


1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, DK-2900 Hellerup, and 2Copenhagen Research Group for Inflammatory Skin (CORGIS), Hellerup, Denmark. E-mail: tanja.todberg@regionh.dk
Accepted Mar 18, 2020; Epub ahead of print Mar 19, 2020
Acta Derm Venereol 2020; 100: adv00118
Prurigo nodularis (PN) is a chronic skin disease, characterized by severe pruritus and multiple hyperkeratotic nodules often located on the extensor part of the upper and lower extremities (1).
The pathogenesis of PN is unknown; however, various hypotheses have been proposed including: increased level of substance P (a neuropeptide and a well-known mediator of pruritus) in the small nerve fibres in the dermis (2, 3); upregulation of nerve growth factor (NGF) in the dermis, leading to modulation of the small nerve fibres (4); and increased levels of interleukin-31 (IL-31) in the blood (5).
PN is defined as a subtype of chronic prurigo and is considered to be a distinct condition, which may originate in underlying comorbidities, such as atopic dermatitis (AD), neurological or systemic diseases (6).
PN is often burdensome to patients, due to severe pruritus leading to reduced quality of life (QoL), lack of sleep, and negative impact on everyday life (7). The existing treatments include topical corticosteroids, zinc dressing treatment, ultraviolet B (UVB), immunosuppressants, gabapentin, antidepressants, and thalidomide, all with limited effect. Overall, there is a need for effective treatments, as a large part of the existing therapies are unable to reduce disease severity and are associated with a poor safety profile (8).
In clinical trials, treatment with the phosphodiesterase-4 (PDE4) inhibitor (apremilast) has resulted in significant reduction in pruritus in AD and psoriasis (9, 10). The aim of this pilot-study was to evaluate the efficacy of apremilast in patients with PN.
A total of 10 patients (5 women) with PN were enrolled in the study. Mean ± SD age was 61.7 ± 10.0 years. All patients had lesions on at least arms and legs and 6 had previously received systemic therapy. Table SI shows the patient characteristics.
Seven patients completed the study, one of whom took a 4-week sunny vacation during week 5, thus data from week 4 for this patient was carried forward, although the patient completed the study. Three patients withdrew consent or were excluded before week 16; one at week 11 due to intermittent fever, and 2 at week 10, both due to lack of effect.
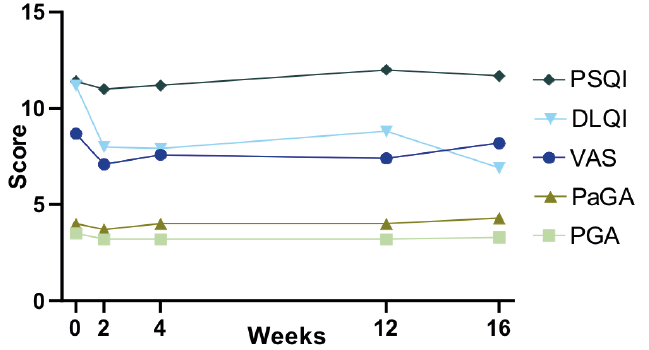
Patients experienced only minor or no reduction in pruritus; 3 patients had an improvement in visual analogue scale (VAS) pruritus ≥ 3 points, with a mean VAS at baseline of 8.7 ± 0.9 to 7.4 ± 2.4 at week 12. Overall, there was no clinical improvement following treatment with apremilast from baseline to the end of the trial, thus none of the 10 patients had an improvement in Physician Global Assessment (PGA) ≥ 2 points, with a mean PGA at baseline of 3.5 ± 0.5 to 3.2 ± 0.8 at week 12 (Table SI and Fig. S1). None of the patients showed an improvement in Patient Global Assessment (PaGA) ≥ 2 points, with a mean PaGa at baseline of 4.0 ± 0.7 to 4.0 ± 0.9 at week 12. Two patients had an improvement in DLQI ≥ 4 points, with a mean DLQI at baseline of 11.2 ± 6.8 to 8.8 ± 7.5 at week 12. One patient had an improvement in PSQI ≥ 3 points, with a mean PSQI at baseline of 11.4 ± 4.9 to 12.0 ± 5.2 at week 12 (Fig. 1). None of the patients had an increase in BDI compared with baseline.
No severe adverse events were observed. For 5 patients an adverse event was registered, with diarrhoea, nausea, and abdominal pain being the most frequent. In one patient recurrent fever was registered.
Cytokines or chemokines were investigated in biopsies from the patients. In 2/6 and 1/6 biopsies from week 12 data were missing for IL-31 and IL-22, respectively. None of the investigated cytokines or chemokines changed significantly during treatment with apremilast; however, a tendency to a decrease in concentrations at week 12 compared with baseline was seen for IL-6, IL-10, IL-31, tumour necorsis factor (TNF)-α, INF-γ, CCL2, and CCL3. The Th17-derived cytokines, IL-17 and IL-22, were almost unchanged (Fig. S2).
Fig. 1. Change in visual analogue scale (VAS) – pruritus, Physician Global Assessment (PGA), Patient Global Assessment (PaGA), Dermatology Life Quality Index (DLQI), and Pittsburgh Sleep Quality Index (PSQI) over a period of 16 weeks of apremilast treatment in patients with prurigo nodularis (PN). End of treatment was at week 12. For data from 4 of the 10 patients the last observation was carried forward from week 4 due to drop-outs.
This study found that 12 weeks of treatment with apremilast did not reduce pruritus in most patients (70%), thus no improvement was found in QoL or quality of sleep. Furthermore, apremilast was unable to clinically reduce the severity of PN. These results were supported by no significant changes in concentrations of cytokine or chemokine.
In a study by Samrao et al. (9), pruritus in patients with AD was significantly reduced within the first 2 weeks after initiation of apremilast. A rapid reduction in pruritus has also been observed in patients with psoriasis soon after initiation of apremilast (11). In the current study 3 of the 10 patients experienced a reduction in pruritus ≥ 3 points, which was reported as early as 2 weeks after receiving apremilast; however, no clinical improvement or no significant change in cytokines was seen in these patients.
The pathogenesis of PN is poorly understood, and only a few molecular mediators of PN have been identified, it is possible that apremilast is unable to suppress the key molecules mediating PN. Apremilast is a PDE-4 inhibitor, which increases the intracellular level of cyclic adenosine monophosphate. The anti-pruritic effect of apremilast in AD and psoriasis may be explained by the modulation of a wide range of proinflammatory mediators, such as IL-22, IL-23, IL-31, IFN-γ, TNF-α and an upregulation of the anti-inflammatory mediator IL-10 (9, 11). In many pruritic skin diseases IL-31 is thought to induce pruritus, and it has also been found to be expressed in PN lesions (12, 13). A tendency was found towards a reduction in the concentration of IL-31; however, this was not significant. In agreement, IL-31 may not be as important in PN, as described earlier (5). This is supported by a recent trial by Zhong et al. (14), showing that IL-31 was expressed significantly more in patients with PN who have a history of AD compared with patients with PN and no history of AD.
This study found that IL-10, an anti-inflammatory cytokine, was decreased, although this was not significant. This is in line with a trial by Schafer et al. (15), in which patients with psoriatic arthritis were treated with apremilast and a decrease in IL-10 was observed during the initial 16 weeks of treatment despite amelioration of arthritis symptoms.
The strengths of this study were: this is the first trial to evaluate the efficacy of apremilast in a group of patients with moderate to severe PN. The efficacy of apremilast was evaluated using both clinical parameters and by measuring changes in expression of cytokines.
Study limitations include: this was a small study with only 10 patients, 3 of whom did not complete the trial. Furthermore, the study was designed as an unblinded proof-of-concept study with no placebo-controlled group.
In conclusion, this study found that 12 weeks of treatment with apremilast did not reduce pruritus in a majority of patients with PN, with no improvement in QoL or sleep. Furthermore, the clinical severity of PN and expression of cytokines were unchanged with this treatment.
Funding statement: Celgene Corporation provided funding for this investigator-initiated trial. Celgene Corporation was not involved in any portion of the study design, data collection, data analysis, manuscript preparation or review process, or in the decision to submit the manuscript for publication.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize