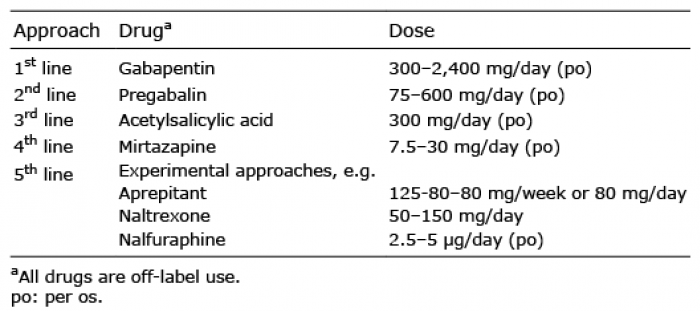 Click to show fullsize
Click to show fullsize