


1Dermatology Department, and 2Medical Oncology Department, Hospital del Mar-Parc de Salut Mar, Passeig Marítim, 25-29, ES-08003 Barcelona, Spain. E-mail: daniel.lopez.castillo@gmail.com
Accepted Feb 19, 2020; Epub ahead of print Mar 2, 2020
Acta Derm Venereol 2020; 100: adv00079
Fibroblast growth factor receptor (FGFR) inhibitors are novel targeted antineoplastic therapies that are obtaining promising results against malignancies with molecular alterations involving the FGFR pathway, such as urothelial carcinoma, cholangiocarcinoma, ovarian cancer and lung adenocarcinoma (1). Hyperphosphataemia, as a result of fibroblast growth factor 23 (FGF23) signalling blockage is a common adverse effect associated with selective FGFR inhibitors (2). Cutaneous adverse events have been rarely described in clinical trials, and include alopecia, nail alterations, dry skin, xerostomia and stomatitis (2–5). We report here a case of metastatic calcinosis cutis (CC)in a patient being treated with a pan-FGFR inhibitor that presented a fast resolution after drug withdrawal.
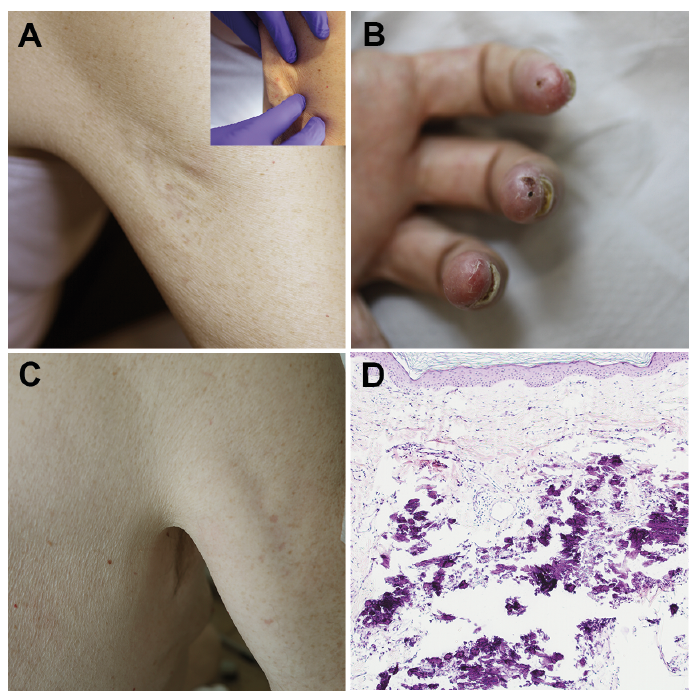
A 69-year-old man was referred to our Department for evaluation of 2 painless, firm, well-defined nodules on both axillary folds, which had developed progressively during the last few weeks. Recent medical history included localized muscle-invasive urothelial carcinoma of the bladder, initially treated with radical cystectomy. Two years later, metastatic retroperitoneal lymph node relapse was observed, and palliative treatment with first-line carboplatin/gemcitabine chemotherapy was administered. Shortly afterwards, pulmonary and hepatic metastatic progression was detected. After demonstrating tumoural FGFR3 overexpression, the patient was included in a clinical trial with an oral selective pan-FGFR inhibitor. After 3 months of treatment, the patient noticed the progressive development of 2 indurated nodules on both axillary folds, accompanied by toenail alterations and painful lesions on the fingers. Physical examination revealed 2 well-circumscribed stony-hard plaques, 4–5 cm in diameter, on the posterior aspects of both axillary folds (Fig. 1A). Furthermore, subungual haemorrhage on the toes and punctiform ulcers on the fingertips were identified (Fig. 1B). A punch biopsy of the left axillary plaque revealed an atrophic epidermis with the presence of amorphous homogenic basophilic aggregates in the entire dermis and upper subcutis corresponding to calcium salts deposits, with no involvement of sweat ducts and vessels (Fig. 1D). Two weeks after starting anti-FGFR treatment, persistent elevated phosphate levels (7.3 mg/dl; reference range: 2.5–4.8 mg/dl) were detected, and management with an oral phosphate binder was initiated and maintained during therapy. Nonetheless, follow-up laboratory studies showed persistent hyperphosphataemia (reach peak 7.7 mg/dl) and elevation of the calcium phosphate product (> 70 mg2/dl2) coincident with the appearance of cutaneous lesions, with no alteration of calcium serum levels (reference range: 8.6–10.2 mg/dl).Withdrawal of the FGFR inhibitor was decided owing to maintained hyperphosphataemia and secondary metastatic CC. Clinical and laboratory follow-up showed normalization of serum alterations 2 weeks after drug withdrawal and a complete resolution of the axillary nodules 5 weeks afterwards (Fig. 1C). Subungual haemorrhages and digital ulcers also resolved. An X-ray was performed and disclosed no remaining calcinosis. The first radiological assessment of the patient showed excellent partial response of the disease. However, the patient died 2 months after the initial dermatological assessment due to disease progression.
Fig. 1. Clinical photographs of patient. (A) Right axilla demonstrating palpable well-circumscribed firm plaque. (B) Painful digital ulcers of the left-hand finger tips. (C) Resolution of the right axilla plaque after drug withdrawal. (D) Punch biopsy from left axilla reveals an amorphous granular basophilic material in the entire dermis of homogeneous basophilic aggregates compatible with calcium salts (haematoxylin and eosin, ×100).
Several novel highly specific pan-FGFR1-4 inhibitors are currently being investigated in clinical trials and have shown encouraging anti-tumour activity in solid tumours harbouring FGFR pathway alterations. A phase 1 trial of rogaratinib, an oral selective pan-FGFR inhibitor, in several types of advanced cancer reported hyperphosphataemia as the most common adverse effect (in 77 of 126 patients; 61%) (6), with serum level restoration in all cases after phosphate binder management and no associated complications. Similarly, erdafitinib, the only pan-FGFR inhibitor currently approved for metastatic urothelial carcinoma, was associated with hyperphosphataemia in 77% of patients in a phase 2 trial and this adverse event was the second most frequent cause leading to dose reduction (3). Pharmacological renal FGFR1 blockade causes a binding impairment to ligand FGF23, disrupting renal phosphate excretion and leading to hyperphosphataemia, increased calcium phosphate product and tissue mineralization risk (7). Hyperphosphataemia and a tumoural calcinosis-like syndrome had been initially observed in FGFR blockade preclinical murine models (8). Results from clinical trials with similar FGFR inhibitors are consistent with this phosphate homeostasis disruption (2–5). Main reported cutaneous adverse effects associated to FGFR inhibitors therapy include stomatitis, dry skin, alopecia, nail alteration (including onycholysis, paronychia, onychodystrophy, onychomadesis, nail discoloration), xerostomia and hand-foot syndrome (2–5, 9).
CC is characterized by the deposition of insoluble calcium salts in the skin and is manifested clinically by skin-coloured, white-yellow or erythematous firm papules, nodules or plaques (10). Metastatic CCresults from an imbalance of the calcium and/or phosphate metabolism leading to precipitation of calcium. CC secondary to FGFR inhibitor treatment-related hyperphosphataemia was the most likely cause of calcium deposition in our patient. Tissue calcification secondary to tumour lysis syndrome was less likely, due to stable electrolyte balance, correct calcium serum level and normal renal function. Characteristically, metastatic CC affects periarticular areas, as seen in our patient (10). CC secondary to FGFR inhibitors may have similar mechanisms with hyperphosphataemic familial tumoural calcinosis, also called hyperostosis hyperphosphataemia syndrome, an autosomal recessive genetic disorder caused by loss-of-function mutations in the FGF23, GALNT3 and KLOTHO pathways (11). This rare entity is characterized by recurrent cutaneous and subcutaneous calcifications, usually on the extensor surface of periarticular skin of large joints, typically the hips, elbows and shoulders.
To our knowledge, 2 cases of metastatic calcinosis cutis associated with FGFR inhibitor therapy have been reported previously. A 24-year-old man with advanced-stage Wilms tumour developed metastatic CC in both axillary vaults and posterior popliteal fossae under therapy with pemigatinib (INCB-054828), a selective FGFR1-3 inhibitor, accompanied by subungual feet haemorrhages (12). Similarly, a 60-year-old man with metastatic cholangiocarcinoma treated with infigratinib (BGJ398) was diagnosed of metastatic CC affecting bilateral axillary and inguinal folds (13). Both patients and the current case presented persistent hyperphosphataemia while under therapy,
despite treatment with phosphate binder. In contrast to our patient, no detailed data regarding the evolution of the lesions was provided (Table I). To our knowledge, the occurrence of digital ulcers has not been described previously in patients treated with FGFR inhibitors.
This case increases the evidence of cutaneous CC as an adverse effect of selective FGFR inhibitor therapy. An increased aware-ness among oncologists and dermatologists regarding this side-effect is important in order to establish an early diagnosis and adequate therapeutic management.
The authors have no conflicts of interest to declare.
Table I. Characteristics of calcinosis cutis cases related to fibroblast growth factor receptor (FGFR) inhibitors


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize