


1Department of Public Health and Primary Care, Brighton and Sussex Medical School, Brighton, UK, 2Medical Sociology, Institute of Epidemiology and Preventive Medicine, University of Regensburg, Regensburg, 3Institute of Social Medicine and Health Systems Research, Otto von Guericke University Magdeburg, Magdeburg, Germany, 4Lee Kong Chian School of Medicine, Nanyang Technological University Singapore, Singapore, and 5Consultant Dermatologist, Dermatology Outpatient Department, Brighton General Hospital, Elm Grove, Brighton, UK
Little is known about which quality of life measure best captures the lived experience of people with a chronic skin condition. The purpose of this study was to explore patients’ views on the Dermatology Life Quality Index (DLQI) and Skindex-29. Participants were adults (n = 28) with a diagnosis of eczema or psoriasis who completed the DLQI and the Skindex-29 before being interviewed about the content and format of these questionnaires. Interviews were analysed using content analysis. Participants were generally satisfied with length and layout of both questionnaires. However, the majority preferred the Skindex-29 for its ease of understanding, use of a longer recall period and incorporation of items on a variety of emotions. Participants reported both questionnaires failing to incorporate important aspects of their lives, for instance impact on professional relationships. Participants voiced limitations in both measures but overall felt Skindex-29 better captured their lived experience.
Key words: quality of life; DLQI; Skindex-29; qualitative study; content validity; lived experience.
Accepted Jan 28, 2020; Epub ahead of print Feb 5, 2020
Acta Derm Venereol 2020; 100: adv00105.
Corr: Prof Christian Apfelbacher PhD, Institute of Social Medicine and Health Systems Research, Otto von Guericke University Magdeburg, Leipziger Str. 44, DE-39120 Magdeburg, Germany. E-mail: christian.apfelbacher@med.ovgu.de
People with chronic skin conditions often experience impairments in their quality of life. Several questionnaires exist for measuring quality of life in skin disease, e.g. the Dermatology Life Quality Index (DLQI) and Skindex-29. In this study we asked 28 patients with eczema or psoriasis to what degree these two measures capture what matters to them. Overall, the patients felt that Skindex-29 better captured their lived experience due to its items on emotions, a longer recall period of 4 weeks and greater ease of understanding. However, both DLQI and Skindex-29 lack important content such as impact of disease on professional relationships.
In any one-year, more than half of the UK’s population (54%) experience a skin disorder (1). Skin conditions can have a profound impact on a persons’ quality of life (QoL), affecting physical, emotional, psychological and social aspects. A recent systematic review reported that health-related QoL (HRQoL) in people with psoriasis is significantly compromised, especially in young adults and in women (2). Other studies have documented the impact of psoriasis on profession (career choices and decisions), family (relationship, time, intimacy etc.), sexual life, and education (3, 4). Studies on eczema have highlighted that disease control “goes beyond the skin” affecting psychological and social aspects, and impacting on everyday activities (5). A high burden of psychiatric disorders, including depression, anxiety and suicidal ideation (6, 7), have been reported in studies of patients with eczema and acne suggesting that the optimal management of chronic skin conditions requires a holistic approach, encompassing management of the skin lesions alongside the psychological sequelae and impact on HRQoL.
HRQoL is a key outcome in health research including clinical trials. The multidimensional construct captures information on patient’s physical and mental health status and the impact of health status on quality of life (8). It is important to examine the construct of HRQoL as it focuses on the well-being of a person, which is mostly affected by the healthcare provided, changes in health status, and the available social support (9).
Dermatology specific HRQoL questionnaires are commonly used when assessing disease burden and evaluating new treatments. The 2017 NICE guideline on psoriasis recommends that the severity of the disease is assessed regularly using HRQoL questionnaires (10). The British Association of Dermatologists (BAD) outlines the approaches necessary for achieving ‘high-quality care’ (11), stressing the value of ‘patient experience’ in addition to safe and effective care. The European Academy of Dermatology and Venereology (EADV) also highlights the importance of QoL measurement in dermatology clinical practice, emphasizing various bene?ts of routine use of HRQoL measures in routine practice (12). Two frequently used measures are the Dermatological Life Quality Index (DLQI) (13) and the Skindex-29 (14), with others, such as the Dermatology Quality of Life Scales (15), the Dermatology-specific Quality of Life instrument (16), used less often. The use of qualitative methods in the development of both the DLQI and the Skindex was limited. In the development of the DLQI, 120 patients from an outpatient dermatology department were asked to write down all the different ways their skin disease affected them, from which 49 different aspects were identified and ranked according to frequency (17). The development of the Skindex was based on published literature and ‘directed focus sessions’ with patients, physicians and nurses without further details being reported (18). Further, it it is unclear which instrument best captures the recent/current impact of skin disease on the individual when compared to each other.
Therefore the purpose of this study was to explore patients’ views of format and content of the DLQI and Skindex-29 using a qualitative research approach.
Study design and sampling strategy
This was a qualitative study using face to face, semi-structured, in-depth interviews in adults (>18) with a physician diagnosis of eczema or psoriasis. We excluded those not fluent in English, or unable to give informed consent or with concomitant chronic disease (with the exception of asthma, so as not to exclude those with eczema).
Recruitment
Convenience sampling was undertaken by distributing leaflets about the study in the outpatient departments of our local hospitals and public spaces (such as libraries and coffee shops) in Brighton and Hove. A telephone number was written on the leaflets and advertisements so that patients could directly contact the research team to discuss eligibility and other questions before arranging a time and place for the interview. Once the potential participants were identified, eligibility criteria were checked and selection of participants was done either by direct approach from the researcher or by nurses and dermatologists.
Data collection and analysis
Participants began by completing the two questionnaires:
– DLQI, a 10-item validated questionnaire available in > 90 languages, which since its introduction in 1994 has been used in > 40 different skin conditions (13, 17). DLQI assesses the impact of the patient’s skin on symptoms, feelings, daily activities, leisure, work or study, close relationships and treatment during the previous week. Items are presented as questions with response options of ‘not at all’, ‘a little’, ‘a lot’ and ‘very much’. Eight questions also have a ‘not relevant’ response option.
– Skindex-29 is also a validated instrument (14). It has 3 scales addressing emotions (10 items), symptoms (7 items) and functioning (12 items). Each item is presented as a statement, with the response options of ‘never’, ‘rarely’, ‘sometimes’, ‘often’, and ‘all the time’. Questions relate to the preceding 4-week period.
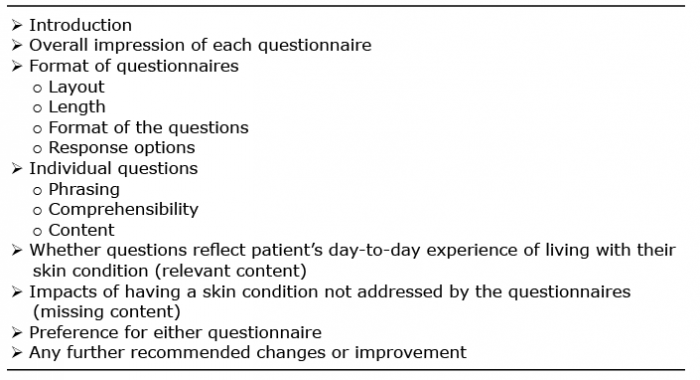
The face to face semi-structured interview which followed completion of the questionnaires encouraged participants through open questions, to critically evaluate the structure and content of these two questionnaires. The interviewers encouraged participants to talk freely about aspects of their skin disease that were bothersome to them, including how their skin affected their QoL, and whether the questionnaire items captured this. As an aide, a topic guide (Table I) was referred to during interviews to ensure that the interview did not deviate too much between researchers. The topic guide was formulated based on a similar study in patients with asthma (19) and modified through a mock interview and discussions within the research team.
The two interviewers (PP and SS) had no involvement in the clinical care of participants. The interviewers were trained to maintain neutrality and use open questions, encouraging new ideas and thoughts to emerge. Interviews were recorded using a digital voice recorder and were transcribed manually. Data were analysed in a step-by-step process using thematic content analysis as suggested by Burnard (20). The process involves a step-by-step process of open coding and categorisation – a structured method which is useful in organizing complex textual data in a systematic and transparent manner.
Two researchers analysed the first 14 transcripts separately before meeting to discuss and finalise the codes to be used. The coding process was iterative; the identified themes from the two researchers were discussed with the wider research team and an agreement was reached for the main themes.
Ethics and clinical governance approval were obtained from the NRES Committee South West Exeter and Research & Development Office, Royal Sussex County Hospital (11/SW/0333).
Table I. Topic guide used for interview process
Twenty-eight participants (17 male) with a mean age of 48 years (range 18–77) took part in the study. Eleven participants had eczema (mean duration 30 years) and 17 had psoriasis (mean duration 18 years). Two patients were identified through local libraries, the remainder were attendees at Dermatology out-patient clinics. Interviews lasted between 15-40 min.
Questionnaire structure
Participants were generally satisfied with the length and the overall layout of both questionnaires and found them easy to complete: “It [Skindex -29] was very simply laid out; very easy to understand. And you could zip through it quite quickly.” (P2).
“... very structured [DLQI] – and the way it is numbered … easy to go through I think.” (P7).
In terms of the format, the statements in the Skindex-29 were considered to be “quicker to read and get the answer in your head” (P7) as they were structured in first person. In contrast, the question format of DLQI was perceived as “someone else is asking the questions” even though participants were self-completing the questionnaire (P24), making it harder to think and contemplate the answers. One patient wanted more space between the questions and suggested using arrows instead of dots for clarity (Skindex-29). Others commented that the ‘not relevant’ option in the DLQI appears detached and needs to be better integrated with the text.
Questionnaire content
The majority of participants affirmed that both questionnaires broadly captured their QoL: “I think there’s a good range of questions, some of which in 50 odd years I have not been asked. So, I’m pleased to see those kinds of things there. Just about the effect that it has not only on work, but on your social life, interpersonal life and on your intimate life.” (P19).
When comparing the two questionnaires, most participants favoured the Skindex-29. They described it as “comprehensive” and “relate personally” (P8), covering a wide spectrum of issues ranging from social, psychological, physical and sexual. In contrast, the DLQI was described as more “generic” (P25), failing to address the emotional impacts of skin disease. Some participants commented that the two questionnaires were complementary; Skindex-29 better capturing emotions whereas the DLQI captured impact the disease on activities: “…Skindex-29 is more about how do you ‘feel’ about it… You’re depressed, you’re angry, seems to be a more emotional approach to the problem. And [DLQI] is actually saying on a day-to-day basis, over the last week, has it interfered with your shopping or looking after your home or garden. So DLQI seems to be ‘action’, and Skindex-29 seems to be ‘emotion’” (P18).
Recall period
The Skindex-29’s 4-week recall period was preferred to the one-week of the DLQI; many participants commented that a month would include at least one outbreak or flare-up, when their skin condition impacted maximally.
“... I mean psoriasis, as I understand it, is a cyclical condition. So it goes up and down, and up and down. If you asked me that questionnaire – the one-week questionnaire [DLQI]– about last week, you might catch me at a point where it has gone right down and the lesions aren’t particularly painful or itchy, whereas the four week one [Skindex-29] would catch, probably, most of the cycle.” (P13)
Some participants recommended that the questionnaire focus should be about exacerbations or times of maximal impact. One respondent was concerned Skindex-29’s 4-week recall period might capture coping strategy rather than the actual impact of the symptoms.
“I think that that questionnaire [Skindex-29] captures a state of mind over four weeks as opposed to this [DLQI] that captures maybe the physical negativities of psoriasis over the last week. I felt that was more sort of mental – how are you coping with the psoriasis as opposed to what the actual physical discomfort” (P9).
Another participant favoured one week recall period of DLQI stating that it might capture the true reflection of the condition “a really accurate snapshot of the last seven days, I think that you can answer this with less thinking and possibly with slightly more accuracy” (P9).
Ambiguous and repetitive phrases
The lack of clarity regarding the various phrases used in the Skindex-29 questionnaire was a recurrent theme. Patients mentioned that phrases used were ‘difficult’ and ambiguous. Questions had “a kind of similar sort of angle” creating a sense of repetitiveness of items.
“I find Question 3 [in Skindex-29] quite difficult, “I worry that my skin condition may be serious” -Well, if that’s im-plying that I think it might be ‘cancer’, then no. But does it cause me serious ‘problems’ over my life? Then yes... so I don’t quite know how to answer that question. So, it might need to be a bit more specific, for me, it would be. Because what do you mean by ‘serious’? Seriously inhibiting my life OR maybe serious as in a disease?” (P18).
It was suggested that phrases with similar meaning could be grouped together to allow participants to select the more relevant one, “I would sort of group those [indicating ashamed, embarrassed, and frustrated] so that people can make a comparison and give you a more accurate answer”. (P9). The issue of repetition of similar phrases was further highlighted by another patient: “I thought that I had started the same one again, because I thought somewhere in here it says ‘Am I ashamed?’ ‘Am I embarrassed?’ I think there is a similarity in that question to be honest. I think you could have one question which said ‘are you ashamed or embarrassed’ (or ashamed/embarrassed)” (P18).
But other participants welcomed this granulation as it enabled them to capture the variety in their emotions: “Very thorough, in terms of, you’ve alternated the words (Skindex-29), one minute --- I am irritated, the next minute - my skin makes me angry, my skin is sensitive…So you can take on board the different kind of embarrassments, humiliation…. I do feel sometimes, that humiliation and embarrassment are different” (P18).
Missing items
Participants identified areas missing from each of the questionnaires. Area of perceived neglect in Skindex-29 related to items regarding treatment and referral process, and how the treatment adherence interferes with daily routine were missing from the Skindex-29 questionnaire: “The only thing that isn’t captured there …is understanding and dealing with the process of treatment.” (P13). “Just about how the treatment interferes with your routine, and how it affects your skin as well” (P24).
Whilst both questionnaires have a question relating to work, participants felt that the impact of their skin conditions on employment options is not clearly captured by either questionnaire. Some explained how their skin condition limited their careers: “The quality of jobs I did was actually lower than my qualifications. I have worked part-time instead of full-time due to the eczema interfering on a daily basis” (P18). Others discussed the disease impact on professional relationships: “I work for lots of people from different companies and I do notice some people seem – ‘Ooh, I don’t really want to shake that hand’. Or they will shake my hand with a flat hand” (P9).
Participants commented that their perceptions and experiences were fluid, and responses were influenced by past experience, the duration of their skin condition and season of the year: “Because how you approach it and how you experienced it before, makes you answer this question differently… For instance, I could say my skin isn’t very irritating, but I could say actually I have forgotten that it was irritating last night. But because it wasn’t as irritating as it was 10 years ago, how do I actually answer that?” (P18).
Some said they had lived with a skin problem for so long that they had no choice but to cope. This transition from feelings of helplessness to reluctant acceptance was not covered in the questionnaires: “... I think you would find that more older people would go ... ‘it is boring and it is tedious but I can live with it’…And more younger people would go ‘it is hell and I want to commit suicide’.” (P4).
In recognition of these absolute and relative shifts in their quality of life there were requests for questionnaires be administered regularly in routine clinical practice:
“...it strikes me that, in terms of an initial assessment, or even an assessment for someone returning to the clinic…you know it’s quite possible that (pause) you don’t just run the survey once, you know, you might run it every little while…” (P19).
Sensitive and irrelevant question items
Participants reported not all items asked in DLQI and Skindex-29 were relevant to them, often cited were sexual relationships and certain activities (e.g. gardening, sports): “Does it affect you when you are gardening?’(DLQI) and things like that. I don’t know how many people are doing gardening around here.” (P1).
When their disease excluded them from these activities they were not always certain how to respond, as ticking the ‘never’ response in Skindex-29 erroneously implied that their disease was without impact. Although ‘Not Relevant’ response option is stated in the DLQI, this option was not available in the Skindex-29: “‘My skin condition interferes with my sex life’ – well, that’s irrelevant. I think there should be a ‘not-relevant’ box [in Skindex-29].” (P20).
Participants were generally satisfied with the length and layout of the two frequently used dermatology-specific QoL questionnaires (DLQI and Skindex-29), but found some items were ambiguous, repetitive or irrelevant. The majority preferred the Skindex-29 as it was perceived to be easier to understand, used a longer recall period and better captured a variety of emotions and experiences. The DLQI, on the other hand, was perceived to overlook the emotional aspect experienced by people with skin disease. The topics not adequately covered by either questionnaire were coping strategies, treatment and side effects, previous experience with the disease, impact due to seasonal variation and limitation in job choices.
Participants in our study were more critical of the DLQI than the Skindex-29. DLQI’s failure to address emotional impact was also highlighted in a previous systematic review (21). The review concluded that the DLQI fails to adequately capture the emotional and mental aspects of the patient’s QoL. Indeed, the DLQI does not capture relevant items such as sleep and swimming but includes questions regarding relationships with friends and relatives which might have little relevance to patients with mild to moderate atopic dermatitis (22). Also, the ‘not relevant’ response option in DLQI has been suggested to raise a concern in content validity of the measure. A study using data from two surveys in patients with psoriasis found that close to 40% of patients provided at least one ‘not relevant’ response, particularly women, elderly patients and those with low educational background (23).
The quest for authenticity regarding instrument development has been highlighted recently, emphasizing the importance of robust development and content validation of dermatology specific patient reported outcomes (PROs) (24). Patient involvement is generally encouraged when developed PRO tools, but in reality, patients are not always involved and when they are their level of involvement varies considerably (25). The design and development of QoL measurements is time consuming and complex; striving to achieve a balance between robust psychometrics and patient preferences may not always be achievable. Additionally, patient suggestions may not always relate to QoL. For example, participants in this study often wished to know exactly what triggered or exacerbated their skin condition and were disappointed by the lack of information provided by their healthcare provider. Also, patients mentioned that items regarding treatment and its side-effects were missing from the questionnaire. Although this uncertainty about the pathogenesis of skin conditions and the lack of information highlights a need for further research, understanding of these matters falls outside the remit of a QoL of questionnaire. Similarly, including questions that relate to seasonal variation, an external factor, may also be considered outside the realm of QoL. Similarly, for limitation of job choice, one could argue that while this is important when considering life as a whole, it does not fit within a questionnaire with a recall period of several weeks or a month. This suggests that the content validity of the questionnaire should have a balance between the lay and the professional perspective (26).
The findings of our study corroborate with the previous research that has looked at QoL questionnaires in a similar fashion. A study exploring patients’ views of three commonly used asthma specific QoL questionnaires reported that patients’ perception varied across the questionnaires; one questionnaire was perceived to focus on ‘emotions’ one ‘medical’ and the other ‘non-medical’ (27). Another study, eliciting patients’ opinion on content and format of three asthma-specific questionnaires, also reported similar findings (28). A recent study describing the process on new questionnaire construction in severe asthma has highlighted the need when developing questionnaires that are fit for purpose to engage patients as partners from the beginning, not merely as sources of information (29).
The missing content highlighted by the participants in our study have also been emphasized in previous qualitative studies among patients with skin disease. A recently published study of patients with psoriasis reported that patients find it difficult to adhere to treatment as they interfere with the physical and psychological demands of everyday living (30). Seasonal variations in disease symptoms, and adjustment and coping mechanisms adapted by patients have also been discussed previously (3, 5, 30). The issues regarding the impact of skin disease on career prospects have been documented, with patients reporting limited employment options due to their physical appearance or time consuming treatment schedule (4, 30).
Our study is the first exploration of the patients’ perspectives in relation to existing skin-specific QoL questionnaires but it has some limitations (participants were all Caucasian with either eczema or psoriasis). Further studies are needed that include other ethnic groups and other dermatological conditions. We recognise that excluding participants with concomitant chronic diseases might have resulted in less reflective real life experience. However, as our aim was to specifically understand whether dermatology specific QoL questionnaires capture the lived experience of people living with a skin condition, involving patients with other chronic conditions may have resulted in a less clear understanding of the impact of the respective skin disease on everyday life. Using convenience sampling rather than purposive sampling may be considered another limitation of our study, but necessary because of time and money constraints. Information on the perceived severity of participants’ skin condition would have been of value to further characterise the sample and to demonstrate diversity and should be included in further studies.
In conclusion, from the patients’ perspective, the Skindex-29 seems to be preferable for assessing QoL in inflammatory skin disease due to its ability to capture a variety of emotions and experiences and use of a longer recall period. However, views were diverse and some participants commented how the Skindex-29 and the DLQI complemented each other. Further research is needed to elicit participants’ views in a more diverse sample, varied settings and considering further available questionnaires.
Conflict of interest: CA is a member of the executive committee of the Harmonising Outcomes Measures for Eczema (HOME) initiative and lead of the QoL working group within HOME. He has received honorariums and institutional funding from Dr Wolff GmbH, and honorariums from Sanofi Genzyme.


 Click to show fullsize
Click to show fullsize