


1Department of Dermatology and 2Division of Rheumatology and Clinical Immunology, University Medical Center of the Johannes Gutenberg University Mainz, Mainz, and 3Division of Sleep Medicine, Center for Psychiatry, Psychosomatic and Psychotherapy, Pfalzklinikum Klingenmünster, Klingenmünster, Germany
This study examined the relationship between insomnia and the frequent itching skin diseases, atopic dermatitis and chronic urticaria. Patients with chronic inflammatory dermatological diseases with pruritus were evaluated for insomnia (Insomnia Severity Index; ISI) and impairment in dermatological quality of life (Dermatology Life Quality Index; DLQI). Disease activity was measured using validated scores. A total of 61 patients participated in the study. Patients with atopic dermatitis had a mean ISI score of 8.7 before flares and 16 when a flare occurred. The mean DLQI score in atopic dermatitis was 11.4. The mean ISI score in patients with chronic urticaria was 6.8 before flares and 14.9 when a flare occurred. In patients with chronic urticaria the mean DLQI score was 8.5. An increase in insomnia during a disease flare was demonstrated in both groups. Thus, sleep is a factor to consider during treatment of itching skin diseases. The results of this pilot study indicate that pruritus may not be the only reason for insomnia in patients with atopic dermatitis or chronic urticaria.
Key words: sleep disturbance; urticaria; atopic dermatitis; insomnia; quality of life.
Accepted Jan 28, 2020; Epub ahead of print Feb 4, 2020
Acta Derm Venereol 2020; 100: adv00073.
Corr: Caroline Mann, Dermatology, Johannes-Gutenberg Universtity, DE-55131 Mainz, Germany. E-mail: caroline.mann@unimedizin-mainz.de
Interactions between sleep and skin diseases are considered clinically relevant. Quality of sleep can positively or negatively influence the course of skin diseases. However, the impact of the interaction between dermatological diseases and sleep disturbance, especially with regard to chronicity, remains to be elucidated. The aim of this pilot study was to identify possible interactions between sleep disturbance and skin diseases, which may be an underestimated aetiopathological aspect.
Insomnia is the most common sleep disturbance among the general population, with an incidence of 10–20% (1). Although the pathophysiology of insomnia is diverse, its definition involves the following aspects: difficulty falling asleep, staying asleep, waking up early or a lack of sleep despite opportunities to sleep (2). Insomnia can be a symptom, or even a cause of other underlying medical disorders and may lead to an increase in interleukins (3). Individual assessment of insomnia is often divergent from the measurement of actual sleep deprivation by polysomnography (1).
Atopic dermatitis (AD) is a common inflammatory skin disease, which affects almost 3% of the German population in adulthood (4, 5). AD is multifactorial and can be triggered by various endogenous and exogenous stimuli. The reaction of different skin types to environmental triggers varies. An individual’s skin barrier dysfunction seems to play a key role, making the skin more vulnerable to environmental damage (6). Hormonal fluctuations, psychological stress, infectious diseases and further more triggers influence the condition of the skin (6). Alteration of the skin texture is often the first sign of an underlying medical problem. Early inflammation of the skin is TH2 driven and becomes TH1 driven when chronic and maintained by various interleukins (7, 8).
Urticaria, also known as hives, is defined as the spontaneous appearance of itching wheals and angioedema (9, 10). Almost 20% of the German population is affected by urticaria, lasting less than 6 weeks, at least once in their lifetime. Approximately 5% of the affected people experience urticaria for longer than 6 weeks and therefore have chronic urticaria (CU) (9). The cause of urticaria is heterogeneous, but it is mainly regarded as a mast-cell driven reaction (10).
Although itching skin disease in the general public is associated with poor sleep quality, little research has been done to better understand insomnia-associated oxidative stress and its impact on inflammatory skin diseases. This was the topic of the current investigation.
Questions about insomnia are routine when taking a medical history of dermatological patients, although this subject has not received particular attention. It is known that patients with sleep disturbance have an increased risk of cardiometabolic disease, which is associated with vascular events such as stroke, coronary artery disease and myocardial infarction, but also with obesity, impotence and depression (11, 12). In many aspects this influence is bidirectional. Insomnia has a significant impact on quality of life (QoL) as well as daytime functioning, and is especially common in elderly people. Moreover, patients with insomnia have reduced resistance to pain (13). These wide-ranging effects provide evidence to support a correlation between skin diseases and insomnia. The aim of this study was to elucidate to what extent insomnia influences the disease process in dermatological diseases with pruritus.
Population and procedure
This was a paper and pencil questionnaire-based cohort study, lasting from September 2018 to February 2019 in the dermatology department of the University Medical Center in Mainz, Germany. Sex, age and body mass index (BMI) were registered for all patients. Disease diagnosis was based on clinical manifestation and validated scores for CU and Hanifin & Rajka criteria for AD (14).
All subjects provided written consent to participate in the survey. In order to increase the level of anonymity of the survey, collection of personal data was reduced to a minimum. The study design was reviewed by the ethics committee of the state of Rhineland-Palatinate, Germany.
Disease activity
For patients with AD, disease severity was evaluated using the Eczema Area and Severity Index (EASI; score 0–72, where 0 indicates no skin manifestations and 72 indicates strong infiltration, erythroderma, xerosis and excoriations), rated by the physician. A flare was defined by an increase of 6–7 points in the EASI (15).
For patients with CU, the Urticaria Control Test (UCT) was used (score 0–16, where ≥ 12 indicates disease control) and the Urticaria Activity Score (UAS7; score 0–42, where 0–6 indicates well-controlled urticaria with no activity and 42 indicates severe activity). The UCT and UAS7 scores evaluate disease activity and are both patient-rated. In the UAS7 activity is assessed for 7 consecutive days, asking about number of wheals (score 0–3) and pruritus intensity (score 0–3), whereas the UCT (0–16) asks about physical symptoms, QoL, treatment efficacy and urticaria control (16), which was defined by newly appearing objective symptoms like hives during the previous 7 days.
Patient-reported outcomes
The Insomnia Severity Index (ISI) is a validated 7-item questionnaire in which patients rate their current quality of sleep in order to assess the extent of insomnia. The ISI was developed in English and translated into various languages. The German version of the ISI was validated by Gerber et al. in 2016 (17).
The Dermatological Life Quality Index (DLQI) is a commonly used 10-item questionnaire with a range of 0–30, which measures the impact of different skin diseases on QoL during the previous week. A score ≥ 10 indicates severely impaired QoL (18).
To measure current pruritus severity patients were asked to rate their itch on a visual analogue scale (VAS) from 1 (no itch) to 10 (unbearable itch). An itch score ≥ 4 was rated significant (19).
Statistical analysis
All data were assessed for normal or non-normal distribution. Differences in disease scores were determined using Mann–Whitney U test and or Student’s t-test with reference to the distribution of the calculated variables. Correlations were determined using Spearman’s rho correlation analysis. The level of significance was set at α = 0.05. The resulting p-values were considered nominally significant at p < 0.05. Statistical analyses were calculated with SPSS PASW23 Statistics (IBM Corp., Somers, NY, USA).
Demographics
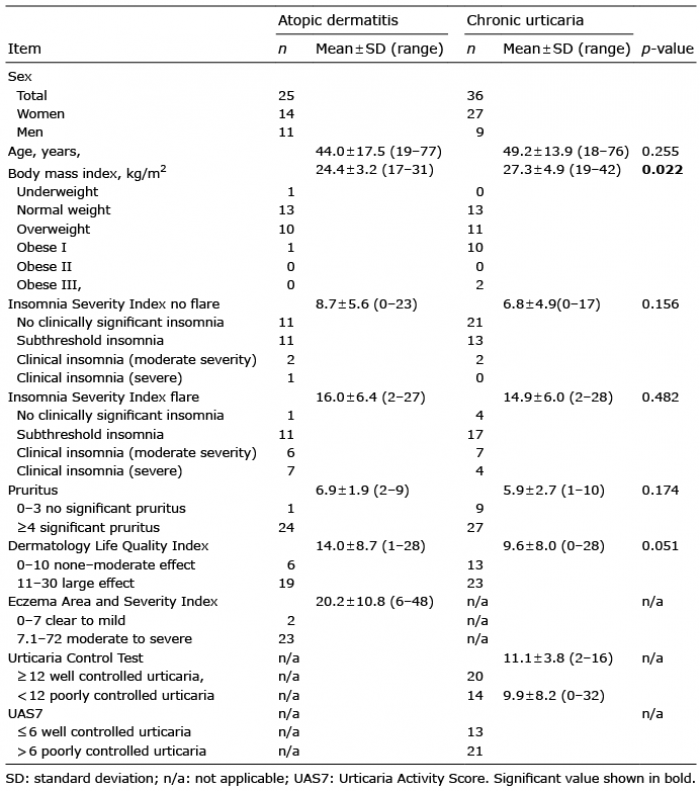
A total of 61 patients (20 males, 41 females) were included; 25 with AD, and 36 with CU, including all subtypes (Table I). All patients were asked to complete the ISI questionnaire on admission. In addition, they rated their insomnia before the onset of the current flare, even though the questionnaire is usually used only to determine current sleep quality. The patients’ ages ranged from 18 to 77 years, with a mean of 44.0 ± 17.5 years for patients with AD and 49.2 ± 13.9 years for patients with CU. The BMI ranged from 17 to 42 kg/m2, with a mean of 24.4 ± 3.2 kg/m2 in AD and 27.3 ± 4.9 kg/m2 in CU. For AD 14 persons were not overweight, whereas 11 had a BMI > 24.9 kg/m2. Only 13 patients in the CU group were of normal weight, while 23 were overweight (BMI > 24.9 kg/m2). The BMI was calculated according to WHO criteria (20).
Table I. Descriptive characteristics of the studied groups
Disease activity
For patients with AD the mean EASI score (physician rated) was 20.2 ± 10.8. For patients with CU the mean UCT was 11.1 ± 3.8 and the mean UAS7 9.9 ± 8.2 (both patient rated). All patients experienced itch to a different level and as a main symptom during a flare. The pruritus score showed a mean score of 6.9 ± 1.9 for patients with AD and 5.9 ± 2.7 for patients with CU, respectively. The mean DLQI during a flare was 14.0 ± 8.7 in patients with AD and 9.6 ± 8.0 in patients with CU. There were no significant differences between the 2 groups, except for BMI, which was higher in patients with CU (p = 0.022). The p-value of the DLQI, at p = 0.051, was close to significance for both patients with AD and those with CU.
Insomnia Severity Index
The ISI score was 8.7 ± 5.6 before a flare in patients with AD and 6.8 ± 4.9 in patients with CU, and during a flare increased to 16 ± 6.4 for patients with AD and 14.9 ± 6.0 for patients with CU. Insomnia was pre-existing in 6 patients with AD and in 12 with CU. Significant change in the ISI score was found in both groups before and after treatment (p > 0.001). More detailed insomnia during a flare was also subtyped by the predominant symptoms, as shown in Table II. Thus, 16 patients with AD (2.1 ± 1.4) and 9 with CU (1.7 ± 1.3) had ”problems falling asleep”, 12 patients with AD (2.2 ± 1.5) and 17 with CU (2.3 ± 1.3) had ”problems maintaining sleep”, and 8 patients with AD (1.8 ± 1.4) and 15 with CU (2.0 ± 1.3) had ”problems with waking up too early”. Only 8 patients with AD (2.9 ± 0.9) and 16 patients with CU (2.4 ± 1.1) were satisfied ”with their sleep pattern”. A total of 16 patients with AD (2.2 ± 1.1) and 29 with CU (1.7 ± 1.2) reported that their “sleep problems were not noticeable by others”. Eleven patients with AD (2.3 ± 1.2) and 15 with CU (2.3 ± 1.1) were worried about their sleep. “Interference with daily functioning” caused by insomnia was reported by 17 patients with AD (2.7 ± 1.0) and 20 patients with CU (2.5 ± 1.0), respectively. The sub-scores did not any show differences between the 2 groups (p > 0.05).
Focusing on age and anthropometrical parameters, correlations were found between age and ISI score (p = 0.036) and between age and UCT score (p =0.024); hence, older age leads to a lower UCT score. In addition, a correlation was found between higher weight and lower DLQI (p = 0.035).
No significant correlations were found between ISI flare and pruritus score, or between UCT, UAS7 and ISI scores. No significant interaction was found between BMI and ISI score during a flare in either group of patients.
Table II. Descriptive characteristics of the Insomnia Severity Index
The correlations between relevant variables for both disease groups are shown in Table III. In the AD group there was a positive correlation between ISI flare score and DLQI score (p = 0.017), and between ISI flare and EASI score (p = 0.032). There was a significant correlation between DLQI score and pruritus score (p = 0.020), whereas no significant correlation was found between ISI and pruritus scores. No other parameters were statistically significant in patients with AD.
In patients with CU during a flare correlations were detected between ISI and DLQI scores (p = 0.029) and between pruritus score and DLQI score (p > 0.001).
Table III. Correlations of the relevant variables for both diseases
In patients with AD when focusing on the 7 subscores of the ISI during a flare (Table IV), a significant correlation was found between DLQI score and “difficulties falling asleep” (p = 0.007). Being “worried about sleep” (p = 0.003) and “interference with daily functioning” (p = 0.017) correlated significantly with the DLQI score. “Difficulties staying asleep” was associated with an increased EASI score (p = 0.014). Younger patients reported, that their “sleep problem was noticeable to others in terms of impaired QoL” (p = 0.010).
In patients with CU, “waking up too early” was correlated with DLQI score (p = 0.012). Patients with CU with a higher DLQI score (p = 0.003) and a higher pruritus score (p = 0.018) were less satisfied with their sleep pattern. “Interference with daily functioning” was reported by patients with CU with a lower DLQI (p = 0.040). Patients who were “worried about sleep” had a higher UCT score (p = 0.022). In younger patients “difficulties staying asleep” (p = 0.039), and “interference with daily functioning” (p = 0.026) were noticed. Furthermore, younger patients found that their “sleep problem was noticeable by others” (p = 0.005).
Table IV. Correlations with the subscales of the Insomnia Severity Index for both diseases
Insomnia is a well-known phenomenon worldwide, which is thought to play an important role in increasing disease activity in inflammatory and itching skin diseases.
This pilot study revealed an association between insomnia and disease activity by evaluating sleep disturbances in 2 different skin diseases. The results demonstrate that disease severity in AD, measured by the EASI score, influences sleep quality. Examining the individual questions of the ISI, a high EASI score, and therefore a high disease activity, was associated with interrupted sleep. This could be explained by subconscious itching during the night, as is often reported by patients’ partners. However, the UCT and UAS7 did not show a correlation between UCT and UAS7 score with insomnia severity. However, a significant difference was seen in ISI scoring before and during a disease flare. This suggests that the UCT and UAS7 instruments are not sufficiently strong to reflect the influence of sleep disturbances. Nonetheless, the sub-score of the ISI “worried about sleep” correlated significantly with the UCT score in patients with CU and showed that impaired sleep has an effect on perception of disease severity in patients with CU.
Although the DLQI did not ask specifically about insomnia, the results of this study show a correlation between insomnia severity and quality of life. Moreover, questions about sleep quality in the ISI revealed a significant correlation with the DLQI (Table IV). In patients with AD “difficulties falling asleep” had a higher correlation with DLQI score. In patients with CU, QoL was more affected by early awakening. This emphasizes the relevance of sleep disturbances on daily functioning in each individual and shows consistency and interaction between the parameters surveyed. Although insomnia is more common in the older population (21), the current study did not find any correlation between advanced age and ISI score. In contrast, the results revealed difficulties staying asleep and interference with daily functioning especially in younger patients with CU. In both groups, but especially in patients with CU, younger patients seemed to be troubled by impaired sleep. This association was also found in other studies dealing with the assessment of QoL in adolescents with insomnia (22). The current study showed that patients with AD and those with CU have different manifestations of sleep disturbances, although both AD and CU are inflammatory diseases with pruritus as a main symptom. However, in both diseases the relevance of insomnia with regard to QoL is manifested.
Recent studies have examined skin diseases and insomnia (23–25). With psoriasis, for example, itch and pain appear to affect both QoL and sleep (26). Patients with AD or psoriasis were scanned for insomnia, demonstrating that, with AD, there was a higher level of insomnia compared with patients with psoriasis (24). This was explained by pruritus. Likewise, the current study showed that 25 patients with AD appeared to be more affected by insomnia than those with CU. The current study showed that the more the patients were affected by pruritus, the higher was the impact on their QoL. This was also confirmed when examining the ISI sub-scores. Patients with CU with a higher pruritus score were less satisfied about their sleep pattern. Interestingly patient-rated insomnia itself did not increase significantly with pruritus. Unlike other studies, we were unable to identify itch as the most reliant predictor for sleep impairment (23, 26). This means that there must be additional relevant factors for poor sleep in this group of patients. The BMI did not have an impact on the outcome of the ISI in this cohort, therefore obstructive sleep apnoea could be ruled out as potential bias. One possible explanation for insomnia in AD could be impaired thermoregulation during sleep and fluid loss due to decreased skin barrier function (6).
CU can be subdivided into different subgroups; how-ever, this pilot study focussed on sleep as the primary endpoint. In contrast to patients with AD, those with CU did not show permanent symptoms and were exposed to specific triggers during the course of the day. The level of histamine release increases in the evening and again in the early hours of the morning, which could explain the higher rating of the question “problems waking up too early” in patients with CU (27). Our results show that, even with a low UAS7 score in patients with CU, which also includes a rating of pruritus severity (16), clinically significant insomnia was observed during a flare. The pruritus documented in the UAS7 score, might vary between patients, as it is known, that some subjects document their worst pruritus during the day, while others document their mean pruritus intensity (28). In addition, symptoms of angioedema are not included in the UAS7, but might contribute to insomnia and explain the high ISI score (29).
The amount of research into intensive pruritus reflects its relevance and need for further workup. However, insomnia has similar psychological and physiological effects and is enhanced by pain (23). It is known that insomnia increases the risk of metabolic syndrome, hyper-tension, coronary artery disease and depression (1). On a molecular level, initial studies show an association between poor sleep and an increase in pro-inflammatory cytokines, such as TNF alpha and interleukin-6, both playing an important role in inflammatory skin diseases, such as AD and CU (3, 30). Moreover, an increase in reactive oxygen species, due to sleep disturbance, has been shown to be of relevance in the pathogenesis of inflammatory skin diseases, such as AD and CU (31–33).
It remains to be elucidated how much cytokines are elevated during sleep deprivation in patients with skin disease. Sleep deprivation has been shown to result in cortisol release (34). Cortisol has various effects and is known to have a negative influence on skin barrier function and homeostasis (35). Nerve growth factor, for example, is increased in chronic stress, as seen in patients with sleep deprivation. This NGF results in increased inflammation and skin thinning (34). Sleep deprivation leads to a diminished skin barrier function (36, 37).
The current study indicates that there is a high likelihood of sleep disturbance in patients with AD and those with CU. In particular, patients with AD experienced poor sleep during acute episodes. Sleep was less affected in patients with CU. In contrast to other studies, the current results indicate that pruritus is not the only reason for insomnia in patients with AD and those with CU, and further research is needed. The current pilot study indicates that patients with dermatological diseases have different manifestations of sleep disturbance and should therefore be individually assessed, as each sleep disturbance may mandate a different treatment. The current study showed that sleep disturbances are indeed an underestimated burden among patients with dermatological diseases and should be considered and treated in patients with AD and CU in order to improve outcomes.
The authors would like to thank the team at the clinical research centre for their help with survey data collection, and all of the participating patients.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize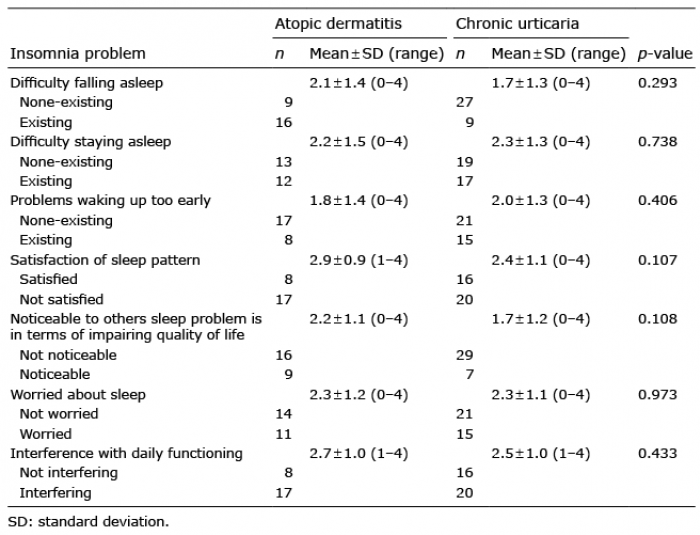 Click to show fullsize
Click to show fullsize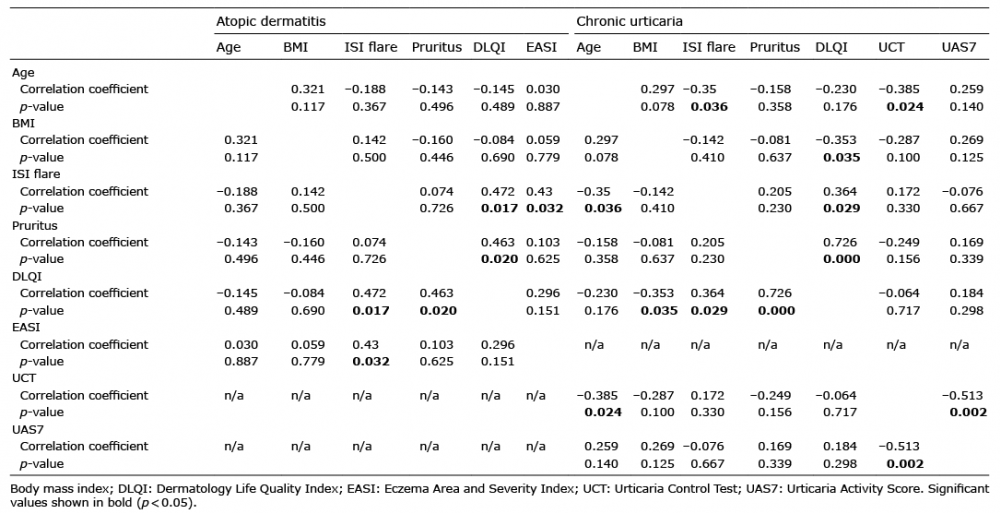 Click to show fullsize
Click to show fullsize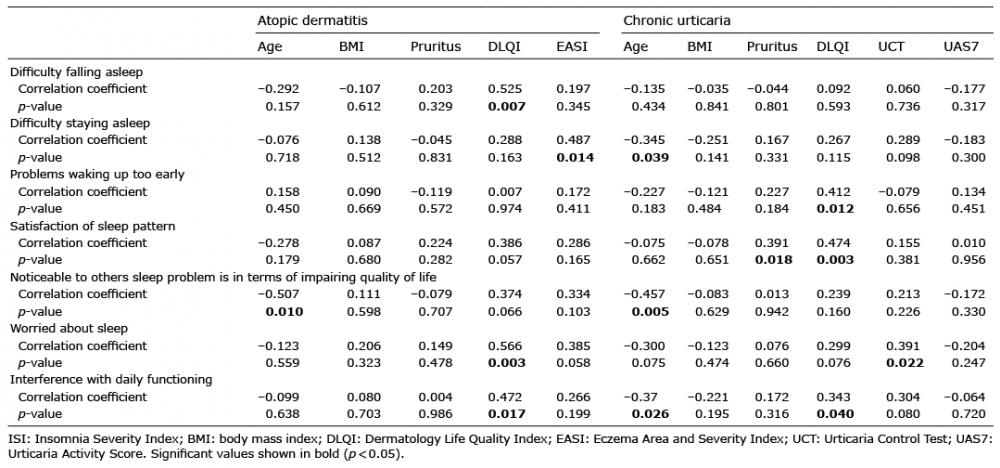 Click to show fullsize
Click to show fullsize