


1Dermatology Department, Hospital Clinic of Barcelona, University of Barcelona, 2Institut d’Investigacions Biomediques August Pi I Sunyer (IDIBAPS), and 3Biomedical Research Networking Center on Rare Diseases (CIBERER), ISCIII, Barcelona, Spain
#Both authors contributed equally to this work.
Numerous dermoscopic structures for the early detection of melanoma have been described. The aim of this study was to illustrate the characteristics of dermoscopic structures that are similar to blotches, but smaller (termed microblotches), and to evaluate their association with other well-known dermoscopic structures. A cross-sectional study design, including 165 dermoscopic images of melanoma was used to define microblotches, and 241 consecutive images of naevi from the HAM10000 database, were studied to evaluate the prevalence of this criterion in both groups. Microblotches were defined as sharply demarcated structures ≤1 mm, with geographical borders visible only with dermoscopy. Microblotches were present in 38.7% of the melanomas and 6.7% of the naevi. Moreover, microblotches were associated with an odds ratio (OR) of malignancy of 5.79, and were more frequent in invasive melanoma than in the in-situ subtype (OR 2.92). Histologically, they correspond to hyperpigmented parakeratosis or epidermal consumption. In conclusion, microblotches are related to melanomas. This finding could help dermatologists to differentiate between naevi and melanomas.
Key words: dermoscopy; dermatoscopy; melanoma; microblotches; prognosis.
Accepted Feb 19, 2020; Epub ahead of print Feb 28, 2020
Acta Derm Venereol 2020; 100: adv00106.
Corr: Susana Puig, Melanoma Unit, Dermatology Department, Hospital Clinic Barcelona, Villarroel 170, ES-08036, Barcelona. Spain. E-mail: susipuig@gmail.com, spuig@clinic.cat
This study evaluated 165 consecutive well-documented dermoscopic images, with the aim of illustrating the characteristics of a dermoscopic structure similar to blotches, but smaller (termed microblotches), and to evaluate their association with other dermoscopic structures. After evaluation by expert dermatoscopists, microblotches were defined as superficial millimetric structures with geographical borders, only visible under dermoscopy. The study also evaluated 241 consecutive naevi from the HAM10000 database and found that microblotches were present in only 6.7% of naevi cases, compared with 38.7% of cases of melanoma in our cohort (odds ratio; OR 5.79). Moreover, microblotches were more frequently observed in invasive melanoma (OR 2.92), and their presence was associated with other dermoscopic criteria of poor prognosis. Histologically, they are correlated with hyperpigmented parakeratosis or consumption of the epidermis. In conclusion, microblotches are correlated with invasive pigmented melanomas.
Dermoscopy is an essential technique in the daily practice of dermatologists, which enables the identification of multiple patterns and structures of melanocytic lesions in order to differentiate early melanomas from benign melanocytic lesions (1). Since the introduction of dermoscopy, it has been possible to reduce the number of unnecessary excisions and biopsies (2, 3).
In addition, dermoscopy has enabled the detection of certain features of invasive melanoma that correlate with a worse outcome of the disease (4–6). For example, the presence of blotches, absence of an atypical pigmented network, and the presence of microulceration has been associated with a positive sentinel lymph node biopsy (4). Furthermore, dermoscopy could help physicians to differentiate naevus-associated from de novo melanomas (7, 8).
The primary objectives of this study were to describe the dermoscopic characteristics of microblotches and to evaluate their association with patients’ clinical characteristics, with other dermoscopic criteria, and with histological features of the tumour.
A single-centre cross-sectional study on patients diagnosed with melanoma from January 2014 to June 2015 in the Melanoma Unit of Hospital Clinic, Barcelona. As inclusion criteria, only lesions with histopathological diagnosis of in situ melanoma or invasive melanoma were examined. Dermoscopy images were obtained with a Dermlite Foto (3GEN, LLC, Dana Point, CA, USA), and clinical images using a Canon PowerShot G7 camera (Canon Inc., Japan). In all the tumours, patients’ clinical variables, such as age, sex, phototype, and location of the tumour, were recorded.
Assessment of lesions and definition of microblotches
A total of 165 well-documented dermoscopic images of melanoma cases were evaluated by 2 expert dermatoscopists (SPu, JM) and 2 dermatologists in training (SPo, NF). Evaluators were asked to indicate whether the new criterion of microblotches was present or absent, and whether 3 or more observers agreed that the presence of microblotches was recognized. Furthermore, the prevalence of this criterion was evaluated in 241 consecutive cases of naevus extracted from the HAM10000 database (9), in order to determine whether microblotches were present in normal naevi.
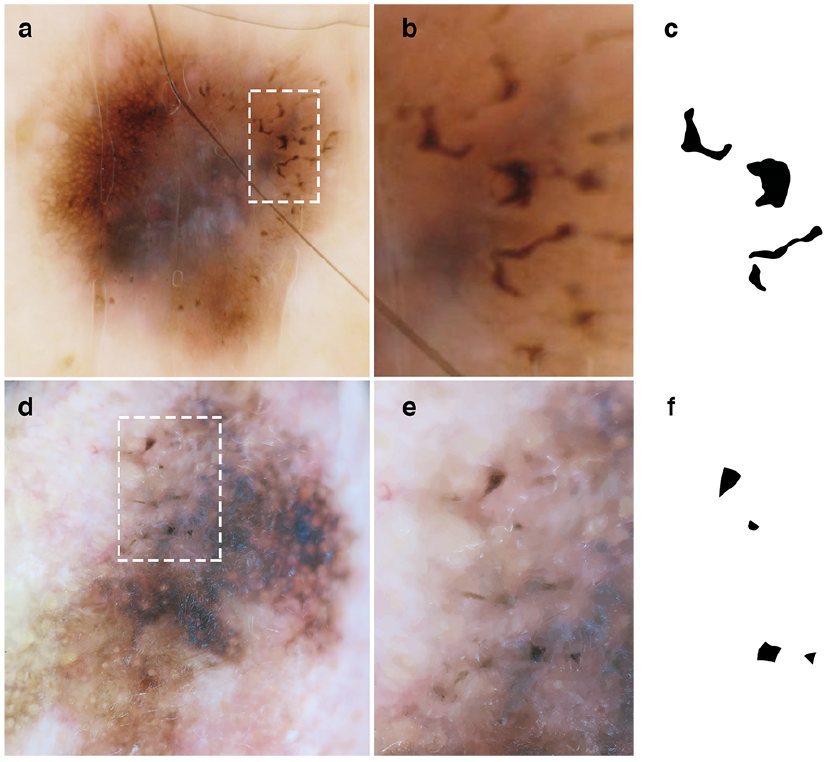
After evaluation of all images, microblotches were described as millimetric (usually less than 1 mm), well-defined structures with geographical borders, without visible dermoscopic structures in their interior. They may be different colours (black, light-brown, dark-brown, or display reddish tones), only visible with dermoscopy, and are seen more clearly with the application of immersion fluid. It was observed that microblotches are usually located in areas of higher pigmentation, and can be located both in the centre and the periphery of the tumour (Figs 1 and 2). Histopathological analysis revealed that they are correlated with 2 different conditions: epidermal thinning by the consumption of superficial layers of the epidermis; and/or presence of focal pigmented parakeratosis (Fig. 2). Interestingly, microblotches were not seen in amelanotic melanomas; however, there were only 9 (3.6%) of this subtype of melanoma in this series.
During evaluation of the images, similarities to other dermoscopic structures, such as clods (globules/dots) and follicular plugs, were observed; however, microblotches differ from these structures because of their smaller size, geographical morphology and well-demarcated borders (Fig. 3).
Fig. 1. (a, b, d, e) Dermoscopic examples and (c, f) diagrams of microblotches. Note the well-defined geographical aspect of their morphology and borders.
Fig. 2. Microblotches. Examples of (a, b) microblotches and histopathological correlation with areas of: (c) consumption of superficial layers of the epidermis or (d) hyperpigmented/haemorrhagic parakeratosis (c, d: magnification ×200).
Fig. 3. Possible errors in interpretation of microblotches. (a) Globules and (b) follicular plugs are round or oval with diffused regular edges; (c) blotches are larger than microblotches, usually with ill-defined borders.
Statistical analysis
Pearson’s χ2 test was used to evaluate the association between categorical variables. If the expected frequency was < 5, Fisher’s exact test was used (Table I). The 95% confidence intervals (CIs) were obtained by the exact binomial method, and the overall risk (OR) calculated with a 95% CI. Statistical analyses were performed using the computing environment R and RStudio (10, 11). p-values < 0.05 were considered significant.
Table I. Baseline characteristics of melanoma cases (n = 165)
Interobserver analysis
A tutorial was prepared with the definition and examples of dermoscopic images of microblotches, in which 26 images were included (15 positives for these structures). In order to calculate the inter-rater reliability, a validity set of 30 images was assembled and given to the 3 independent observers (AB, CC, MC). Fleiss’s kappa method was used to evaluate the kappa index, since there were more than 2 independent observers. Interobserver analysis showed a kappa value of 0.794, which indicates substantial agree-ment between observers.
Of the 165 patients, 81 were male (49.1%) and 84 female (50.9%), with a mean age of 66 years, interquartile range 54–80. Baseline characteristics of the patients with melanoma included in the study are summarized in Table I. Microblotches were present in 46 melanomas, and were more frequent in invasive melanoma (39%, n = 31/80) than in in situ melanoma (18%, n = 15/85). The presence of microblotches was correlated with a 2.92-fold (95% CI 1.44–6.14; p = 0.003) increased risk of invasive melanoma compared with in situ melanomas.
Furthermore, 241 consecutive cases from the HAM10000 database were analysed, and a prevalence of 6.7% of microblotches was found, which were mainly present in more atypical dermoscopic lesions. Moreover, the presence of microblotches was associated with an odds ratio (OR) of 5.79 (95% CI 3.11–10.82) of having a melanoma compared with the naevus database.
As for dermoscopic global patterns of melanomas that presented microblotches, the most frequent were the multicomponent pattern in 38 cases (82.6%) and the reticular pattern in 30 (65.2%). Furthermore, microblotches were significantly associated with the presence of other dermoscopic features: in 43.5% of the cases with shiny white streaks (OR 3.45), 54.3% with blue-white veil (OR 7.67), 60.9% with regression (OR 2.73), 63% with atypical network (OR 3.12), 76.1% with atypical dots/globules (OR 5.53) and 23.9% of the cases with pseudopods (OR 3.89) (Table II).
Table II. Association of microblotches with dermoscopic and histological features in melanoma cases
These results indicate that the presence of microblotches is highly indicative of malignancy, and is more common in invasive melanoma than in in situ melanoma. Furthermore, the presence of microblotches is associated with other dermoscopic criteria of poor prognosis, such as shiny white streaks, blue-white veil, regression, atypical network, atypical dots and globules, and pseudopods. Shiny white streaks, well-described structures associated with invasive melanomas and thicker tumours, appear to be due to changes in the dermal collagen (12), while microblotches provide information about epidermal changes, and both provide complementary biological prognostic information.
The literature contains several confusing dermoscopic terms (13); therefore, we suggest using the term “microblotches”, because it does not presuppose the diagnosis of the lesion (superficial basal cell carcinoma for microerosions) and does not use histopathological terminology (such as pigmented parakeratosis). The term can be used independently of the nature of the lesion. Furthermore, we believe that the presence of this structure could help dermatologists to suspect early invasive melanomas. The idea of microblotches arises from clinical observations in our centre, and with the aim of improving the morphological characterization of melanomas to better understand their biology. In daily practice, this criterion has helped us to decide to carry out further studies (e.g. confocal microscopy), resulting in the excision of the lesion and diagnosis of melanoma.
The main limitation of this study is the difficulty of performing a histopathological correlation, due to the small size of the structure, which can easily be missed in some histopathological evaluations. With increasing use of artificial intelligence (AI) for image recognition, better criteria to identify suspicious lesions will probably be developed. Nevertheless, until new algorithms are fully developed and widely available for the dermatology community, it is important to continue working on clinical dermoscopy criteria that can be used by all dermatologists.
Further studies are needed to determine whether microblotches constitute a prognostic factor or influence the survival of patients.
The authors thank the patients and their families, who are the main reason for our studies; the nurses from the Melanoma Unit of Hospital Clínic of Barcelona, Daniel Gabriel, Pablo Iglesias and Maria E. Moliner for helping to collect patient data; and Paul Hetherington for helping with the English editing and correction of the manuscript.
Part of the work was developed at the building Centro Esther Koplowitz, Barcelona.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize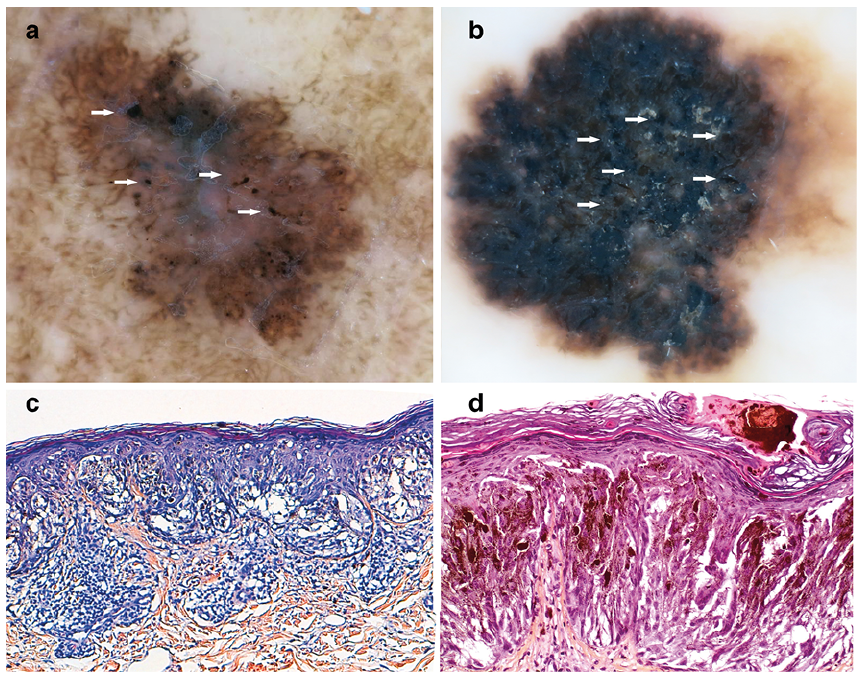 Click to show fullsize
Click to show fullsize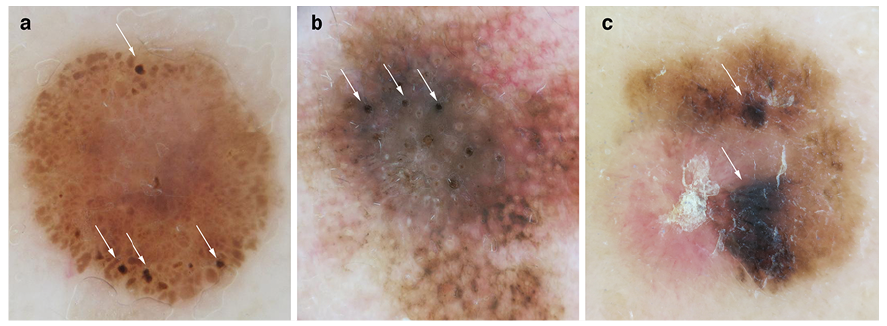 Click to show fullsize
Click to show fullsize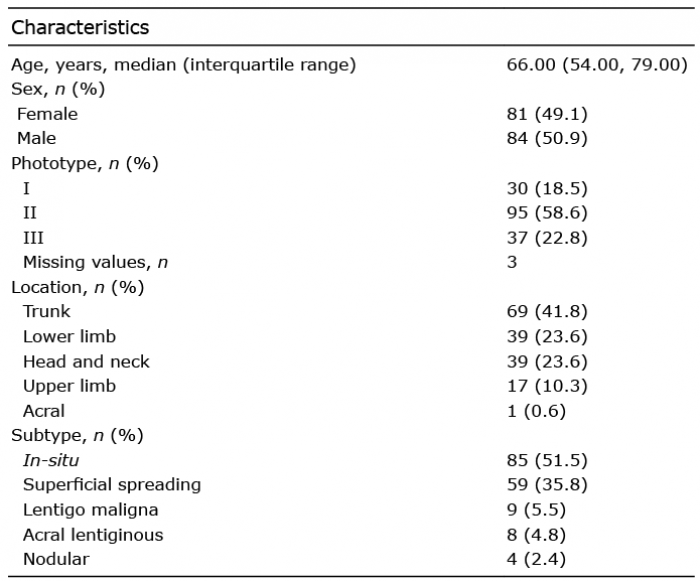 Click to show fullsize
Click to show fullsize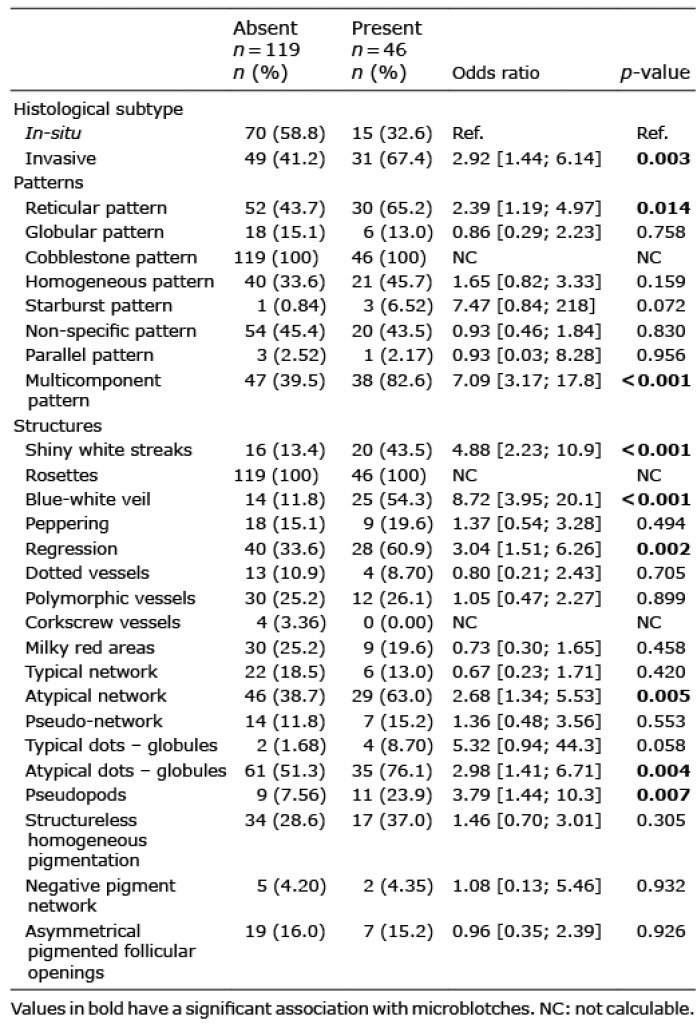 Click to show fullsize
Click to show fullsize