


1Department of Dermatology, Reference Center for Rare and Undiagnosed Skin Diseases, Larrey Hospital, 24, Chemin de Pouvourville, TSA 30030, FR-31059 Toulouse Cedex 9, and 2Dermato-pathology Department, IUCT Oncopole, Toulouse University Hospitals, Toulouse, France. *E-mail: mazereeuw-hautier.j@chu-toulouse.fr
Accepted Feb 25, 2020; Epub ahead of print Mar 11, 2020
Acta Derm Venereol 2020; 100: adv00123
Netherton syndrome (NS) is a rare autosomal-recessive syndromic ichthyosis with an estimated prevalence of 1 in 200,000 individuals worldwide (1, 2). NS is caused by mutations in the SPINK5 gene, which encodes serine protease inhibitor LEKTI (3). Patients usually present from birth with erythroderma and scaly skin, sometimes presenting as an ichthyosis linearis circumflexa. They also develop a characteristic hair shaft abnormality (trichorrhexis invaginata (TI)), which leads to short and brittle hair, various atopic manifestations (including eczematous lesions) and high levels of IgE. No curative or effective treatment is available. Treatment is symptomatic and is based mainly on skin care using emollients (4). Quality of life is often impaired because of the appearance of the skin and complications, such as pruritus and recurrent skin infections.
The presence of severe inflammatory vegetative lesions of the perineum is a rare, and not well-known, clinical feature of NS. To date, it has not been described in textbooks or case series. Only 3 patients with NS with this complication (without molecular analysis) have been reported in the literature: a male aged 14 years and 2 females aged 26 and 28 years. We report here a new case of this rare complication.
The patient was a 42-year-old man with non-consanguineous parents of French origin. He had two older sisters, both diagnosed with NS. The patient presented since birth with inflammatory scaly skin with ichthyosis linearis circumflexa, atopic manifestations (including recurrent eczematous lesions). Immunohistochemistry revealed an absence of LEKTI staining. Molecular analysis confirmed the diagnosis of NS, since the patient carried 2 heterozygous mutations in the SPINK5 gene: c.283-2A> T in intron 4 and c.2468dupA (p.Lys824GlufsTer3) in exon 26. These 2 mutations have been reported previously. The first mutation disrupts a well-conserved splice element and generates a premature stop codon. The second mutation leads to a frameshift and a premature stop codon. Both mutations predict null expression of the mutated SPINK5 alleles through accelerated mRNA decay or loss of function of truncated LEKTI polypeptides if any are translated in the patient (3).
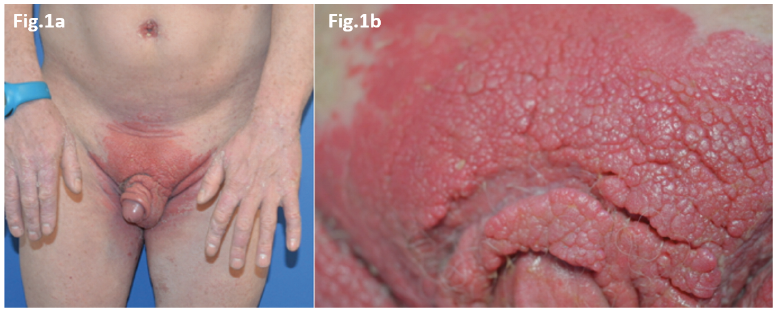
The patient’s usual treatment included emollients and antiseptics, due to recurrent skin infections. From the age of 35 years, he developed malodorous inflammatory vegetative plaques in the pubic area and, to a lesser extent, on the umbilicus, both of which worsened over time (Fig. 1). His 2 older sisters did not present with such lesions.
Fig. 1. Clinical photographs of a patient with Netherton syndrome (NS) with severe inflammatory vegetative lesions. (a) Inflammatory vegetative plaques on the pubic area; and on the umbilicus (b) Lesions on the pubic area.
Repeated bacterial swabs revealed abundant Streptococcus dysgalactiae. A fungal swab was negative. Viral swabs showed an absence of human papilloma virus (HPV) on PCR and on immunohistochemistry of a skin biopsy. Histological examination of the lesional skin revealed a hyperplastic and hyperkeratotic epidermis. In the superficial dermis a lymphocytic, histiocytic and plasmocytic infiltrate was observed underlining the lesion, associated with numerous dilated capillaries. There were also many neutrophils in the stratum corneum that evoked bacterial superimposed infection. No mycelium filaments were observed, indicating an absence of fungal infection. No signs of malignancy were seen.
Clinical and pathological evaluation led to a diagnosis of hyperplastic lesions, probably secondary to recurrent skin infections in the skin folds, which were prone to maceration.
As first-line treatment, antiseptics and oral antibiotics were prescribed, but with no improvement. Due to the massive hypertrophy of the lesions, carbon dioxide laser (CO2 laser) treatment was performed on a test area under local anaesthesia. This appeared to lead to good results, with decreasing hypertrophy, but the patient refused extensive treatment under general anaesthesia for the whole area. Botulinum toxin type A (BtxA) injections were then performed on a test area, with no significant improvement.
Comparison of the current case with the 3 cases reported previously in the literature reveal some similarities and differences, which help to better define this complication. Men and women may be affected by this complication of NS , and the vegetative inflammatory lesions are located in the pubic region. The lesions started later in our patient (at the age of 35 years), compared with the previously reported cases (from 14 to 19 years). The lesions increased over time and were disabling; they prevented 2 of the 3 reported patients from sitting comfortably (5, 6). Similarly to our patient, bacterial swabs were positive (Staphylococcus aureus and Streptococcus pyogenes) for 2 patients (5, 7) (but not mentioned for the third patient). Skin biopsies revealed similar results to our patient, with hyperplastic and hyperkeratotic epidermis with numerous capillaries, with no signs of malignancy. The terms Buschke-Lowenstein tumour (5) or giant condyloma of Buschke and Lowenstein were used for 2 patients (6, 7), but only the third patient (7) had HPV 52-specific DNA in the skin lesions (together with HPV 16-specific sequences in plane warts on her face and forearms).
The cause of these vegetative inflammatory lesions is poorly understood. Several factors can be hypothesized: firstly chronic inflammation of the skin, with episodes of repeated superimposed infections (which can be due to skin barrier defects) and maceration in the folds (8). Decreased cellular immunity or epidermal defence mechanisms were thought to be the cause for one patient (5). No immunological studies were performed in our patient, but he had no history of infections, suggesting immunocompetence.
Regarding the treatment of these hyperplasic lesions, the 3 patients reported previously were treated with electrosection or surgical excision, with excellent results. One of the 3 patients developed a relapse on the scars of the skin graft, which was treated with cryotherapy and imiquimod with good results. In our case, in a test area treated with CO2 laser the hypertrophy of the lesions decreased. This suggests that CO2 laser could be a
therapeutic option, but it has not been tested or discussed in the literature. BtxA injections have not been tested in NS. The hypothesis behind the use of BtxA in such a case was based on its effect on reducing sweating, and therefore maceration, which may play a role in the onset and maintenance of lesions. The toxin could also have anti-inflammatory effects (8). The effectiveness of BtxA has been shown in a case of Darier’s disease with moderate vegetative lesions on the back (9). In contrast, in our case, the injections were not effective, possibly because the lesions were already too severe and advanced.
In conclusion, vegetative inflammatory lesions of the perineum are very rare complications of NS. Management may be based on the control of superimposed skin infections and the destruction of hyperplastic and vegetative zones, with surgery or laser treatment. The effect of BtxA in the early stages is unknown.


 Click to show fullsize
Click to show fullsize