


Departments of 1Dermatology, and 2Plastic Surgery, Nara Medical University Hospital, 840 Shijo, Kashihara, Nara 634-8522, Japan. *E-mail: fumim@naramed-u.ac.jp
Accepted Feb 19, 2020; Epub ahead of print Mar 2, 2020
Acta Derm Venereol 2020; 100: adv00080
Lipomatosis is characterized by diffusely distributed growing lesions composed of mature adipose tissue. The lesions infiltrate through pre-existing structures, such as blood vessels, nerves, and muscles, and often exhibit typical distribution patterns (1, 2). In contrast to circumscribed lipomas, lipomatosis is distributed in a diffuse and symmetrical manner, and the lesions are not surrounded by fibrous capsules (2). Here, we report a rare case of multiple lipomas, which had distinct clinical manifestations, such as an asymmetrical distribution and a late onset. Our case does not fit into any previously categorized disease entity, and thus, together with a case reported by Yang et al. (3), might represent a new disease entity, named adult-onset asymmetrical lipomatosis. The possibility that this case involved a mosaic condition or a variant of benign symmetric lipomatosis also needs to be considered.
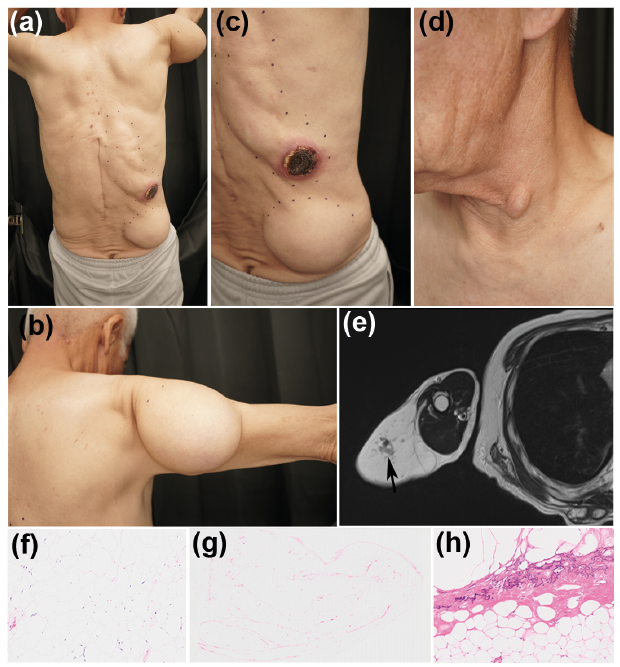
A 72-year-old Japanese man presented with multiple soft subcutaneous tumours, mainly on the right side of his trunk. He had noted a subcutaneous tumour, which measured about 3 cm in diameter, on the right side of his upper back 8 years ago, and diffusely distributed masses subsequently grew on the right side of his trunk. The tumour on the lateral side of his right lower back became necrotic so he visited a hospital, where a mass was removed from the centre of his back. Then, he was referred to our department. His medical history included hypertension and diabetes mellitus, which were diagnosed at the age of 65. He had smoked 20 cigarettes a day and drank a glass of clear liquor almost every day for over 50 years. He had no relevant family history. A physical examination demonstrated that there were diffusely distributed, soft, non-tender subcutaneous masses, which protruded between his ribs, on the right side of his back (Fig. 1a). He also had a soft rounded subcutaneous mass (size: 16 × 11 × 8 cm) on his right upper arm, which he had first noticed 3 or 4 years ago (Fig. 1b), and a similar one, measuring approximately 15 × 10 × 5 cm, on his right hip (Fig. 1c). On the right side of his back, a region of painful necrotic tissue, measuring 4.5 × 4 cm, was noted (Figs. 1a and c). He also had small soft tumours on his right jaw and the left side of his neck (Fig. 1d). He did not exhibit peripheral neuropathy. Laboratory tests revealed no significant abnormalities, except for mildly elevated triglyceride (155 mg/dl; normal range: 40–149 mg/dl) and C-reactive protein (3.59 mg/dl) levels. Magnetic resonance imaging (MRI) revealed that the tumours on the patient’s back and upper arm had solid components (Fig. 1e), and the one on his right upper arm had also infiltrated into the muscle. These MRI findings led to a suspicion of liposarcoma; thus, skin biopsy examinations were performed. Histopathological examinations of the tumours on the right arm and right hip revealed that they were composed of mature fat cells (Fig. 1f). The tumours were negative for CDK4 and p16, which excluded malignancy. A diagnosis of lipoma was made, and most of the tumours were surgically removed. The excised tumours were composed of mature fat tissue and did not have fibrous capsules (Fig. 1g). Parts of the tumours exhibited calcification (Fig. 1h), necrotic fat, and increased levels of collagen fibres. No atypical cells were observed. The necrosis on the patient’s back consisted of necrotic tissue and granuloma tissue and did not exhibit any signs of malignancy. No recurrence has been observed since the operation.
Fig. 1. (a) Multiple tumours were present, mainly on the right side of the patient’s back. (b) A large soft mass was present on the right upper arm. (c) A magnified view of (a). Multiple tumours and necrosis were seen on the right side of the patient’s back. (d) A small tumour was present on the left side of the neck. (e) T1-weighted MRI of the tumour on the right upper arm showed lipomatous tissue with solid components (arrow) inside it. (f) A biopsy specimen from the right arm revealed that the tumour was composed of mature fat cells (hematoxylin & eosin staining; × 100). (g) The excised tumour consisted of mature fat cells without a fibrous capsule (hematoxylin & eosin staining; × 4). (h) Some calcification was detected inside the tumour (hematoxylin & eosin staining; × 100).
Lipomatosis refers to a number of diseases, which are characterized by the progressive growth of unencapsulated fat masses with diffuse and symmetrical distributions (2, 4). A number of clinically different lipomatoses have been categorized. One of these is benign symmetric lipomatosis, which has been further classified into 4 subtypes (the neck type, the shoulder girdle type, the pelvic girdle type, and the abdominal type) based on the distribution pattern of proliferating adipose tissue (2) and is characterized by the gradual development of many large, coalescent, asymptomatic lipomas, mainly on the trunk and arms, in middle-aged male alcoholics. Mutations in mitochondrial genes have been implicated in some cases (5). Another type is lipomatosis dolorosa (Dercum’s disease), which causes generalized painful, circumscribed or diffusely distributed fatty deposits in middle-aged women (2). In these two diseases, multiple lipomas arise during adulthood. As our case involved asymmetrically distributed lipomas, it did not fit into either of these two entities. Asymmetrically distributed growing regions of lipomatous tissue are seen in Proteus syndrome and hemihyperplasia-multiple lipomatosis syndrome (6). However, these conditions are often congenital and are associated with vascular malformations (7). In our patient, asymmetrically distributed non-tender lipomatosis developed around the age of 65 years; therefore, our case does not fit into either of these entities. Familial multiple lipomatosis (FML) is another disease entity that needed to be considered as a potential diagnosis in the present case. However, the clinicopathological features of our case were not compatible with FML since FML is a hereditary syndrome, involving multiple symmetrically distributed encapsulated lipomas (8).
Thus, our case differs from the conditions mentioned above. Yang et al. reported a similar case to ours, in which a patient developed acquired asymmetrical lipomatosis in her 80s (3). To the best of our knowledge, our case is only the second case of adult-onset asymmetrical lipomatosis, and therefore, probably represents a new disease entity; i.e., asymmetrical lipomatosis. Enzi et al. (4) reported similar cases but they developed in childhood and involved peripheral neuropathy. Whether the adult-onset asymmetrical lipomatosis reported by Yang et al. and ourselves belongs to the same disease entity as the early-onset asymmetrical lipomatosis reported by Enzi et al. requires further investigation. Another possibility is that adult-onset asymmetrical lipomatosis is just an asymmetrical variant of benign symmetric lipomatosis. If this is the case, benign symmetric lipomatosis should be termed “benign lipomatosis” instead. The unilateral distribution of the lipomas observed in our case also implies that mosaic gene mutations might be involved in benign symmetric lipomatosis. Further cases are needed to confirm this.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize