


1Clinical Epidemiology Unit, IDI-IRCCS, Rome, Italy, Departments of Dermatology: 2Justus Liebig University, Giessen, Germany, 6ULB Erasme Hospital, Brussels, Belgium, 7Zealand University Hospital, Roskilde, University of Copenhagen, Copenhagen, Denmark, 11Oslo University Hospital and Institute of Clinical Medicine, University of Oslo, Oslo, 12Stavanger University Hospital, Stavanger, Norway, 13Wroclaw Medical University, Wroclaw, Poland, 15University Hospital Miguel Servet. IIS Aragon, Zaragoza, Spain,17Cardiff University School of Medicine, Cardiff and 20University Hospital of Brest, Brest, France, 3Department of Psychology, University of Zaragoza, Zaragoza, Spain, 4Department of Public Health, Hedmark University College, Elverum, 5National Center for Dual Diagnosis, Innlandet Hospital Trust, Brumundal, Norway, 8Department of Dermatology and Allergology, University of Szeged, Szeged, Hungary, 9Department of Medical Psychology and Psychotherapy, Medical University of Graz, Graz, Austria, 10Department of Health, Medical and Neuropsychology, Leiden University, Leiden, The Netherlands, 14Department of Psychiatry and Psychosomatics, I. M. Sechenov First Moscow State Medical University (Sechenov University); Mental Health Research Center, Moscow, Russia, 16University of Health Sciences, Etfal Training and Research Hospital, Dermatology, Istanbul, Turkey, 18Department of Pharmacy, Pharmacology and Postgraduate Medicine, School of Life & Medical Sciences, University of Hertfordshire, Hatfield, UK, and 19Institute of Medical Psychology, Justus Liebig University, Giessen, Germany
#These 2 authors contributed equally to the study.
Pain and discomfort are important symptoms in dermatology. The aim of this cross-sectional, multicentre study was to describe the prevalence of pain/discomfort and its associations in patients with several dermatological conditions across 13 European countries. The outcome was the prevalence of pain/discomfort according to a question of the EQ-5D questionnaire. Data collected from November 2011 to February 2013 were complete for 3,509 consecutive outpatients. Moderate or extreme pain/discomfort was reported by 55.5% of patients and 31.5% of controls with no skin conditions. The highest proportions were reported by patients with hidradenitis suppurativa (92.9%), leg ulcer (81.4%), prurigo (80%) and lichen planus (75.6%). Pain/discomfort was associated with older age, low educational level, clinical severity, flare on scalp or hands, itch, depression, anxiety, low quality of life, and thoughts of suicide. It is important to enquire specifically about pain/discomfort during clinical consultations and to address it when planning a patient’s care.
Key words: dermatology; discomfort; EQ-5D; pain.
Accepted Apr 2, 2020; Epub ahead of print Apr 6, 2020
Acta Derm Venereol 2020; 100: adv00120.
Corr: Jacek C. Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Pain and discomfort are relevant issues affecting patients with various dermatoses. This study included a large group of outpatients from 13 European countries, and revealed that pain and discomfort frequently affect dermatological patients, especially those with hidradenitis suppurativa, leg ulcer, prurigo and lichen planus.
Pain and discomfort may be experienced by patients with dermatological conditions (1, 2). Pain has been defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” (3). This definition is still current, as it clearly defines pain as a subjective experience. Moreover, it links pain to both the sensory systems’ physiology and to the neurobiology of emotions, and it specifies that pain is associated with a specific adequate stimulus (4). Pain is an important symptom to be aware of clinically, since it is associated with profound effects on many aspects of quality of life (QoL) in many diseases (5).
The concept of discomfort is less well defined than pain, and has a slightly different meaning in different languages. In English “discomfort” may be defined as “slight pain” (Oxford English Dictionary), as “a painful feeling in part of your body when you have been hurt slightly or when you have been uncomfortable for a long time” (Collins English Dictionary), but also as the “feeling of being uncomfortable physically or mentally” (Cambridge English Dictionary). In a study that aimed to create a questionnaire on discomfort of body skin (6), 7 items were identified from consumers and confirmed by dermatologists’ experience: stinging, itching, tightness and warming, reported by the patient, and dryness, redness and desquamation, evaluated by the dermatologist.
