


Department of Dermatology, Nara Medical University School of Medicine, 840 Shijo, Kashihara, Nara 634-8522, Japan. E-mail: fumim@naramed-u.ac.jp
Accepted Mar 18, 2020; Epub ahead of print Mar 20, 2020
Acta Derm Venereol 2020; 100: adv00102
Drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms (DIHS/DRESS) is a type of severe adverse drug reaction associated with multi-organ involvement and the reactivation of human herpesvirus 6 (HHV-6) (1, 2). Previously, we reported that CD134 (OX40), an HHV-6 cellular receptor (3), was preferentially upregulated on CD4+ T cells in patients with DIHS during the acute stage of the condition, compared with its expression level in other drug eruptions, such as maculopapular exanthema (MPE) and Stevens-Johnson syndrome (SJS) (4). We suggested that the upregulation of CD134 might be necessary for CD4+ T cells to become permissive to HHV-6 entry, and that CD134-expressing CD4+ T cells might facilitate the spread of HHV-6 in DIHS (4). In this study, we found that OX40L, the ligand of CD134, is also preferentially expressed on peripheral blood mononuclear cells (PBMCs) in patients with DIHS. Moreover, the percentage of CD134-expressing CD4+ T cells was correlated with laboratory parameters associated with Th2-type immune responses, such as the serum thymus and activation-regulated chemokine (TARC) level and the eosinophil count. Since OX40–OX40L ligation is known to promote Th2 differentiation (5), CD134 might function not only as an HHV-6 receptor (3), but also as a driver of Th2-type immune responses in DIHS.
This study included 12 patients with DIHS (7 males and 5 females; median age 59 years, range 16–74 years) and 9 patients with MPE (4 males and 5 females; median age 71 years, range 36–88 years) and was carried out with the approval of the ethics committee of Nara Medical University. Acute-stage blood samples were obtained between 2 and 18 days after the onset of eruptions in DIHS (mean 9.1 days after onset), and between 0 and 8 days after the onset of MPE (mean 3.1 days after onset). PBMCs were isolated from whole blood by Ficoll density gradient centrifugation (GE Healthcare, Little Chalfont, UK) and divided into 2 aliquots, one for real-time PCR and one for flow cytometry. Sera were separated from whole blood by centrifugation and stored at –80°C until use. HHV-6 DNA was detected by real-time PCR following DNA extraction from PBMCs. Serum TARC levels were measured by enzyme-linked immunosorbent assays (Shionogi, Osaka, Japan). For cell surface staining of PBMCs, FITC-conjugated anti-CD3 (clone UCHT1), -CD134 (ACT35), PE-conjugated anti-OX40 Ligand (ik-1), -CD3 (UCHT1), and APC-conjugated anti-CD4 (RPA-T4) antibodies (BD Pharmingen, Franklin Lakes, NJ, USA) were used. Experiments were performed on a FACSCalibur flow cytometer (Becton Dickinson, Franklin Lakes, NJ, USA) and analysed using CellQuest software (Becton Dickinson).
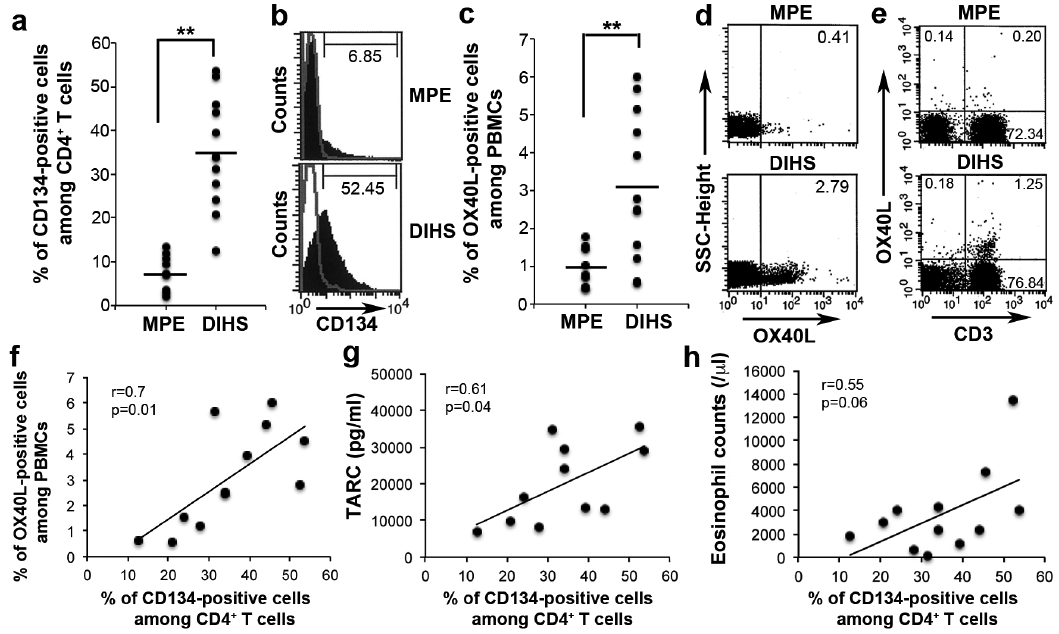
Consistent with our previous study (4), the percentage of CD134-expressing CD4+ T cells was markedly higher in the patients with DIHS in the acute stage than in the patients with MPE (Fig. 1a, b). The mean percentage of CD134-expressing cells among CD4+ T cells was 35.0 ± 3.65% (mean ± standard error of the mean (SEM), range 12.6–53.7%) in the patients with DIHS, whereas it was 7.56 ± 1.35% (2.08–13.2%) in patients with MPE (Fig. 1a). OX40L expression was also upregulated in the patients with DIHS in the acute stage, while it was almost undetectable in the patients with MPE (Fig. 1c, d). The mean ± SEM percentage of OX40L-positive cells among the PBMCs was 3.07 ± 0.56% (range 0.56–6%) in the patients with DIHS, whereas it was 0.53 ± 0.18% (0.41–1.79%) in patients with MPE (Fig. 1c). Both CD3+ T cells and non-T cells, including antigen presenting cells, expressed OX40L in the patients with DIHS (Fig. 1e). The percentage of OX40L-positive PBMCs decreased in the late stage of DIHS. The percentage of CD134-expressing CD4+ T cells was correlated with the percentage of OX40L-positive PBMCs in the patients with DIHS (Fig. 1f).
