


Departments of 1Dermatology, 3Plastic Surgery and 4Biomedical Data Sciences, Leiden University Medical Centre, 2Department of Dermatology, Roosevelt Clinic, Leiden, and 5Department of Dermatology, University Medical Centre Groningen, Groningen, The Netherlands
The treatment of choice for cutaneous squamous cell carcinoma is complete surgical excision. Incomplete excision of cutaneous squamous cell carcinoma has an increased risk of local recurrence, deep subclinical progression, and metastasis. This study aimed to investigate the proportion and risk factors of incomplete excised cutaneous squamous cell carcinoma. A systematic review of the literature was performed. Incomplete excision rates for cutaneous squamous cell carcinoma ranged from 0.4% to 35.7%. The pooled incomplete excision risk estimate was 13% (95% confidence interval 9–17%). Risk factors noted in more than one study for incomplete excision included tumor depth and size, type of operator, head and neck localization, and former incomplete excision. We found an overall incomplete excision rate of 13% for cutaneous squamous cell carcinoma. Risk factors should be taken into account in the management of cutaneous squamous cell carcinoma surgical treatment.
Key words: squamous cell carcinoma; excision margin; surgery; treatment outcome.
Accepted Feb 19, 2020; Epub ahead of print Mar 4, 2020
Acta Derm Venereol 2020; 100: adv00084.
Corr: Roel E. Genders, Department of Dermatology, Leiden University Medical Centre, Albinusdreef 2, NL-2333 ZA Leiden, The Netherlands. E-mail: r.e.genders@lumc.nl
Treatment of choice for cutaneous squamous cell carcinoma is complete surgical excision. Incomplete excision of cutaneous squamous cell carcinoma has an increased risk of local recurrence, deep subclinical progression and increased risk of metastasis. In this systematic review, incomplete excision rates for cutaneous squamous cell carcinoma ranged from 0.4% to 35.7%. An overall incomplete excision rate of 13% was calculated. Risk factors include location in the head & neck area, tumor depth and size, invasive growth, type of operator and re-excision. These factors should be taken into account in the management of cutaneous squamous cell carcinoma surgical treatment.
Cutaneous squamous cell carcinoma (cSCC) is the second most frequent skin cancer in the world and comprises about 25% of all skin cancers. cSCC has the potential to metastasize (1). The treatment of choice in most countries is surgical excision with complete histological clearance at peripheral and deep margins (2).
Incomplete excision of cSCC has an increased risk of local recurrence, deep subclinical tumor progression, and metastasis (3). Therefore, complete excision of SCC is mandatory. Recommended surgical excision margins in Europe are 5 mm for low risk tumors and 10 mm for high risk tumors and in depth at least to the hypodermis. In case of incomplete excision, re-excision is recommended (2).
Micrographic surgery with complete margin control on frozen sections (Mohs micrographic surgery) or on paraffin sections (Breuninger technique) is considered for selected cases where a broad excision margin can cause significant aesthetic or functional impairment, as in the central face (2).
High-risk factors associated with a poor cSCC outcome, include location, greater size, poor differentiation, depth of invasion, perineural involvement, a recurrent tumor, and immunocompromised status (1).
Several studies have been published investigating positive margins after excision of cSCC. Risk factors for incomplete excision are tumor characteristics, such as location, and depth of invasion (4–6). However, the role of patient characteristics such as immunosuppression is not clear, although it has been suggested that cSCC in these patients, especially organ transplant recipients, frequently exhibits aggressive behavior irrespective of the size (7). In the present study, we review the avail-able literature studying the proportion of incompletely excised cSCC and all possible risk factors, including immunosuppression.
Literature search strategy and study selection
An electronic database search of the data sources PubMed, Embase, Web of Science and COCHRANE Library was performed, identifying studies published before 14 March 2018 that reported on incompletely excised cSCC. The following search terms and comparable were used: excision, incomplete, and cutaneous squamous cell carcinoma. The detailed search strings are outlined in Appendix S1. Titles and abstracts were screened by two authors (RG and EH). Subsequently, full texts of potentially relevant articles were assessed for eligibility by the same two authors. Any discrepancy was resolved by consensus with a third author (MK).
We included only original articles that fulfilled our inclusion criteria of 1) cSCC removed by conventional surgery, 2) studies reporting on incomplete/irradical excision 3) reports containing 25 or more cSCC cases. Studies reporting on cSCC treated by Mohs surgery and lacking cohort demographics were excluded. When more than one report was published on the same population or subpopulation, we included the report with the largest number of cSCC. This systematic review and meta-analysis were guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses principles. Inclusion and exclusion criteria and methods of data analysis were specified in advance.
Data collection process and risk of bias assessment
Data extraction was performed by two reviewers independently (NM and MM). The following information was extracted from each included study: 1) study details (e.g., design, type of operator, location and center, years of data collection, aim); 2) patient cohort (e.g. number patients, presence of immunosuppressive patients); and tumor characteristics (including number of cSCC, presence of recurrent tumors, excision margin); 3) Outcome (e.g. number of incomplete excisions, risk factors for incomplete excision, outcome of incomplete excision).
A component-based approach to assess risk of bias based on the Newcastle-Ottawa Quality assessment scale was used (8). Relevant items of this scale were used and adjusted for our cohort. Important items relevant to the topic of this review were added. The following design elements were assessed: 1) The study aim reported on incomplete excision; 2) The patient selection was consecutive and unbiased; 3) The excision margin was described; 4) If more excision margins were used, the cases where this was done were specified adequately; 5) The outcome of incomplete excision was clearly described; 6) At least 2 high risk features of cSCC were reported (e.g. recurrence, differentiation grade, size, depth); 7) Statistical methods were well-described. For quality assessment, a positive point was allocated for each feature if mentioned in the article (9).
Statistical analysis
The proportion of incomplete excised cSCC was the primary outcome measure. We estimated a pooled absolute risk of incomplete excision. Summary estimates were calculated for the proportion of incomplete excised cSCC in the head and neck region and for total body cSCC studies using STATA version 14. Risk factors for incomplete excision as a secondary outcome were presented as descriptive statistics. Due to the heterogeneity of data and risk factors involved, we performed only a basic meta-analysis.
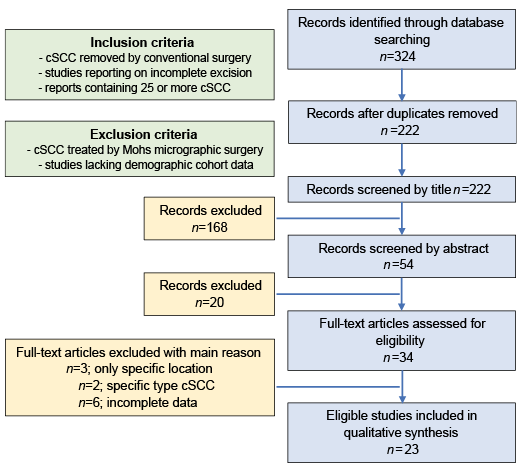
Details of the selection process for eligible studies are shown in Fig. 1. A total of 222 publications were retrieved, of which 23 studies were included in the review (Table I) (4, 6, 10–30). The studies were published between 1997 and 2018. The quality assessment score ranged from 2 to 7.
Fig. 1. Flow chart. Details of the selection process for eligible studies.
Table I. Details of studies included in the analyses and quality assessment
The number of cSCC per study ranged from 28 to 2536, with a total of 10,935 (Table II). The studies were performed in the patient populations of general practitioners (GP), dermatologists (D), plastic surgeons (PS), maxillofacial surgeons (MAX), ear-nose-throat surgeons (ENT), and general surgeons (GS), both specialists and trainees. Excision margins were documented in 12 studies and ranged from 2 to 20 mm. The majority of the cSCC in the studies were located on the head and neck. Five reports solely included cSCC in the head and neck area.
Table II. Details of studies regarding cutaneous squamous cell carcinoma (cSCC) cohort and risk factors for incomplete excision
The reported incomplete excision rate for cSCC ranged from 0.5% to 35.7%. Summary estimates for the proportion of incomplete excised cSCC was 12% (95% confidence interval [CI] 0–24%) for the H&N studies and 13% (95% CI 8–17%) for the total body studies. The pooled incomplete excision risk estimate was 13% (95% CI 9–17%) (Fig. 2).
Fig. 2. Forest plot of incomplete excision rate for cutaneous squamous cell carcinoma (cSCC).
The majority of studies (19/23) reported on possible risk factors for incomplete excision; in 15 statistical analyses were performed.
Detailed tumor location was reported in 15 studies and 9 studies analyzed location as a risk factor. Head and neck localization was found to be a significant risk factor in 3 studies (11, 17, 29). Locations on the ear (p < 0.001, odds ratio [OR] 95% CI 2.16–11.93) (6), lateral canthus, upper lip, forehead, cheek, and neck were associated with increased risk within the head and neck area (22). Location of cSCC on the foot was identified in one study as a risk factor for incomplete excision (22). In 4 studies no correlation was found with location (21, 25, 27, 28).
Brinkman et al. (13) reported a significant increase (p < 0.001) in the percentage of incomplete excision according to tumor differentiation, while other studies found no association (11, 13, 21, 22, 29).
A significant correlation with tumor size > 20 mm was found in a minority (3) of studies (10, 22, 29). No significant association was found in most (7) studies (6, 11, 20, 21, 23, 25, 28).
The thickness of the excised specimen was found in one study to be inversely related to incomplete excision (p = 0.002) (11). Another study reported increased tumor thickness as a risk factor (p < 0.001) (29).
The invasive character of cSCC was noted in two studies. One study found 4 cSCC with nerve invasion and one cSCC with ingrowth to deep fascia, two of them were incompletely excised (p = 0.0034, OR 95% CI 1.7–66.3) (6). In the other study, perineural invasion was not associated with incomplete excision (29). Re-excision was considered in 4 studies as a possible risk factor; only Tan et al. (6) found a positive association with incomplete excision (p < 0.001) (6, 17, 20, 26).
The inclusion of patients with a compromised immune status was reported in 4 studies (16, 18, 21, 29). One study excluded immunosuppressed patients from their cohort (28). In two reports, immunosuppression was not significantly associated with incomplete excision (21, 29).
Bhatti et al. (10) found excision performed by a GP to have an increased risk (p < 0.001) of incomplete excision compared to excision performed by consultants and trainees. Also, Wong et al. (30) described that medical specialists had a significantly less incomplete excision rate (p < 0.001).
The study by Delaney et al. (15) showed no difference between GPs and medical skin specialists (OR 0.84, 95% CI 0.47–1.27). Two reports found no difference between specialists and trainees in dermatology and plastic surgery (6, 21). Incomplete excision rates decreased during the course of a plastic surgeon’s surgical training (p = 0.026) (25).
The management of incompletely excised cSCC was specified in only a few studies (not shown in the table). One study reported on 119 incomplete (17.6% from total) cSCC, of which 84 underwent further excision. Residual SCC was seen in 24 (28.6%) of these specimens. Tumor diameter and Breslow thickness contributed independently to residual SCC (p < 0.001). A lengthier delay between initial excision and re-excision correlated with less residual tumor (p < 0.005) (12).
Brinkman et al. (13) reported that of 155 cSCC, 16 (10%) were excised with a minimum margin of less than 1 mm, and 36 (23%) had positive resection margins. Twenty-five were re-excised. In 27 cases, no re-excision was performed (4 radiotherapy, 3 metastases, 4 not feasible to completely remove tumor, 2 died, 3 not physically fit enough, 11 refused). In 18 re-excised specimens, no additional tumor was found, while in 4 cases some tumor remnants were identified, but completely removed. Three re-excisions were incomplete. One patient refused further treatment, 2 were re-re-excised (one totally excised, one impossible to remove and treated with radiotherapy) (13).
One study reported that of 26 incompletely excised cSCC, 15 were re-excised and 11 underwent radio-therapy (23). In the study by Rubino et al. (27) all 49 (out of 712 cSCC) incompletely excised SCC were re-excised and the entire margin was clear upon histological examination.
The development of local recurrences and/or metastasis of cSCC was reported in 3 cohorts, but the authors did not specify these results for the incompletely excised cSCC. Therefore, it cannot be concluded if incomplete excision is a risk factor for local recurrence and/or metastasis (13, 18, 27). One of these studies stated that the risk of dying of cSCC increases fourfold (95% CI 2.4–6.6) after incomplete excision (13). Incomplete excision was found to be an independent risk factor for regional metastasis (OR 2) in another study, they reported on 10 nodal metastasis in the total cohort of 218 cSCC, versus 3 nodal metastasis in the 26 incompletely excised cSCC (23).
In this review we found incomplete excision rates for cSCC ranging from 0.4% to 35.7%. Summary estimates for the proportion of incompletely excised cSCC in studies reporting on head and neck cSCC were calculated at 13% and at 12% for the total body studies. The pooled incomplete excision risk estimate was 13%. These rates are higher than Lansbury et al. (31) described in their systematic review of observational studies on interventions for non-metastatic cSCC. Overall, they found a pooled average estimate of incomplete excisions of 8.8% (95% confidence interval 5.4% to 13.0%, I2=89%). Incomplete surgical excision was reported in 11 studies (comprising 2,343 excisions with excision margins ranging from 2 to 10 mm). Seven studies reported on total body cSCC, two on head and neck cSCC, one on cSCC located at the ear and one focused on periorbital cSCC. Lansbury et al. (31) included studies reporting outcomes after surgical excision if there were 20 or more eligible participants, unless the studies were restricted to a specific anatomical location, such as periorbital or auricular sites. Similarly to our systematic review, excision margins varied between and within studies; definitions of incomplete excision within the studies were also inconsistent. Incomplete excision was defined as the presence of tumor cells at the surgical margin, the presence of residual tumor within 1 mm, or “close to” the margins of the excised specimen.
In our review, 4 studies showed noticeably high incomplete excision rates above 30%. One study was performed in an outpatient setting by GPs (14). Another study used data from an institutional pathology database, where cSCC were excised by GPs and a mixture of hospital consultants in New Zealand (10). The GPs showed the highest incomplete excision rates, but this was not specified for cSCC. The studies by Brinkman et al. (13) and Haisma et al. (16) were both performed in a tertiary referral hospital with complex cSCC cases. The other studies with incomplete excision rates between 0.4 and 17.6 % varied widely by setting (outpatient, hospital, tertiary) and tumor cohort. The setting of cSCC treatment is likely to be important. It is thought that complex cases are more likely to be treated in a tertiary hospital than in an office-based setting or at the GP office. In addition, experience naturally also plays a role, which was demonstrated in the study of Riml et al. (25).
Locations in the head and neck area, tumor depth and size, invasive growth, type of operator and re-excision were stated as risk factors for incomplete excision. This is concordant with a recently published study that found older age, location on the head and neck, increased lesion diameter, invasive subtype or increased tumor thickness, and previous treatment to be statistically significant risk factors for positive surgical margins (29).
In the head and neck, excision margin is sometimes compromised by anatomical locations. Both tumor depth and size are associated with incomplete excision (10, 11, 22, 29). Surgical margins are based upon peripheral margins, but there have been fewer evaluations concerning excision depth. To achieve adequate deep clearance, excision should be performed at the anatomical plane to the depth of the clinically apparent level of tumor invasion; therefore, the level for high risk cSCC is deeper than low risk cSCC (2, 32). This will vary according to tumor site.
In case of perineural invasion, the tumor spreads through the peripheral nerves, thereby compromising surgical margins. This risk factor was only studied in two cohorts, with one study finding a positive correlation but not the other (6, 29).
Only a few studies reported on immunosuppressed patients in their cohort. Patients on immunosuppression develop cSCC that tend to behave more aggressively, with a higher rate of both local recurrence and metastasis compared to immunocompetent patients (9, 33–35). Also, peripheral tumor borders can be difficult to properly define because of severe damage to the surrounding skin. Nevertheless, in two studies immunosuppression was studied as a risk factor, but no association was found with incomplete excision.
The development of local recurrence is a cause of incomplete excision and is associated with a high rate of further local recurrence and subsequent regional metastasis, predominantly to the regional lymph nodes (2). One study described that positive margins on re-excision showed a recurrence rate of 29% versus 5% in negative margin re-excisions. This is in line with the fact that 29% of the re-excisions for margin-positive cutaneous SCC yield residual tumor. Factors associated with residual tumor on re-excision are similar to the characteristics of high-risk SCC (5). But even with complete excision, there remains debate about what to do when histological margins are close. Conventional histological assessment of excision specimens with vertical bread-loaf sectioning examines 0.2–2% of the margins. Wider excision should be performed when margins appear more limited (debat-able < 1 mm or < 2 mm) if high risk features are present and if the benefits outweigh the risks (2).
Overall, the risk of incomplete excision can be minimized by determining adequate excision margins. How-ever, there is some discussion about the use of adequate excision margins, especially in high-risk cSCC. Recommendations for excision margins are based on only a few studies and consensus expert opinion (36). Guidelines recommend excision margins of 4–6 mm for low risk cSCC and 6–10 mm or more for high risk cSCC (32, 37, 38). There is general consensus that when reconstruction is warranted for closure of a defect, negative histologic margins have to be confirmed (38).
Excision with complete peripheral and deep-margin histologic margin control, like Mohs micrographic surgery (MMS) or techniques on paraffin block (e.g. Breuninger technique), is more often recommended for high risk cSCC, especially in anatomic sites where tissue conservation is desired (1, 32, 33, 37, 38). The MMS recurrence rate for high risk cSCC has been shown to be lower than standard surgical excision, ranging between 6 and 11% (32). However, a prospective comparative study did not show a significant benefit of MMS in terms of 5-year recurrence rates (39).
Subsequently, this systematic review on observational studies of interventions for primary, non-metastatic, invasive cSCC of the skin reports that after MMS, the pooled estimate of local recurrence during variable follow-up periods from 10 studies with 1,572 cSCC was 3.0% (2.2% to 3.9%), which was non-significantly lower than the pooled average local recurrence of 5.4% (2.5% to 9.1%) after standard surgical excision (12 studies with 1144 cSCC) (31). However, a recently published retrospective cohort study suggested that MMS is superior to standard excision for cSCC of the head and neck because of lower recurrence rates (3% versus 8%). CSCC treated with MMS were at a 3 times lower risk of recurrence than those treated with standard excision, when adjusted for tumor size and tumor invasion (HR 0.31, 95% CI 0.12–0.66) (40).
Limitations
This systematic review has some limitations. The quality of evidence limits both the interpretation and scope of this review, due to diversity in study design, patient cohorts, and data reported. The outcomes must be interpreted with caution, because of this considerable heterogeneity between studies. Several studies did not report on tumor characteristics, and risk factors could therefore not be evaluated. Excision margins were not always adequately documented.
Conclusion
We found an overall incomplete excision rate of 13% for cSCC. Risk factors include location in the head and neck area, tumor depth and size, invasive growth, and re-excision. Treatment of these high risk cSCC should be considered with surgical methods with 100% margin control.
The authors want to thank J.W. Schoones for his help with the literature search and R.M. Johnston-White for reviewing the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize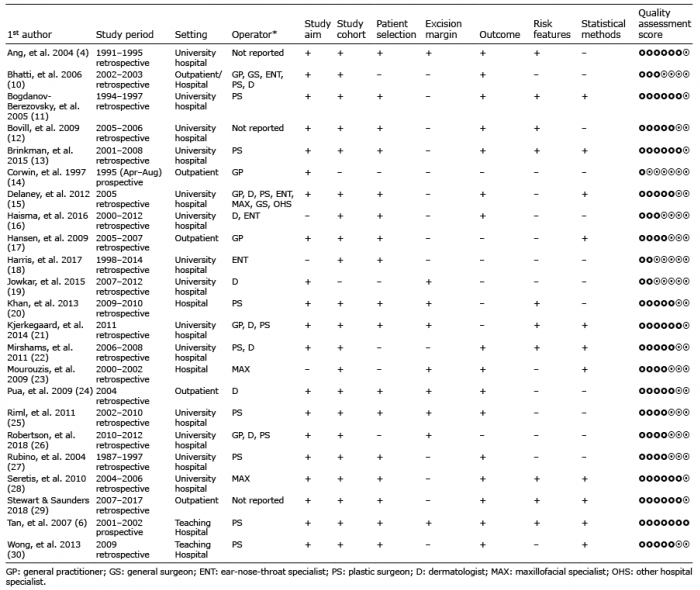 Click to show fullsize
Click to show fullsize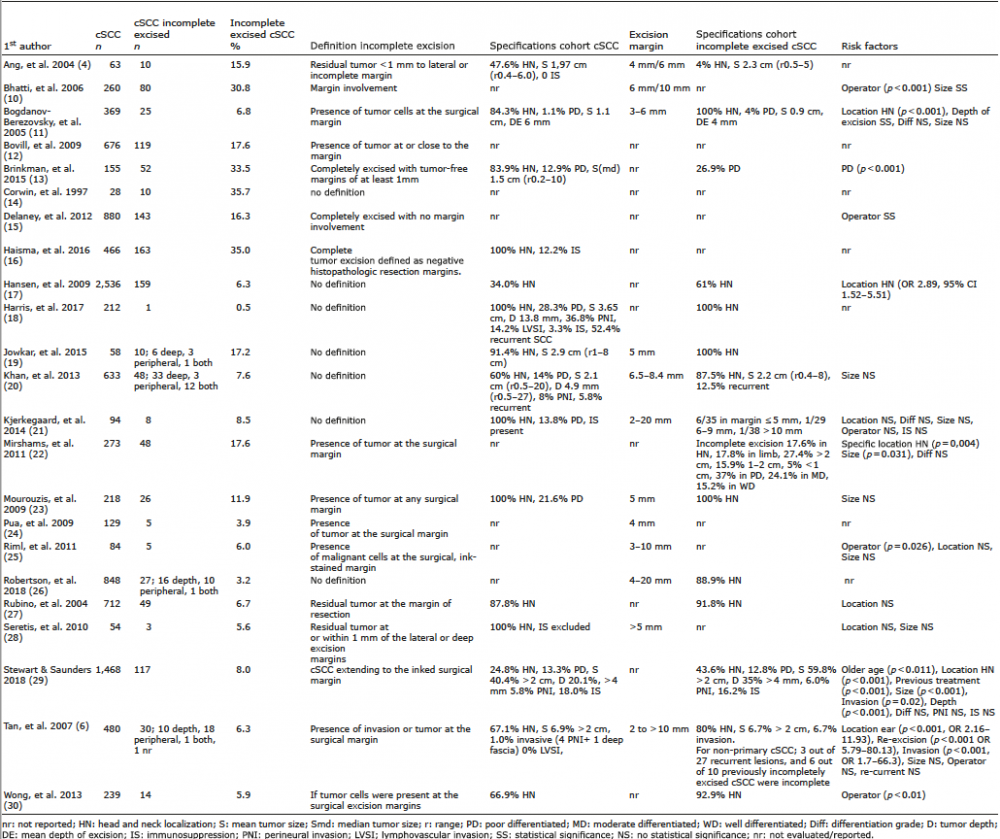 Click to show fullsize
Click to show fullsize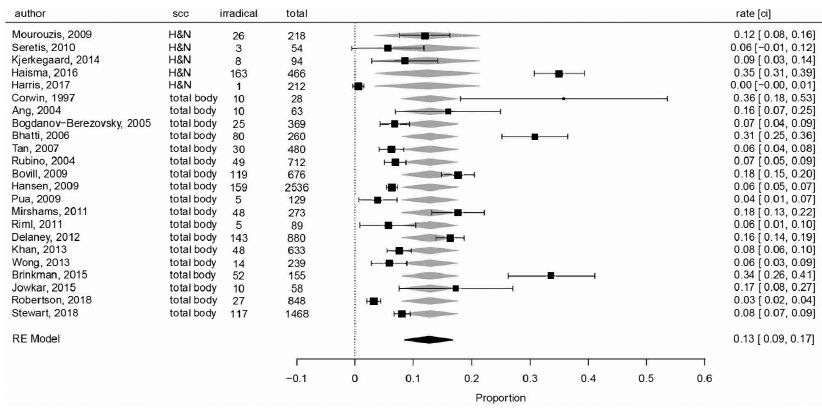 Click to show fullsize
Click to show fullsize