Skin conditions are frequently responsible for unpleasant sensory symptoms, most obviously itch. However, pain, burning, and fatigue are also present in a large proportion of patients with skin conditions (2, 7, 8). In particular, pain is often reported by patients with psoriasis, atopic dermatitis (AD), and leg ulcers (8–11). However, only a few studies have investigated pain in other skin conditions (2, 7, 12, 13). Also, the presence of other unpleasant sensations that contribute to discomfort, such as stinging, tightness and warming, has been rarely investigated. This emphasizes the need to explore in more detail the presence of unpleasant sensory symptoms in patients with a wide variety of skin conditions. To do this, we used the question from the EuroQoL-5D (EQ-5D) instrument that asks about the presence of pain/discomfort. The study was conducted in a large sample of patients with several dermatological conditions across 13 European countries.
This report presents data from a large, multicentre, epidemiological study on the psychological burden of skin conditions. Methods have been described previously in detail (14). In brief, consecutive patients were recruited from dermatological outpatient clinics in 13 European countries from November 2011 to February 2013. Each centre had to collect data on 250 patients and 125 controls. Patients’ inclusion criteria were: age 18 years and over; being able to read and write the local language; having provided written informed consent. Patients were excluded if they had severe psychiatric conditions. The control group was recruited among employees at each study centre. The inclusion criteria were: age 18 years or more and no presence of skin condition, having provided written informed consent.
Collected data
Each patient was clinically examined by a dermatologist, who also collected information on comorbidities. The clinical severity of the skin condition was evaluated by the physician as either “mild”, “moderate” or “severe”. Patients were asked to complete a questionnaire with socio-demographic data and several questionnaires on the psychological burden of skin conditions. The clinical evaluation and the patient’s self-assessment were independent of each other.
Evaluation of pain or discomfort: the EQ-5D
The EQ-5D (15) questionnaire allows measurement of health-related QoL across all medical fields and across the general population. It has been used in skin conditions (16, 17), showing a good overall validity, especially for psoriasis and psoriatic arthritis (16). The EQ-5D includes a visual analogue scale (VAS) for self-rated health state from “0” (worst imaginable health state) to “100” (best imaginable health state), and 5 questions on mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each question has 3 poss-ible answers. In this study we used data based on the question that asked subjects to rate “pain/discomfort” as either “I have no pain or discomfort” (score=0), or “I have moderate pain or discomfort” (score=1), or “I have extreme pain or discomfort” (score=2).
Depression and anxiety: the Hospital Anxiety and Depression Scale questionnaire
Symptoms of depression and/or anxiety in patients were evaluated using the Hospital Anxiety and Depression Scale (HADS) (18). It consists of 7 items assessing anxiety (HADS-A) and 7 assessing depression (HADS-D), each with 4 possible answers. For each dimension of anxiety and depression a person with a score of 0–7 is considered a normal case, 8–10 a borderline case, and 11–21 a case in need of further examination or treatment. In this paper we describe a subject with a score of 11–21 as a “clinical case”, and with a score of 8–10 as a “borderline case”. Although the EQ-5D asks about depression and/or anxiety, this is only an exploratory question that does not distinguish between the 2 conditions; hence the need to also use HADS as a screening tool to identify depression or anxiety separately.
Quality of life: the Dermatology Life Quality Index
Dermatology-specific health-related QoL was assessed using the Dermatology Life Quality Index (DLQI) (19). It consists of 10 questions, with possible answers from 0 (“not at all”) to 3 (“very much”). The total score is obtained by adding the score of each item. The following score band descriptors have been validated (20): total score 0–1: no effect at all on patient’s life; 2–5: small effect on patient’s life; 6–10: moderate effect on patient’s life; 11–20: very large effect on patient’s life; and 21–30: extremely large effect on patient’s life.
Suicidal ideation
To assess suicidal ideation due to the skin condition, the item ‘’Have you ever thought of committing suicide because of your skin?’’ was included, with possible answers ‘’yes’’ or ‘’no’’.
Sample size
As previously described (14), the statistical power was calculated on the basis of the prevalence of depression in the general population, estimated as 9%, and the expected prevalence in the dermatological population being higher (21). To identify a difference with a power of 0.80 and alpha=0.05 between a prevalence of depression of 9% in controls and 11% in cases, using a 1-sided test, 3,500 cases and 1,300 controls were needed (233 cases and 87 controls in each centre).
Statistical analysis
The answers to the “pain/discomfort” question of the EQ-5D were dichotomized into a variable “yes/no” by grouping the answers “I have moderate pain or discomfort” and “I have extreme pain or discomfort”. The frequency of pain/discomfort for the different dermatological conditions was calculated, and graphically represented by histograms. The group “psychodermatological diseases” included patients with factitial dermatitis, burning mouth, psychogenic itch, and trichotillomania. The association of pain with different variables was calculated: socio-demographic variables (sex, age, “living in the country of origin”, education, marital status, geographical region); clinical information (clinical severity of the skin condition, body site of the disease, presence of itch); presence of depression, presence of anxiety, suicidal thoughts, and DLQI score. The associations were analysed using odds ratios (ORs). Countries were grouped into Northern Europe (Denmark, Norway), Western Europe (Belgium, France, Germany, The Netherlands, UK), Eastern Europe (Hungary, Poland, Russia, Turkey), and Southern Europe (Italy, Spain). Logistic regression models were tested to estimate the degree of association of each variable of interest with pain/discomfort, while adjusting for all the other variables in the model. The dichotomous variable “pain/discomfort yes/no” was introduced in each model as the dependent variable. The independent variables were: sex, age, marital status, clinical severity, itch, depression, anxiety, and DLQI. Separate models were created for some diseases, selected on the basis of the number of patients (approximately 200 patients or more), i.e. psoriasis, eczema, non-melanoma skin cancer (NMSC), and acne. The diagnosis “eczema” included AD, eczema and hand eczema.
In total, 5,067 individuals agreed to participate; 3,651 patients and 1,416 controls. The participation rate was 79.9%. Of the initial 3,651 patients, 16 were excluded, 9 because they were too young and 6 because of missing data, leaving 3,635. Of the initial 1,416 controls, 57 were subsequently excluded because, in the questionnaire specific for controls, they reported being treated for a skin disease, leaving 1,359. Information on pain/discomfort was available in 3,509 patients (96.5%). In the study population 43.6% were males, and the mean ± standard deviation age was 46.9 ± 17.2 years.
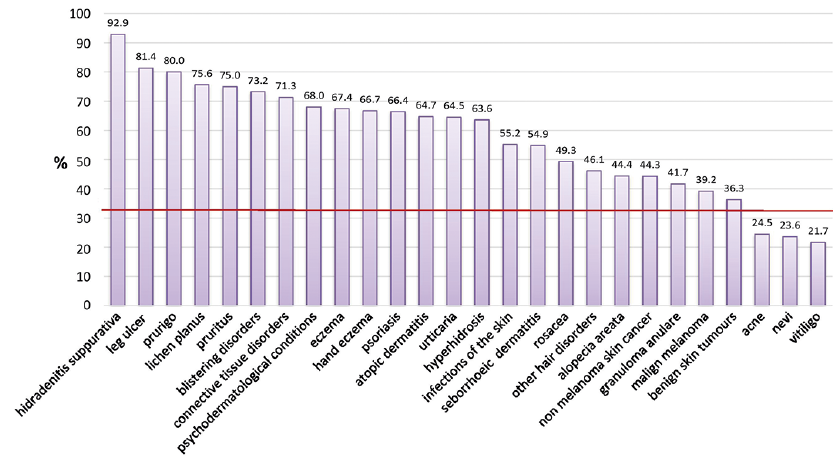
The disease was evaluated by the clinician as severe in 16.6% of patients, moderate in 45.3%, and mild in 38.1%. Clinical or borderline depression were present in 10.1% and 14.0% of patients, respectively (total prevalence of depression in cases 24.1%); clinical or borderline anxiety in 17.2% and 19.9%, respectively (total prevalence of anxiety in cases 37.1%). In patients, the presence of some pain/discomfort was reported by 49.7% of patients and extreme pain/discomfort by 5.8% (total prevalence 55.5%). In controls, these figures were 30.1% and 1.4%, respectively (total prevalence 31.5%). The prevalence observed in controls was quite high; however, it is consistent with that reported in other studies (22). Furthermore, while the overall prevalence rate ratio (PRR) of moderate or extreme pain/discomfort was 1.8, when considering only extreme pain, the PRR was 4.1. In the 4 geographical areas PRR of moderate or extreme pain/discomfort was quite homogeneous, varying from 1.5 in Western Europe to 2.0 in Southern Europe. The highest proportion of presence of pain/discomfort (Fig. 1) was reported by patients with hidradenitis suppurativa (92.9%), leg ulcer (81.4%), prurigo (80%), lichen planus (75.6%), and pruritus (75.0%). Patients reporting pain/discomfort were less frequently those with vitiligo (21.7%), naevi (23.6%), and acne (24.5%). The conditions with a higher prevalence of frequent pain/discomfort were prurigo (28.0%) and hyperhidrosis (27.3%). Pain/discomfort was associated with older age, low educational level, high clinical severity, flare on scalp or hands, and itch (Table I). It was less frequently reported by single patients or by patients with a flare on the face. As to mood disorders (Table II), the presence of borderline/clinical depression and anxiety, as well as thoughts of suicide, were strongly associated with pain/discomfort. The association between pain/discomfort and QoL increased substantially with increasing impairment in QoL, ranging from an OR of 2.18 for a small impairment of QoL up to 23.48 for a major impairment.
The multivariate models for single diseases (Table III) confirmed the strong association between pain/discomfort and low QoL in psoriasis, eczema, acne, and NMSC. Pain/discomfort was also significantly associated with the presence of anxiety in psoriasis, eczema, and acne. In psoriasis and acne, pain/discomfort was associated with itch. Age was positively associated with pain/discomfort in psoriasis and eczema.
Fig. 1. Prevalence of positive answers (“moderate” or “extreme”) to the question on the presence of pain/discomfort of the EuroQoL-5D (EQ-5D) questionnaire in different skin conditions. Data from 3,509 outpatients collected from November 2011 to February 2013. Red line indicates the prevalence of positive answers in controls.
Table I. Prevalence of patients experiencing pain/discomfort in the study population according to demographic and clinical variables
Table II. Prevalence of patients experiencing pain/discomfort in the study population according to psychological conditions and quality of life
Table III. Logistic regression models for psoriasis, eczema, acne, and non-melanoma skin cancer (NMSC) patients, with pain/discomfort from the EuroQoL-5D (EQ-5D) questionnaire as the dependent variable
In this study of a large number of dermatology outpatients, moderate or extreme pain/discomfort was reported by 55.5% of patients. The proportion was particularly high in patients with hidradenitis suppurativa, leg ulcer, prurigo, and lichen planus. Between 65% and 75% of patients with pruritus, blistering disorders, connective tissue disease, psychodermatological conditions, eczema, and pruritus experienced some or extreme pain/discomfort. These results are not directly comparable with those of previous studies, where only the dimension of pain was considered, or pain and discomfort were measured separately. For example, in a study of over 1,500 dermatological outpatients who used a specific questionnaire for neuropathic pain (7), skin pain was reported by 36.4% of patients. In another study (2), 23% of patients with skin diseases experienced pain evaluated with a VAS. Ljosaa et al. (9) reported a prevalence of 42% of skin pain and 37% of discomfort in patients with psoriasis. On the basis of these results we can speculate that approximately half of our patients reporting pain/discomfort actually had pain, and half had discomfort. This would be consistent with the results of the previous studies on the prevalence of pain in skin conditions.
In the current study, pain/discomfort was strongly associated with poor QoL, as also previously observed (1). We reported a significant association between pain/discomfort and both depression and anxiety. The association with anxiety was particularly strong, since it was significant even in the multivariate models when considering single conditions, such as psoriasis, eczema, and acne. It has been observed, in the musculoskeletal domain, that anxiety disorders, as well as other psychological symptoms, are associated with high levels of perceived pain (23, 24). According to the biopsychosocial model (25), there might be a bidirectional relationship between anxiety/depression and pain, including skin pain (26). Concerning the association with suicidal thoughts in the current study, the number of subjects was not large enough to know if suicidal thoughts were due to pain, especially as suicidal ideation was reported by a relatively small proportion of the participants. However, we have run a crude analysis for the association between pain and suicidal ideation, stratified by diagnosis. In general, we have observed that suicidal ideation was more frequent among patients reporting higher levels of pain/discomfort.
In the current study, pain/discomfort was more frequent in older patients. This could be due also to the presence of comorbidities. In fact, the EQ-5D question does not specify if pain/discomfort is due to a skin condition. This lack of specificity and presence of co-morbidities may also explain the reporting of pain/discomfort in conditions such as naevi and vitiligo.
Almost all patients with hidradenitis suppurativa reported moderate or extreme pain/discomfort. It is known that, among inflammatory dermatoses, hidradenitis suppurativa has the highest impact on QoL (27), presumably because of the frequent presence of symptoms, such as pain. Our results emphasize the importance of taking into account pain management when planning a treatment strategy for this condition (28).
Various studies with different samples and assessment methods have reported a range of percentages of patients with psoriasis experiencing pain. For example, in one study (8) 26% of psoriasis patients reported pain (up to 50% for psoriatic arthritis), but in that study a stringent definition of pain as experienced “often” or “all the time” was adopted. In the study by Ljosaa et al. (9), skin pain was reported by 42% of psoriasis patients, while in our study moderate or extreme pain/discomfort was reported by 66.3% of patients. In patients with psoriasis, pain was also strongly associated with the presence of itch. This is not surprising, since mechanisms that underlie the development of chronic itch and pain may overlap to a great extent (29).
Pain is present in patients with AD (30). Patients may scratch their skin, resulting in skin barrier disruption and painful erosions, but pain could also be partly related to neurogenic inflammation (31). In a previous study (11), pain and itch occurred together in 78% of patients with AD. It was observed that the presence of pain had an important impact on QoL, since it interfered with sleep, leisure activities, and daily living. In our study population, pain was strongly associated with older age and with anxiety.
There has been little investigation of pain in acne. In our population 24.5% of patients reported that they had experienced moderate or extreme pain/discomfort, which was associated with itch, anxiety, and poor QoL. We suggest that in acne pain is directly caused by the inflammatory lesions and may be exacerbated by trauma or manual interference with the lesions.
Pain was also present in patients with NMSC. In a previous study (32), 57.5% of patients with squamous cell carcinoma reported spontaneous pain, and 80% reported pressure-related pain. Patients with basal cell carcinoma may also report pain, in particular as a major side-effect of topical photodynamic therapy (33). In our study, pain/discomfort was reported by 44.3% of patients with NMSC. Pain is more frequently associated with squamous cell carcinoma than other skin cancers (34) and is frequently (but not exclusively) associated with perineural invasion.
Other studies have used the EQ-5D questionnaire in dermatology (17, 35), but none have previously analysed a single dimension. The analysis of single items of a questionnaire may give important information on the burden on patients of a particular symptom or psychosocial problem on patients (36). Our previous European group paper presenting EQ-5D data (17) focused on a different study question, i.e. the comparison between dermatological cases and non-dermatological controls.
A possible issue of the use of the question about pain/discomfort concerns the translation of the term “discomfort” into different languages. The word “discomfort” does not have such a well-defined meaning as “pain”. The number of words that express a sensation, such as tingling, prickling and stinging, differs depending on the language used (37). High-standard validated translations and cross-cultural adaptations are crucial to ensure equivalence of meaning, as previously shown in a comparative study on pain (38). However, the original selection of the dimensions of the EQ-5D questionnaire was done on the basis of a survey of patients and the general population, and of a detailed review of other generic health measures (39). The dimension of pain/discomfort was chosen taking into account the translation issues. Moreover, the combination of the 2 terms has been used previously; for example, in a study on patients with psoriasis (40).
A strength of this study is that it includes data from a multicentre European initiative aimed at providing insight to the impact of skin diseases on QoL and psychological well-being. This involved the collection of a large amount of data using a single study design with standardized procedures and common research tools. There were no differences among regions in the prevalence of pain, which may indicate that it is the skin condition, and not factors specific to each country (health policy, climate, etc.), that influences the degree of pain/discomfort.
A limitation of the current study is the cross-sectional design, which does not allow determination of the direction of the associations between pain/discomfort and the other variables. Thus, for example, it is not possible to know if people with depression thereby experienced more pain/discomfort, or if the presence of more pain/discomfort may cause depression in some people. Another limitation of the study is that the EQ-5D question does not distinguish pain and discomfort. This may hinder comparisons with the results of other studies where pain or other unpleasant sensations are investigated separately.
In conclusion, pain/discomfort is a common symptom in several skin conditions, and is associated with a poor QoL, mood disorders and anxiety. Dermatologists should be aware of this, should enquire specifically about these very common symptoms in their routine clinical practice, and, when necessary, refer patients to a pain management specialist. In particular, the EQ-5D is a simple instrument that can be used in clinical practice to obtain information on specific aspects, such as pain/discomfort.
Funding sources and conflicts of interest: FS and DA are partially supported by the “Progetto Ricerca Corrente RC 4.1” of the Italian Ministry of Health, Rome, Italy. FS acted as a consultant for Abbvie, Janssen, Eli Lilly, and Pierre Fabre; JS is a consultant and Advisor for AbbVie, Celgene, Dignity Sciences, Leo Pharma, Novartis, Pierre-Fabre, Menlo Therapeutics, Sienna Pharmaceuticals and Sandoz, Investigator for AbbVie, Actelion, Amgen, GSK, Janssen, Merck, Novartis, Regereron, Takeda, Trevi, Speaker for AbbVie, Actavis, Astellas, Janssen, Leo Pharma, Novartis, SunFarm, Sandoz, Eli Lilly; AYF is joint copyright owner of the DLQI, Cardiff University and AYF receive royalties, AYF is a member of a Novartis advisory board.


 Click to show fullsize
Click to show fullsize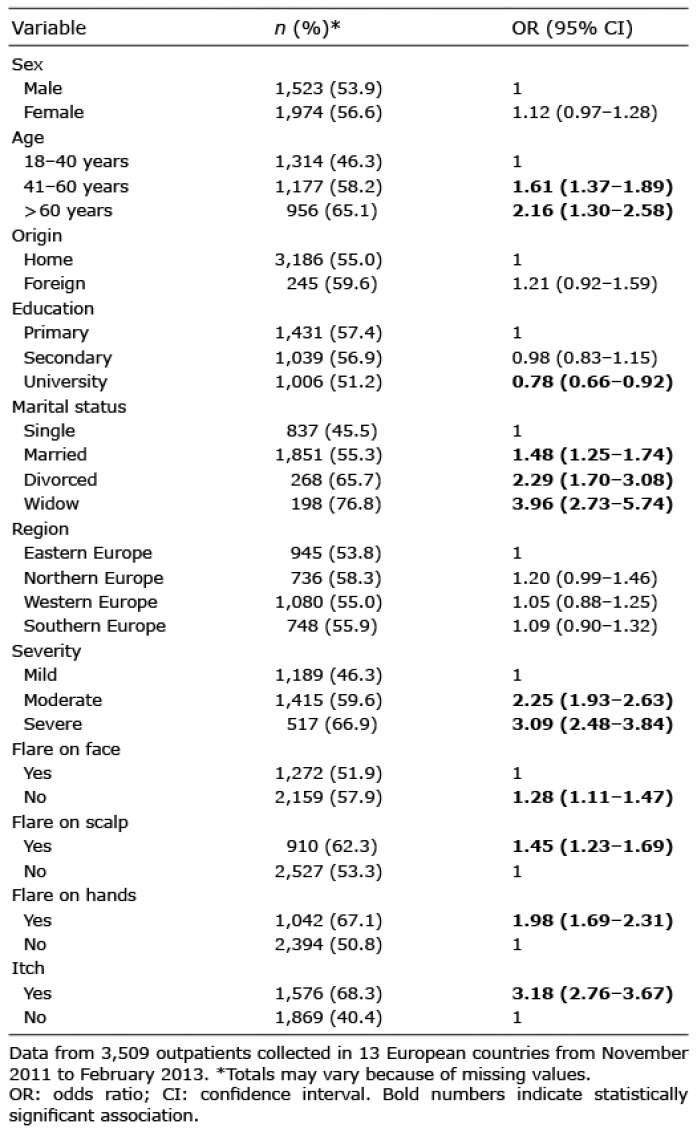 Click to show fullsize
Click to show fullsize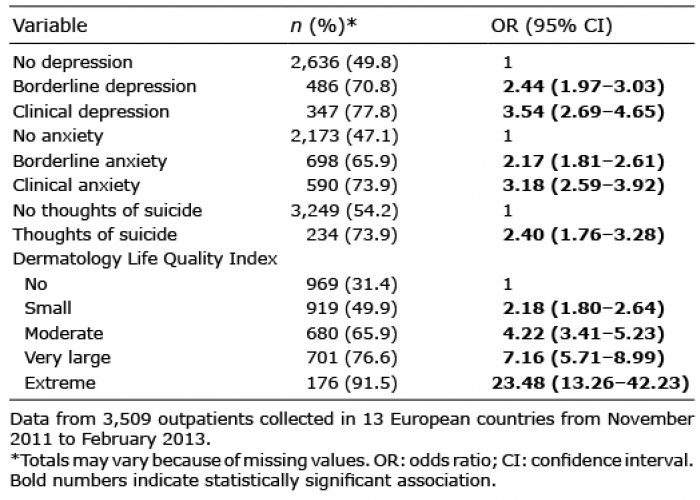 Click to show fullsize
Click to show fullsize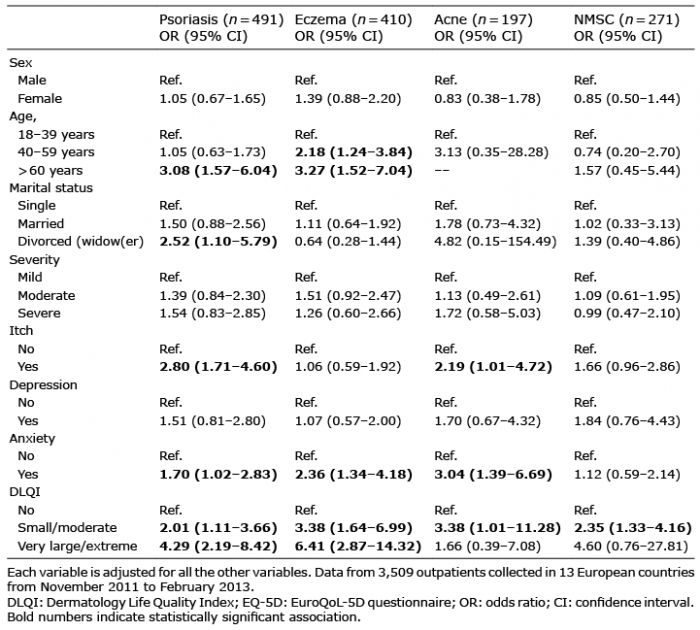 Click to show fullsize
Click to show fullsize