Fig. 1. Upregulation of CD134 and OX40L in patients with drug-induced hypersensitivity syndrome (DIHS) during the acute stage. (a) CD134 expression was upregulated on CD4+ T cells in patients with acute-stage DIHS. Horizontal lines indicate the mean value for each group. Data were compared using the Student’s t-test (**p < 0.01). (b) Representative flow cytometric plots of CD134 expression on the CD4+ T cells shown in (a) are presented. Peripheral blood mononuclear cells (PBMCs) were stained for CD3, CD4, and CD134 and analysed via flow cytometry. The cells within the lymphocyte gate were subjected to CD3+CD4+ gating. Thin line represents the results of the isotype control staining, and the numbers on the histograms indicate the percentage of CD134-positive cells. (c) OX40L expression was upregulated on PBMCs in patients with acute-stage DIHS. Horizontal lines indicate the mean value for each group. Data were compared using Student’s t-test (**p < 0.01). (d, e) Representative flow cytometric plots of OX40L expression on the PBMCs shown in (c). PBMCs were stained for OX40L and CD3 and analysed by flow cytometry. (d) Percentages of OX40L-positive cells within the lymphocyte gate. (e) Representative CD3 vs. OX40L plots for the cells within the lymphocyte gate. Numbers in the quadrants indicate the percentage of the lymphocyte population. (f–h) Correlations between the percentage of CD134-expressing CD4+ T cells and (f) the percentage of OX40L-expressing cells in PBMCs, (g) serum thymus and activation-regulated chemokine (TARC) levels, and (h) eosinophil counts. Pearson’s correlation coefficients were calculated for these correlations.
We next determined whether CD134 expression was correlated with the serum levels of TARC, a Th2-associated chemokine. We previously reported that serum TARC levels were markedly elevated in patients with DIHS during the acute stage of the condition (6, 7) and correlated with the severity of the disease (8). Consistent with this, the serum TARC levels of the patients with DIHS were markedly increased (mean ± SEM 20,016.8 ± 3,251.3%, range 6,971.5–35,485.9%, normal range < 450 pg/ml). We found that the percentage of CD134-expressing CD4+ T cells was positively correlated with the serum TARC level (Fig. 1g) and eosinophil count (Fig. 1h) in the patients with DIHS. There were no correlations between the percentage of CD134-expressing CD4+ T cells and other laboratory parameters, including the severity score of skin and mucosal lesions (8), the percentage of atypical lymphocytes, the serum level of alanine transaminase or creatinine, and the HHV-6 DNA copy number.
In DIHS/DRESS, eosinophilia (1, 2), increased plasma interleukin (IL)-5 levels (9), and increased serum levels of Th2-associated chemokines, including TARC (6, 7) and macrophage-derived chemokine (10), have been documented. These results suggest that DIHS/DRESS is polarized toward Th2-type immune responses. Our results showed that the percentage of CD134-expressing CD4+ T cells and OX40L expression were increased in DIHS and were correlated with the serum TARC level and eosinophil count in the acute stages of the condition. These findings indicate that increased expression of CD134 and OX40L and the resultant OX40 engagement might lead to Th2 generation in DIHS. Thus, the current study might provide pathomechanistic insights into DIHS. From a therapeutic point of view, since no effective therapeutic agents for HHV-6 have been developed, the results of the current study suggest that the development of drugs targeting CD134 might represent a useful prophylactic/therapeutic approach for DIHS/DRESS.
The authors thank Ayako Yamamoto for technical assistance. This study was supported in part by a Grant-in-Aid for Scientific Research (KAKENHI) to FM.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize