


1Department of Dermatology and Cutaneous Surgery, and Itch Center University of Miami Miller School of Medicine, Miami, USA, and 2Clinical Trials and Epidemiology Research Unit, Singapore
Research suggests that itch and psychiatric diseases are intimately related. In efforts to examine the prevalence of psychiatric diagnoses in patients with chronic itch not due to psychogenic causes, we conducted a retrospective chart review of 502 adult patients diagnosed with chronic itch in an outpatient dermatology clinic specializing in itch and assessed these patients for a co-existing psychiatric disease. Psychiatric disease was identified and recorded based on ICD-10 codes made at any point in time which were recorded in the patient’s electronic medical chart, which includes all medical department visits at the University of Miami. Fifty-five out of 502 (10.9%) patients were found to have a comorbid psychiatric diagnosis based on ICD-10 codes. The most common psychiatric diagnoses were anxiety disorders (45.5%), followed by major depressive disorder (36.4%). There was no significant association of any specific type of itch to a particular psychiatric disorder. No unique itch characteristics were noted in patients with underlying psychiatric diagnoses.
Key words: itch; psychiatric; anxiety; depression; chronic; psycho-logic.
Accepted Apr 21, 2020; Epub ahead of print Apr 21, 2020
Acta Derm Venereol 2020; 100: adv00169
Corr: Gil Yosipovitch, MD, Department of Dermatology and Cutaneous Surgery, and Itch Center University of Miami Miller School of Medicine, 1600 NW 10th Ave, RMSB 2067B, Miami, FL 33136, USA. E-mail: yosipog@gmail.com
The primary aim of this study was to examine the prevalence of psychiatric diagnoses in patients with chronic itch that is not due to psychogenic causes. The secondary aim of this study was to determine whether psychiatric diagnoses have any correlation to specific itch characteristics such as itch intensity, or if there are any psychiatric-specific diseases this patient population is more prone to. This information will not only allow us to better understand the potential factors underlying the presentation of chronic itch, but also allow us to provide these patients with more holistic and complete assessment and treatment in the future.
Studies have shown evidence of a correlation between chronic itch and mental health problems (1), and in recent years, research has begun to further explore the intimate relationship between itch and the psychological disorders. For example, a study found that 70% of hospitalized pruritus patients who were administered global rating scales on psychiatric, social, and professional functioning presented with symptoms suggestive of psychiatric illness (2). Chronic pruritus has been correlated to increased psychologic burden, with higher incidences of psychiatric disturbances and suicidal ideations reported in chronic itch patients compared to non-chronic itch patients (3, 4). Furthermore, our group has previously found that there is a significant component (up to 32%) of chronic itch without rash amongst hospitalized psychiatric patients (5). This raises the question whether chronic non-psychogenic itch is associated with psychiatric comorbidities.
The primary aim of this study was to examine the prevalence of psychiatric diagnoses in patients with chronic itch that is not due to psychogenic causes. The secondary aim of this study was to determine whether comorbid psychiatric diagnoses have any correlation to specific itch characteristics such as itch intensity, or if there are any psychiatric-specific diseases this patient population is more prone to.
Five-hundred and two adult patients diagnosed with chronic itch conditions between November 2017 and December 2019 who were seen at the Miami Itch Center clinic were included in the study. Chronic itch was defined as itch lasting > 6 weeks and etiologies included dermatologic, systemic, or neuropathic, as well as idiopathic causes of itch. These patients were identified based upon completion of an electronic medical record (EMR) itch questionnaire part of the clinic assessment. The EMR itch questionnaire contains questions related to duration, characteristics, and factors associated with the patient’s itch (see Table I). All chronic itch diagnoses were made by a board-certified dermatologist with an expertise in itch (GY). Chronic itch diagnoses were grouped into 6 major categories as shown in Table II. Patients who were diagnosed with psychogenic itch, as defined by the French Psychodermatology Group as an itch disorder where psychological factors play an evident role in triggering the itch, were excluded from the analysis (6).
Table I. Itch questionnaire variables
Table II. Categorization of itch-related dermatologic diagnoses
This sample of 502 patients was then divided into those who have comorbid psychiatric disease versus those who have no comorbid psychiatric disease based solely on EMR data. Identification of patients with psychiatric illness was made possible by a shared electronic medical record system which contains each patient’s medical history from all department visits at the University. Patients who were diagnosed with a psychiatric disease at any point in time were identified based upon a designated psychiatric ICD-10 code. Of note, all cases were manually examined to assure that neuropathic causes of itch were not coded as a psychiatric comorbidity.
Statistical analysis
All statistical analyses were performed using SPSS 25.0. Association between factors were determined by χ2 tests for categorical variables and ANOVA for comparison of means. A p-value < 0.05 was considered significant.
Five-hundred and two adult patients (191 males and 311 females) with chronic itch due to dermatologic, systemic, and neuropathic causes filled out the EMR itch questionnaire during their clinic visits. Forty-one of these patients were diagnosed with more than one disease process contributing to their chronic itch. The prevalence of each dermatologic diagnosis can be found in Table III. Of these patients, 55 were found to have a comorbid psychiatric diagnosis based on recorded ICD-10 codes (10.9%).
Table III. Prevalence of itch-related dermatologic diagnoses
Psychiatric diagnoses
Of the 55 chronic itch patients with a comorbid psychiatric diagnosis, 19 were diagnosed with multiple ICD-10 codes. The most common psychiatric diagnosis amongst chronic itchy patients was anxiety disorders, which accounted for 25 patients (i.e. F41, 45.5%). Eighteen patients had a recurrent or single episode of major depressive disorder (F32 and F33, 36.4%), 9 patients had a reaction to severe stress or adjustment disorders (F43, 16.4%), 8 patients had sleep disorders not due to a substance or known physiological condition (F51, 14.5%), 5 patients had obsessive compulsive disorder (F42, 9.1%), 5 patients had substance-related disorders (F10, F11, F17, and F19, 9.1%), 4 patients had unspecified mood (affective) disorder (F39, 7.3%), 3 patients had attention deficit hyperactivity disorder (F90, 5.5%), and 2 patients had bipolar disorder (F31, 3.6%). Other disorders represented by a single patient each include mental disorders due to a known physiological condition (F06), psychological and behavioral factors associated with disorders/diseases classified elsewhere (F54), and other behavioral and emotional disorders with onset usually occurring in childhood and adolescence (F91).
Dermatologic diagnoses
There was no significant association in the observed chronic itch patients with any psychiatric diagnosis compared with those without a psychiatric diagnosis.
Chronic itch characteristics
No significant differences in itch characteristics as described in the itch EMR questionnaire (Table I) were noted amongst all chronic itch conditions between patients with comorbid psychiatric diagnoses versus those without.
Demographic information
The mean age of patients with psychiatric diagnoses (56.1 ± 16.2) did not differ significantly from those without comorbid psychiatric diagnoses (59.0 ± 19.4). Females were more likely to have a comorbid psychiatric diagnosis than males (12.5% vs. 8.4%, respectively), but this difference was not significant (p-value 0.15). Psychiatric diagnosis was significantly more associated with Hispanic patients (15.2%) than Non-Hispanic patients (8.3%) (χ2 5.87, p < 0.02).
This is the first large-scale study to examine the association of psychiatric comorbidity in an outpatient itch center in the United States. The prevalence of underlying psychiatric diseases is 10.9%. Previous studies using patient-reported questionnaires and interviews by psychosomatic experts determining psychiatric comorbidity in chronic itch patients elicited varied results. In a recent study conducted in hospitalized chronic itch patients in Germany, 580 chronic itch patients out of 6,374 who were suspected to have psychosomatic comorbidities were referred to psychiatric interviews, and among them, a high proportion of patients (77%) were diagnosed with at least one psychosomatic/psychiatric diagnosis according to ICD-10 code. Although this study uses a different methodology, we can extrapolate from the data that about 6.7% of patients with chronic itch in an inpatient setting have psychiatric comorbidity (7). The same lead author conducted a previous study demonstrating a significantly higher prevalence (>70%) of psychiatric symptoms among 109 consecutive hospitalized chronic itch patients (2). Finally, based on a recent large European study by Dalgard et al., it is clear that there is a significant association between the presence of chronic itch and clinical depression (accounting for 14.1% of dermatologic patients with itch versus 5.7% in dermatologic patients without itch) (8).
The lower prevalence of psychiatric disorders in chronic itch patients elicited from our database as compared to the aforementioned studies may relate to the fact that consistent with the general population (9, 10), psychiatric disorders in chronic itch patients are underdiagnosed. Whereas in previous studies patients were selected and thoroughly assessed for psychiatric comorbidity using trained interviewers as well as self-reported questionnaires, our study was limited to retrospective analysis of electronic data reflecting existing psychiatric diagnoses. These psychiatric diagnoses were either made secondary to the patient’s desire to seek psychiatric care, or due to obvious psychiatric symptoms as identified by a physician. Unfortunately, patients may either be hesitant to report symptoms which are often stigmatized, or they may not exhibit psychiatric symptoms that are not concerning enough to prompt a self-motivated clinical assessment. Various psychological conditions which may not be reflected by an ICD-10 code in our study were likely to be elicited through the lengthy interview process as well as self-reported patient questionnaires featured in the previous studies. It is likely that had each individual patient in our study been thoroughly assessed for psychiatric illness by means of a lengthy interview by trained specialists or through self-reported questionnaires, the prevalence of psychiatric disease in this study would be much higher. Importantly, the aforementioned studies did not exclude psychogenic itch from their analyses, which may also contribute to the increased prevalence of psychiatric illness elicited by these studies.
Itch characteristics such as 24-h itch severity or impact on sleep were not shown to be associated with any psychiatric comorbidity among all chronic itch conditions, including those in which itch is typically a significant and debilitating component of the disease (i.e. prurigo nodularis, atopic dermatitis, or psoriasis). It is possible that this lack of difference in itch characteristics may be related to the sample size of our study, as only 55 out of 502 patients were identified as psychiatric patients. However, our results are supported by the study of dermatologic patients with and without itch across Europe, where it was found that there was no significant association for chronicity and intensity of itch with psychosocial factors (8). In contrast, amongst the chronic pruritus patients that had a psychiatric comorbidity in the large study conducted in Germany, those that were found to have a comorbid psychiatric condition had significantly higher pruritus scores and longer durations of pruritus (7). Similarly, other studies have found that depression was significantly associated with itch severity (11, 12). Future studies should be conducted in order to further elicit this relationship.
Our study demonstrated that psychiatric diagnoses were significantly more prevalent in Hispanic patients (15.2%) than Non-Hispanic patients (8.3%). Although this association was found to be significant (p-value 0.02), our sample size was small, and a larger population sample is required in order to assess whether ethnicity actually plays a real role in the association between psychiatric illness and chronic itch. There was also a trend that females were more likely to have a comorbid psychiatric diagnosis than males (12.5% vs. 8.4%, respectively), but this difference was not statistically significant.
Conclusion
The connection between itch and psychiatric disorders has been well established. This statement is supported by studies assessing psychiatric comorbidities in chronic itch patients using patient-reported questionnaires, and also by the fact that psychological behavioral treatment and anti-depressant/anxiolytic medications have been shown to be beneficial in itchy patients beyond those with psychogenic itch or those with a pre-existing psychiatric diagnosis (13). Future studies should be conducted to assess the use of anxiolytic and antidepressant drugs in this population, as this could further suggest the association of subclinical psychiatric symptoms in chronic itch patients.
Conflict of interest: GY is Scientific Board Member of Menlo, Trevi, Sienna, Sanofi, Regeneron, Galderma, Pfizer, Novartis, Bayer, Kiniksa, Eli Lilly, Bellus, AbbVie. Research support by Pfizer, Sun Pharma, Leo, Menlo, Kiniksa. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize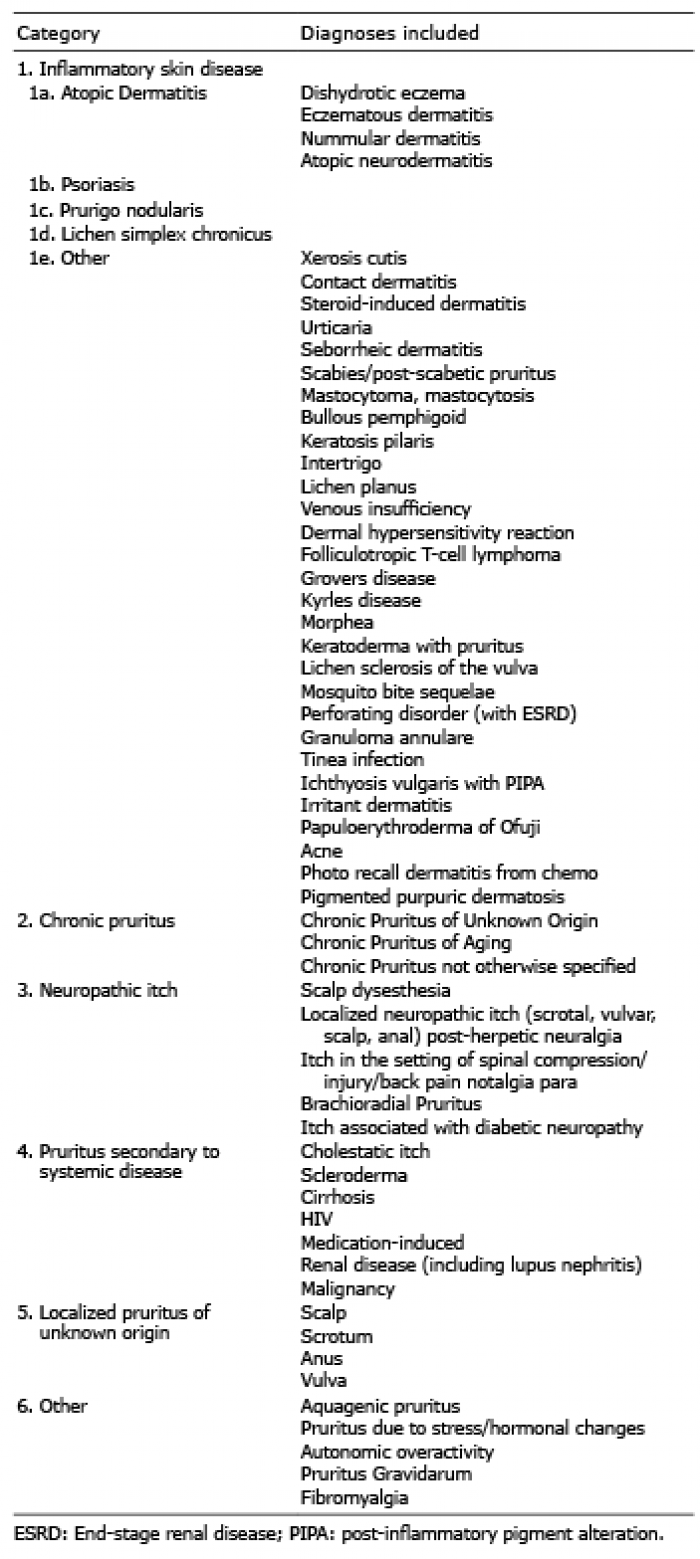 Click to show fullsize
Click to show fullsize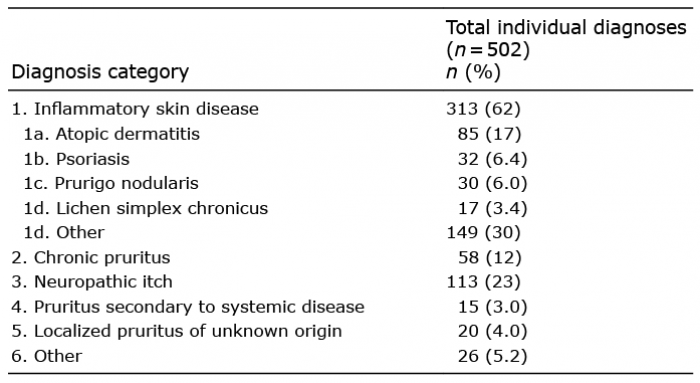 Click to show fullsize
Click to show fullsize