


1Department of Dermatology, Graduate School of Medicine, Kyoto University, 54 Shogoin-Kawahara, Sakyo, Kyoto 606-8507, and 2Department of Dermato-Oncology/Dermatology, National Hospital Organization Kagoshima Medical Center, Kagoshima, Japan. *E-mail: hontetsu@kuhp.kyoto-u.ac.jp
Accepted Feb 25, 2020; Epub ahead of print Mar 16, 2020
Acta Derm Venereol 2020; 100: adv00100
Erosive lichen planus is a severe variant of lichen planus that mostly affects the oral and genital area, and involvement of the extremities is rare (1, 2). Nivolumab (a programmed cell death protein-1 inhibitor) is now widely used for many kinds of cancer, and various immune-related adverse events including erosive lichen planus and lichen planus pemphigoides have been reported (3–5). We previously reported a case of erosive lichen planus on the extremities during combination therapy with nivolumab and radiation (6). In that earlier case, the skin lesions developed shortly after the radiation therapy. Herein, we report a similar case of erosive lichen planus on the extremities during treatment with nivolumab, in which lichen planus progressed to erosive lichen planus after radiation therapy.
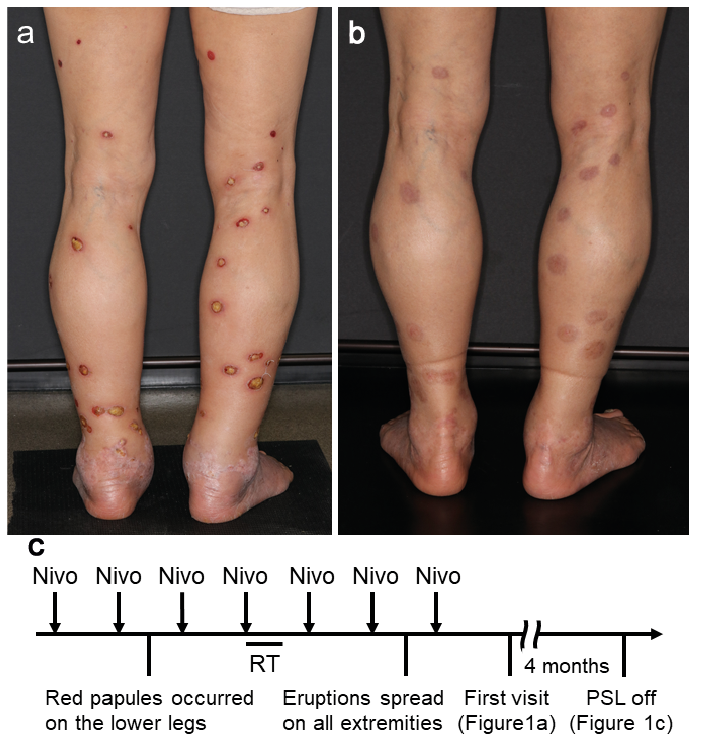
A 76-year-old woman with metastatic lung adenocarcinoma was treated with nivolumab therapy (240 mg/body, per two-week period). After two cycles of nivolumab, red papules occurred on the lower legs. Between the 4th and 5th cycles, radiation therapy for brain metastases was administered (28Gy/5Fr). Approximately 4 weeks after the completion of radiation therapy, the eruption gradually spread to involve all 4 extremities and became erosive with pain. At her first visit to our dermatology department, multiple erosive red macules/papules with yellowish crusts were present on all 4 extremities (Fig. 1a). Histological examination revealed band-like lympho-cytic infiltration beneath an hypertrophic epidermis with compact ortho-hyperkeratosis and hypergranulosis, as well as focal erosions (Fig. 2a). Vacuolar changes at the dermo–epidermal junction and apoptotic keratinocytes were also observed (Fig. 2b). These findings were consistent with erosive lichen planus. Blood tests were normal except for a slightly elevated C-reactive protein level (0.6 mg/dl). Administration of nivolumab was paused, and oral prednisolone therapy (1 mg/kg/day) was initiated with rapid clinical improvement. Nivolumab was then restarted, and prednisolone was tapered off over the next 4 months. At the time prednisolone was discontinued, only post-inflammatory pigmentation remained at the sites of previous lesions (Fig. 1b, c).
Fig. 1. Clinical findings. (a) Multiple erosive red macules/papules with yellowish crusts on the lower extremities at the first visit. (b) Clinical appearance when prednisolone was discontinued. Only post-inflammatory pigmentation remained at the affected sites. (c) Schematic presentation of the clinical course. Nivo: nivolumab; RT: radiation therapy; PSL: prednisolone.
Fig. 2. Histopathological findings. (a) Hematoxylin-eosin-stained specimens of the erosive papules on the right forearm. Band-like lymphocytic infiltration just beneath the hypertrophic epidermis with compact ortho-hyperkeratosis and hypergranulosis. Focal erosion is shown on the right (scale bar = 500 µm). (b) High magnification of the black square in (a). Vacuolar changes at the dermo–epidermal junction and apoptotic keratinocytes (scale bar = 100 µm).
Herein, we report a second case of multiple erosive lichen planus on the extremities during combination therapy of nivolumab and radiation presenting to our department. The patient’s clinical course showed that the initial eruptions on the lower legs only became erosive after radiation therapy. There are some similarities in the clinical course between our previous case and the current reported case: lichen planus, possibly induced by nivolumab, was preceding the radiation therapy and erosive lichen planus appeared around 4 weeks after radiation therapy and on extremities which had not been irradiated in both cases. We speculate that the activation of auto-reactive T cells might have been induced by the abscopal effects of radiation, leading to the development of erosive lichen planus (6). The two cases presented with different cancer types (breast cancer and lung cancer, respectively). This observation suggests that the radiation-induced activation of auto-reactive T cells can occur regardless of cancer type.
This report provides additional evidence of a relationship between erosive lichen planus and combination therapy of radiation and nivolumab. Clinicians should consider the potential risk of erosive lichen planus when starting radiation therapy in patients receiving nivolumab therapy, especially in cases in which lichen planus were caused by nivolumab therapy.
The authors have no conflicts of interest to declere.


 Click to show fullsize
Click to show fullsize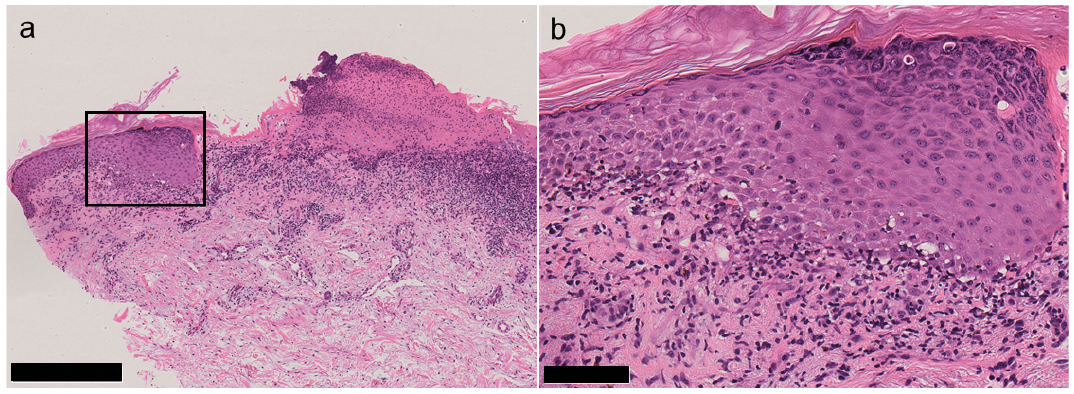 Click to show fullsize
Click to show fullsize