


1Department of Clinical Immunology, Næstved Hospital, Health Sciences Faculty, University of Copenhagen, 2Department of Dermatology, Zealand University Hospital, Roskilde, Health Sciences Faculty, University of Copenhagen*, and 3Department of Dermatology and Allergy Centre, Odense University Hospital, University of Southern Denmark, Odense, Denmark
*Part of the European Reference Network on Rare and Undiagnosed Skin Disorders
#Shared senior authorship.
Hidradenitis suppurativa is a chronic skin disease characterized by inflammation and disfiguring scarring in the intertriginous body areas. Hidradenitis suppurativa is associated with overweight and impaired quality of life. This study sought to describe Body Image Quality of Life (BI-QoL) in patients with hidradenitis suppurativa and to compare it with patients with other skin diseases (controls). A total of 285 participants were recruited, 141 with hidradenitis suppurativa and 144 controls, at the Department of Dermatology at Zealand University Hospital, Denmark (during 2017–18). The Danish “Body Image Quality of Life Inventory” questionnaire measured BI-QoL. Patients with hidradenitis suppurativa had significantly lower mean BI-QoL than controls: Hidradenitis suppurativa BI-QoL (standard deviation; SD) –0.87 (0.98) vs. control BI-QoL (SD) 0.01 (1.11), p < 0.001. Predictors of negative BI-QoL were hidradenitis suppurativa, increased body mass index, female sex, symptoms of depression, and body mass index moderated by hidradenitis suppurativa. These data suggest that BI-QoL is impaired in patients with hidradenitis suppurativa compared with patients with other skin diseases after adjusting for confounders.
Key words: hidradenitis suppurativa; body image; quality of life; patient-reported outcome measures.
Accepted Mar 18, 2020; Epub ahead of print Mar 20, 2020
Acta Derm Venereol 2020; 100: adv00107.
Corr: Pernille Lindsø Andersen, Department of Dermatology, Zealand University Hospital, Roskilde, Health Sciences Faculty, University of Copenhagen, Sygehusvej 5, DK-4000 Roskilde, Denmark. E-mail: pehso@regionsjaelland.dk
People with skin diseases often have a negative self-image compared with healthy persons. Hidradenitis suppurativa is a chronic skin disease leading to boils and scarring, mainly in the armpits and groins. Patients with hidradenitis suppurativa are often overweight and have a reduced quality of life. This study investigated whether patients with hidradenitis suppurativa had a more negative self-image compared with patients with other skin diseases. The results showed that, even after taking into account other important factors related to self-image, e.g. body mass index, sex, age, and symptoms of depression, hidradenitis suppurativa influenced self-image more negatively than did other skin diseases.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease, characterized by recurrent painful and inflamed nodules, abscesses, fistula formation, and disfiguring scarring in the intertriginous body areas, e.g. the axillae and groin (1, 2). The prevalence of HS is 0.10–2.10% in the US and in Denmark. (US: 0.10-0.13%, Denmark: 1.8–2.10%). (3–6). It usually presents in early adulthood and is associated with obesity and affects females more frequently than males (7–9). The HS-associated symptoms of pain and suppuration appear to be linked to reduced health-related quality of life (HR-QoL), psychological distress, low self-esteem, depression, anxiety, and fear of stigmatization (10–12). HS may also affect the patient’s sexual health (13, 14) due to its location (15). Sexual health is furthermore affected by psychological factors, such as the person’s perception of their own physical appearance (16).
Body image (BI) is the perception of self-image related to physical characteristics; it is associated with psychosocial functioning. Quality of life (QoL) may be influenced by BI, but to different extents depending on the context (17). In 2001, Cash & Fleming developed the Body Image Quality of Life Inventory (BIQLI) as an assessment tool to evaluate the impact of BI on QoL in different contexts, e.g. perception of personal adequacy, meeting new people, enjoyment of sex life, etc. (17). BI is impaired in dermatological patients with, for example, psoriasis, systemic lupus erythematosus (SLE) and in patients with head and neck cancer (HNC) (18–20).
In 2018, BI was studied in a limited population of patients with HS compared with healthy controls. This study found evidence to suggest that patients with HS have a poorer BI compared with healthy controls and, furthermore, suggested BI as a potential outcome measure in HS studies (21).
The aim of the current study was to describe BI in patients with HS in greater detail and, in particular, the relative impact of HS compared with patients with other dermatological diseases.
Participants were randomly recruited during outpatient visits at the Department of Dermatology, Zealand University Hospital; Roskilde, Denmark (during the period Oct 2017 – July 2018) as part of another survey study (22). Patients (over 18 years of age) with a variety of other dermatological diagnoses than HS were recruited from the general outpatient clinic. Two dermatologists (PLA and RMN) performed the data collection. Patients completed the questionnaires while waiting to be seen in the clinic. The questionnaires included data on age, weight, smoking, education level, and marital status.
The impact on QoL due to BI was measured using the validated Danish version of the “Body Image Quality of Life Inventory” questionnaire (BIQLI) (23, 24). BIQLI uses a 7-point bipolar scale, from highly negative impact to highly positive impact (from –3 to +3). It examines 19 contexts or life domains where BI plays a significant role, e.g. “when I meet new people”, etc. (17, 23). The overall BI-related QoL is calculated as a mean of the 19 life domains in the questionnaire, resulting in a mean BIQLI score. In the following, the concept of BI-related QoL is referred to as BI-QoL.
Symptoms of depression and anxiety were measured using the Hospital Anxiety and Depression Scale (HADS). HADS provides a score that categorizes patients as either normal (0–7 points (p)), borderline abnormal (8–10 p) or abnormal (11–21 p) with regard to depression and anxiety, respectively (25). Using the HADS definitions, patients were grouped as those without symptoms of depression (0–10 p) or patients with symptoms of depression (11–21 p) Patients were furthermore grouped as either not having symptoms of anxiety (0–10 p) or with symptoms of anxiety (11–21 p).
Statistics
The sample size was calculated based on a minimum detectable mean difference in BI-QoL of 0.5 between HS and other dermatological disorders. With a common standard deviation (SD) of 1.4, a confidence level (CI) of 0.95 and a power level of 0.8, the required sample size per group was 124 participants.
The difference in mean BI-QoL between HS and control patients was assessed using independent samples t-test. The difference in BI-QoL score in each domain was assessed using Mann–Whitney
U test. To investigate other potential predictors of BI-QoL, a multivariate analysis was performed with the predictors: age, sex, body mass index (BMI), HS, symptoms of depression and anxiety. A hierarchical approach was used, where step 1 included age, sex and BMI (based on the literature; 19, 26, 27). Other predictors were added step by step. Because depression and anxiety are traditionally correlated (28), this correlation in our data was tested using Pearson correlation considering a coefficient > 0.4 as strong (29). A moderated multivariate analysis (MMA) assessed whether moderation of other predictors by HS occurred. Likewise, a hierarchical method was used based on the preliminary multivariate model and correlation of BI-QoL with the interaction terms (HS × age, HS × sex, HS × BMI, HS × symptoms of depression). Multicollinearity in regression models was assessed by variance inflation factors (VIF) < 10, and tolerance > 0.2.
p-values < 0.05 were considered significant and corrected using Holm Bonferroni correction. All statistics were performed using IBM® SPSS® Statistics version 25 for Windows.
Results are presented with means and SD or medians with percentiles (interquartile range (IQR)) depending on normality, as assessed by histograms.
Ethics
Surveys do not require institutional review board approval according to Danish law. Data collection was registered by the Danish Data Protection Agency (REG-165-2017). The study follows the STROBE guidelines for reporting observational studies.
A total of 285 patients were recruited in a dermatological outpatient clinic as a convenience sample. The HS patient population comprised 138 patients with active disease (at least one flare during the past 6 months), and the control population included 147 patients with dermatological conditions other than HS. Non-responders were not registered. Other conditions than HS included a variety of diagnoses representing the case-mix of the clinic. The largest groups were psoriasis (n = 38), dermatitis (n = 15), and malignant neoplasms (n = 10). A detailed overview of the diagnoses is shown in Table SI. Quality control of the control population diagnoses revealed that 3 patients had HS, and were subsequently included as such in the statistical analyses. Thus, our study population consisted of 141 patients with HS, and 144 patients with other dermatological conditions.
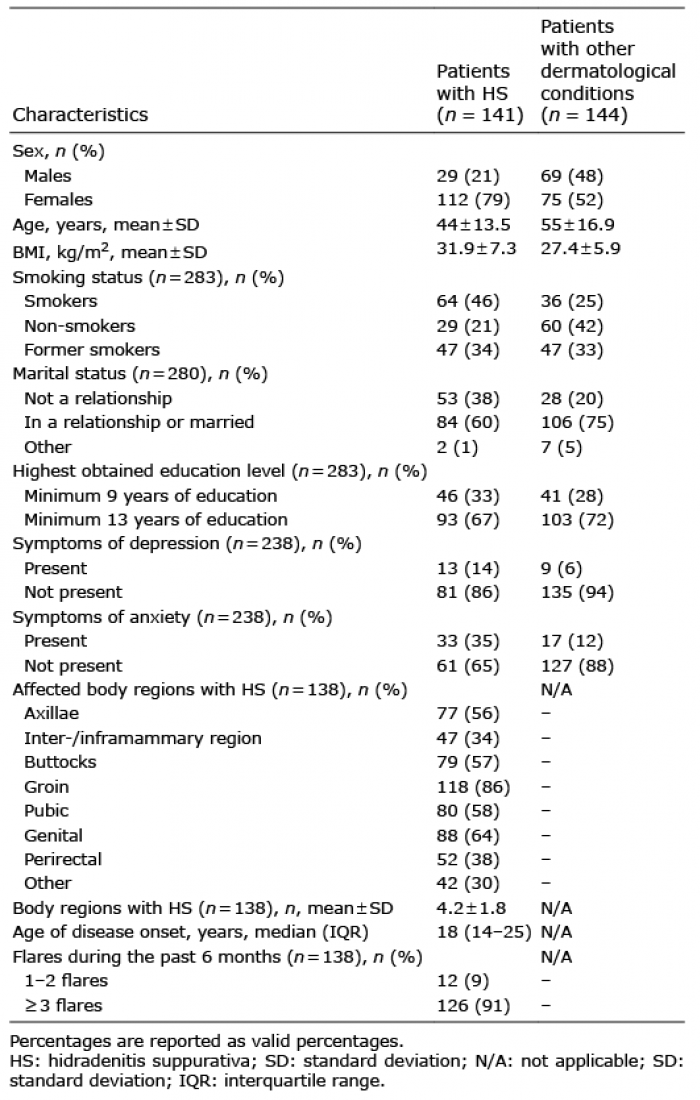
Of the patients with HS, 112 (79%) were female, whereas 75 (52%) of the control patients were female. The mean ± SD age varied from 44 ± 13.5 years in the HS group to 55 ± 16.9 years in the control cohort. The mean ± SD BMI in the HS group was 31.9 ± 7.3 kg/m2, and 27.4 ± 5.9 kg/m2 in the control group. According to the HADS definitions, the proportion of patients with symptoms of depression was 13/94 (14%) in the HS group and 9/144 (6%) in the control group (Table I). Clinical characteristics of patients with HS are also shown in Table I. The most frequently affected body region was the groin, which was affected in 118/138 (86%) patients.
Table I. Study population
Patients with HS had a significantly lower mean ± SD BI-QoL than patients with other skin diseases (controls): HS mean BI-QoL –0.87 ± 0.98 and control mean BI-QoL 0.01 ± 1.11, p < 0.001. The difference was particularly pronounced in domains regarding sexuality. In both item 11 “feelings of acceptability as sexual partner”, and item 12 “enjoyment of sex life”, patients with HS had highly significantly lower BI-QoL than controls: median HS BI-QoL (IQR) of –2 (–3;0) compared with median control BI-QoL of 0 (–1;0), both p < 0.001 (Table II).
Table II. Body Image Quality of Life Inventory items and their corresponding scores in patients with hidradenitis suppurativa (HS) and controls with other dermatological conditions
The multivariate analysis revealed that significant predictors of BI-QoL were age, sex, BMI, HS, and symptoms of depression. Anxiety, marital status and educational level were insignificant and excluded, as they did not significantly improve the model (model 1, Table III). There was no substantial risk of multicollinearity (mean VIF 1.16 and tolerance > 0.74). Symptoms of depression and anxiety were, however, significantly correlated with each other: Pearson coefficient 0.41 (95% CI 0.24–0.54), p < 0.001.
Table III. Multiple regressions on predictors for Body Image Quality of Life scores
The MMA investigated potential moderation effects by HS on the predictors; sex, age, BMI, and symptoms of depression. Forced entry order was determined by Pearson correlation coefficient of each interaction term and BI-QoL. The coefficients were: HS × BMI: –0.378, HS × sex: –0.376, HS × age: –0.297 and HS × symptoms of depression: –0.255. All correlations were significant, p < 0.001. Significant moderation was evident for HS*BMI, which significantly improved the model (model 2, Table III). This model was the best fit to our data, R2=0.32.
The interaction between HS and BMI is illustrated in Fig. 1. The figure shows the linear decrease in BI-QoL per increasing BMI point for patients with HS (red) and controls (blue), respectively.
Fig. 1. Mean Body Image Quality of Life (BiQoL) by body mass index (BMI) in patients with hidradenitis suppurativa and those with other dermatological diseases (controls). Moderation of BMI by hidradenitis suppurativa (HS): The impact of increase in BMI point on BiQoL in patients with HS and controls. Patients with HS at a certain BMI value has a negative BiQoL compared with controls with the same BMI value.
Skin diseases are associated with impaired BI. This study compared BI-QoL in patients with HS and in those with other dermatological diseases, to assess the relative impact of HS. Patients with HS had a significantly impaired BI compared with patients with other skin diseases. Presence of HS had a significantly negative impact on BI-QoL with a coefficient of –1.40 (95% CI –2.30 to –0.51), p = 0.002, when adjusting for other factors (model 2, Table III). This is in accordance with the results of Schneider-Burrus et al., who, however, compared HS patients with healthy controls assessed by another BI-QoL measurement tool (the Frankfurt Body Concept Scale) (21).
Items relating to sexuality (item 11–12) were the predominantly affected items in patients with HS. BI-QoL item 11 “acceptability as sexual partner”: Median HS patients (IQR): –2 (–3;0) and controls: 0 (–1;0), and item 12 “enjoyment of sex life”, HS: –2 (–3;0) and controls: 0 (–1;0) (Table II). Impaired sexual health in patients with HS has been documented previously by Janse et al., who found that impairment seems to be greater in females than in males. The authors hypothesized that both physical appearance and psychological factors play a role for sexual health (15). Our data suggest that BI is important for patients with HS and their perception of self-image in sexual contexts. This may be due partly to the clinical presentation in our cohort, in which the majority of the patients were affected in the groin, pubic, and genital areas (Table I). A previous study found that the anogenital localization of HS impairs quality of life substantially, while HS in exposed skin increases feeling of stigma (30).
Younger females were relatively over-represented in the HS group. Consequently, the skewed age and sex distribution between the 2 groups may affect these results. Other skin diseases also negatively affect the self-perception of sexual attractiveness. A qualitative study of patients with psoriasis found that these patients report concerns about meeting people of the opposite sex and starting new sexual relations (18). Our results indicate that HS may affect sexual BI-QoL more negatively than do other skin diseases. This finding supports the evidence provided by a European multicentre study, which found that sexual impairment is markedly present in patients with HS compared with other dermatological conditions. This study furthermore found that sexual impairment is strongly correlated with symptoms of depression (31).
In our sample, age had a marginally positive impact on BI-QoL, age coefficient 0.02 (95 % CI 0.01–0.03); p < 0.001 (Table III). This finding is in accordance with previous findings in healthy women and patients with SLE, who also experience a positive body appreciation with increasing age (19, 27). It may be speculated that improved coping and likelihood of established long-lasting sexual relationships may play a role in this context.
The current study found that increasing BMI negatively influenced BI-QoL, consistent with previous findings (17). In addition, we also demonstrated a significant interaction between BMI and HS, p = 0.020 (Fig. 1). Of 2 patients with the same BMI, the patient with HS has the most negative BI-QoL compared with the control patient. Furthermore, the effect of the interaction term HS × BMI 0.04 (95% CI 0.01 –0.07) illustrates that a patient with HS has a slightly less negative slope per increasing BMI point compared with a patient with another dermatological condition. Assuming a linear relationship, the 2 slopes do not intersect at BMI values < 70. However, outside of the mean ± SD BMI range of 29.7 ± 7.0 kg/m2, conclusions about the effect of BMI on BI-QoL should be drawn with caution, due to few observations outside this range.
In our sample, symptoms of anxiety and depression were correlated, with a Pearson correlation coefficient of 0.41. Thus, anxiety was excluded from our regression model, as it did not significantly improve the model.
In our population, patients with HS had a mean ± SD BI-QoL of –0.87 ± 0.98. Comparing these results with previous studies of patients with SLE and those with HNC, patients with HS seem to have a more impaired BI-QoL. Both patients with SLE and patients with HNC (pre- and post-treatment) had positive mean ± SD BI-QoLs: SLE BI-QoL 0.8 ± 1.3, and HNC BI-QoL 0.6–0.9 ± 1.13–1.21 (32, 19). In our study, the control group also had a lower mean BI-QoL than patients with SLE and HNC: Control mean ± SD BI-QoL 0.01 ± 1.11. Thus, our Danish dermatological population had a more negative BI-QoL than the populations in the aforementioned studies from the USA, which may partly be explained by cultural differences (33).
The current study investigated whether social factors, i.e. marital status and educational level, would have an impact on BI-QoL. Correlations between social factors and BI have been suggested previously (20). The current study found no significant associations between social factors and BI-QoL when adjusting for other predictors (age, sex, BMI, HS, and symptoms of depression) (Table SII).
Implications of negative BI include low self-esteem and impaired disease coping (19, 34, 35). It was found that patients with HS have a poor BI compared with those with other dermatological conditions. BI concerns can be addressed using cognitive behavioural therapy (CBT) (36). CBT is furthermore very effective in the treatment of depression and anxiety (37). As a considerable fraction of HS patients exhibit symptoms of anxiety and depression, these patients might benefit from CBT to improve their BI as well as symptoms of psychiatric comorbidities.
Strengths and limitations
The major strengths of our study are the usage of a validated measurement tool to examine BI-QoL, the sample size, and the investigation of social factors. However, the Danish BIQLI questionnaire is validated only for patients with infective endocarditis, which might influence the results.
It may further be speculated that both HS and control patients in a hospital setting have more severe disease, thereby limiting the generalizability of our absolute findings. We would, however, argue that the balanced sampling reflects the relative impact of HS even outside a hospital setting. Non-responders were not registered. Though, the motivation for participation in surveys is probably the same for dermatological patients regardless of their diagnosis. Another limitation of our study is the study design based on questionnaire data. Thus, the data collection did not include clinical severity assessment of the study participants, which is worthy information to evaluate more accurately the BI-QoL within different dermatological disorders.
Conclusions
BI-QoL is more impaired in patients with HS than in those with other dermatological conditions. The high BMI of many patients with HS is a potential confounder for BI-QoL, but after adjusting for HS’s moderation of BMI, patients with HS still have a worse BI-QoL than patients with other dermatological conditions.
Financial support: PTR received support from the Region Zealand Research Found. PLA received a PhD grant from LEO Foundation and Naested, Slagelse and Ringsted Hospital’s Research Fund. GB Jemec has received honoraria from AbbVie, Coloplast, Pfizer, Pierre Fabre, Inflarx, MSD, Novartis and UCB for participation on advisory boards, and grants from Abbvie, Leo Pharma, Novartis, Janssen-Cilag, Regeneron, UCB, and Sanofi for participation as an investigator, and received speaker honoraria from AbbVie, Galderma, and Leo Pharma.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize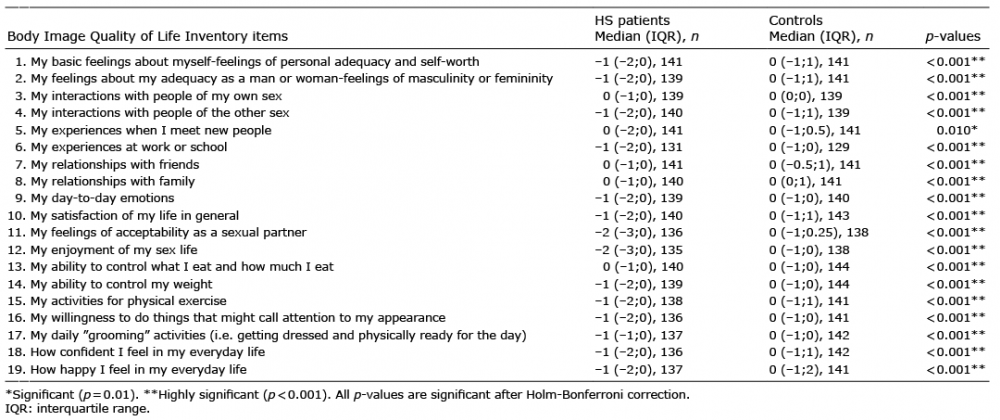 Click to show fullsize
Click to show fullsize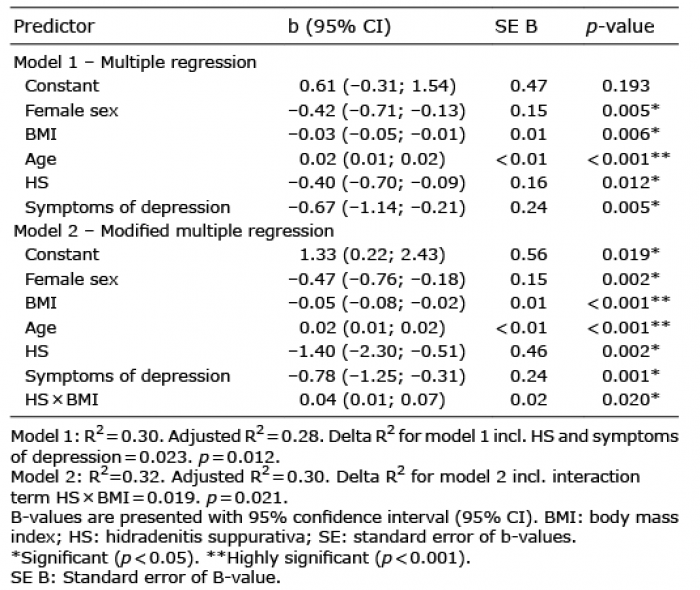 Click to show fullsize
Click to show fullsize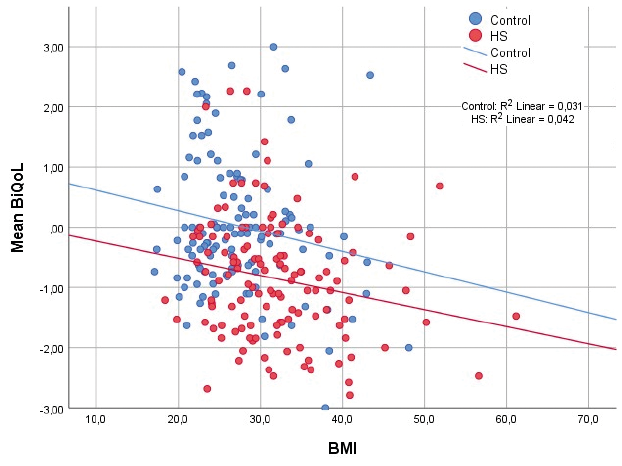 Click to show fullsize
Click to show fullsize