


Department of Dermatology, The Second Xiangya Hospital of Central South University, Changsha 410011, China. *E-mail: misseven69@csu.edu.cn; lindazgy@csu.edu.cn
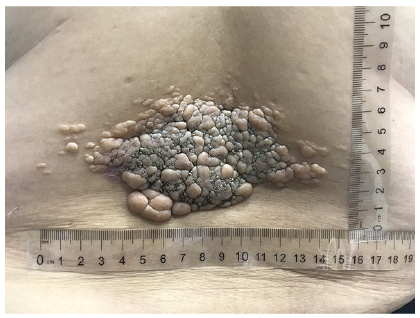
A previously healthy 44-year-old woman presented to our department with a skin lesion on her back. The lesion presented as multiple, variable-sized, skin-coloured to tan-grey, papules, focally coalesced into a huge plaque (15.5×7 cm) with a grouped distribution on her lower back (Fig. 1). The surface of the lesions presented a prominent granular appearance. The papules had appeared in early childhood, increased in number, and progressively enlarged and coalesced into a huge plaque with large amounts of grey granules on the surface. She had no family history of similar lesions, and no other physical or systemic abnormality.
What is your diagnosis? See next page for answer.
Fig. 1. Multiple variable-sized skin-coloured to tan-grey papules focally coalesced into a large plaque with prominent granular appearance on the patient’s lower back. (Rulers in cm).
Acta Derm Venereol 2020; 100: adv00085.
Diagnosis: Mucinous naevus of the combined epidermal-connective tissue naevus of proteoglycan type
A skin biopsy specimen from the plaque revealed epidermal papillomatosis with thin, elongated rete ridges and marked hyperkeratosis. Histopathological features were a prosy thickened papillary dermis of empty appearance with loosely separated collagen fibres, increased mucinous ground substance and fibroblast proliferation (Fig. 2a, b). The mucin localized in the dermis stained positive with Alcian blue at pH 2.5 (Fig. 2c, d). Based on the clinical and pathological findings, a diagnosis of mucinous naevi was made.
Fig. 2. Histopathological features. (a) Abundant mucin in the papillary and superficial dermis, epidermal papillomatosis with thin elongated rete ridges, and marked hyperkeratosis (HE staining ×40). (b) Loosely separated collagen fibres, increased mucinous ground substance, and fibroblast proliferation in thickened papillary dermis (HE staining ×200). (c, d) The mucin localized in the dermis stained positive with Alcian blue at pH 2.5 (c: ×40; d: ×200).
Mucinous naevus is a rare entity, first characterized in 1993, with naevoid features and a characteristic pattern of mucin deposits in the papillary dermis (1).The clinical feature of mucinous naevus is multiple, asymptomatic, brownish to skin-coloured papules or plaques, with a striking unilateral, linear, zosteriform, or grouped distribution. The clinic characteristics of reported cases of mucinous naevus are summed up in Table I.
The typical histopathological presentation of mucinous naevi is a diffuse, band-like deposition of mucin in the superficial dermis. Depending on whether the epidermis is normal, mucinous naevus is divided into 2 histopathological types: a CTNP type and combined epidermal-CTNP type (2). Regardless of classification, the origins of the mucin and the mechanism of its development are unclear, but previous studies suggest that mucin formation might increase as a result of fibroblast upregulation (3, 4). Using immunohistochemical staining, Li et al. (5) found that the dermal fibroblasts were positive for CD34 and vimentin, but negative for CD31, laminin and S100. Ultrastructural observation revealed exuberant mucin and hyperactive fibroblasts with abundant rough endoplasmic reticulum and secretory vacuoles in the lesion dermis. Our case also showed an increase in number of fibroblasts, which lends additional support to the hypothesis that mucin deposition may develop in association with fibroblasts.
Treatment is not necessary for a mucinous naevus, due its benign nature. Surgical operation, carbon dioxide laser and topical drug therapy, including keratolytic, corticosteroid ointments and retinoids, may remove the lesion effectively. Chi et al. (6) proposed that carbon dioxide laser vaporization may be a treatment option for mucinous naevus of the combined epidermal-CTNP type with multiple exophytic and verrucous lesions, but not for the CTNP type. However, Mulcahy et al. (7) reported a case of combined-CTNP type, in which carbon dioxide laser resurfacing resulted in hypertrophic scarring despite being performed by an experienced laser dermatologist. Thus, the outcome of such treatment is unpredictable.
Table I. Characteristics of 31 reported cases of mucinous naevus (including the present case)


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize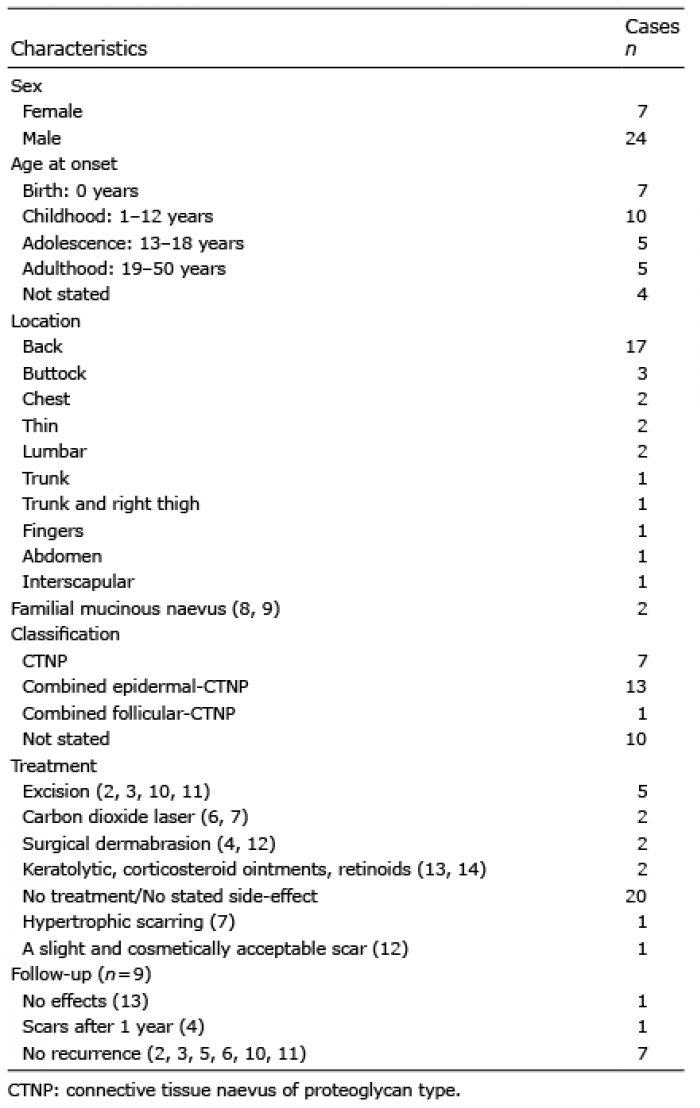 Click to show fullsize
Click to show fullsize