


1The George Washington University School of Medicine and Health Sciences, Washington, DC, 2Global Medical Affairs, Pfizer Inc., New York, NY, 3Global Product Development, 4Health Economics and Outcomes Research, 5Biostatistics, Pfizer Inc., Groton, CT, and 6Global Medical Affairs, Pfizer Inc., Collegeville, PA, USA
*At the time of the analysis.
Crisaborole ointment, 2%, is a nonsteroidal phosphodiesterase 4 inhibitor for the treatment of mild-to-moderate atopic dermatitis. This post hoc analysis pools results from 2 phase 3 studies (ClinicalTrials.gov, NCT02118766 [AD-301]; NCT02118792 [AD-302]) to evaluate crisaborole efficacy in patients ≥ 2 years with mild-to-moderate atopic dermatitis (per Investigator’s Static Global Assessment) using the Atopic Dermatitis Severity Index (ADSI) and percentage of treatable body surface area (%BSA). Patients were randomly assigned 2:1 to receive crisaborole (n = 1,016) or vehicle (n = 506) twice daily for 28 days. ADSI scores were the sum of pruritus, erythema, exudation, excoriation, and lichenification severity scores, each graded on a 4-point scale from none (0) to severe (3). Respective mean changes in ADSI score and %BSA at day 29 were (crisaborole vs. vehicle) −3.52 versus −2.42 (p < 0.0001) and –7.43 versus –4.44 (p < 0.0001). Crisaborole was effective in treating mild-to-moderate atopic dermatitis based on ADSI and %BSA.
Key words: crisaborole; atopic dermatitis; atopic dermatitis severity index; Investigator’s Static Global Assessment.
Accepted Apr 21, 2020; Epub ahead of print Apr 21, 2020
Acta Derm Venereol 2020; 100: adv00170.
Corr: Jonathan I. Silverberg, The George Washington University School of Medicine and Health Sciences, 2121 I St NW, Washington, DC 20052, USA. E-mail: JonathanISilverberg@gmail.com
Crisaborole is a nonsteroidal topical treatment for mild-to-moderate atopic dermatitis. In 2 large, identically designed phase 3 studies of patients with mild-to-moderate atopic dermatitis, significantly more patients treated with crisaborole achieved treatment success per the Investigator’s Static Global Assessment (ISGA) than patients treated with vehicle. This post hoc analysis confirms the effectiveness of crisaborole in alleviating atopic dermatitis severity using the measures Atopic Dermatitis Severity Index (ADSI) and percentage of treatable body surface area (%BSA).
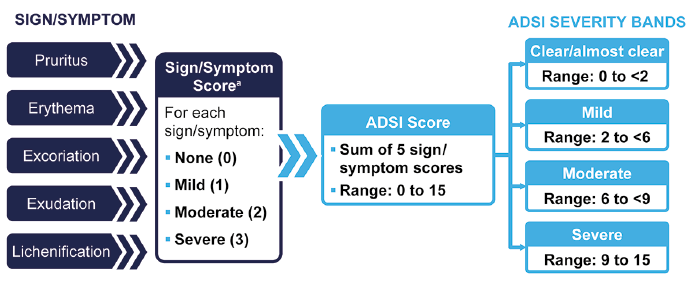
Atopic dermatitis (AD) is a common chronic inflammatory skin disease associated with itch (pruritus) and eczematous lesions (1, 2). Many tools assess AD outcomes, signs, and symptoms; however, standardization is lacking (3, 4). Some of the most commonly used disease severity measures include SCORing of Atopic Dermatitis (SCORAD), Eczema Area and Severity Index (EASI), Investigator’s (Static) Global Assessment (I[S]GA), and Six Area, Six Sign Atopic Dermatitis (SASSAD) (4, 5). The I(S)GA is a physician-assessed outcome that evaluates overall disease severity on a 5- or 6-point scale ranging from clear (0) to severe (4) or very severe (5, 6). It provides a single assessment of disease severity based on visual signs of disease such as erythema, induration/papulation, and oozing/crusting (5, 6). However, it is limited in that it does not distinguish between individual AD signs or account for percentage of treatable body surface area (%BSA) or pruritus, one of the most prominent symptoms of AD (7). The Atopic Dermatitis Severity Index (ADSI) is a composite tool that uses the sum of 5 signs and symptoms of AD, each assessed globally and graded on a 4-point scale from none (0) to severe (3) for a maximum severity score of 15 (3). Unlike the I(S)GA, which uses a single score for a global assessment, the ADSI allows for a more detailed breakdown of the severity of individual signs of AD and includes pruritus, erythema, exudation, excoriation, and lichenification. However, it does not include an assessment of %BSA (3).
AD treatment guidelines primarily recommend topical agents, specifically topical corticosteroids, as first-line therapy, and topical calcineurin inhibitors as second-line options (8–11). Crisaborole ointment, 2%, is a nonsteroidal phosphodiesterase 4 inhibitor for the treatment of mild-to-moderate AD (12). In 2 large, identically designed phase 3 studies (AD-301: ClinicalTrials.gov, NCT02118766; AD-302: ClinicalTrials.gov, NCT02118792), significantly more crisaborole-treated patients with mild-to-moderate AD achieved ISGA success (defined as clear [0] or almost clear [1] with a ≥ 2grade improvement from baseline) than vehicle-treated patients (6). In phase 2 studies, crisaborole was effective in improving ADSI score (13, 14). Although the components of ADSI were assessed in the phase 3 studies, ADSI score was not a prespecified outcome measure. In this post hoc analysis, the efficacy of crisaborole in the pooled phase 3 studies was evaluated using ADSI scores, calculated via the summation of pruritus and signs of AD scores, and by evaluating the effect of crisaborole on %BSA.
Study designs
Study designs and methods have been published previously (6). Two multicenter, randomized, double-blind, vehicle-controlled phase 3 studies were performed to assess the efficacy and safety of crisaborole in patients ≥ 2 years with mild-to-moderate AD per ISGA. Patients were randomly assigned 2:1 to receive crisaborole or vehicle twice daily for 28 days. Both studies were conducted in accordance with Good Clinical Practice Guidelines and local regulatory requirements. The institutional review boards of participating centers approved the study protocols, and all participants provided informed consent.
Assessments
Prespecified efficacy measures included assessment of pruritus and signs of AD, including erythema, exudation, excoriation, and lichenification, each graded on a 4-point scale ranging from none (0) to severe (3). Pruritus was assessed twice daily by the patient or parent/caregiver via electronic diary using the validated Severity of Pruritus Scale (SPS) (15). For SPS, baseline values were based on the average of ≥ 2 assessments on day 1. For all other time points, SPS values were based on weekly average scores. Signs of AD were assessed by the investigator at each study visit. Other prespecified efficacy measures included %BSA, quality of life (QOL, as measured by the Dermatology Life Quality Index [DLQI] for patients ≥ 16 years and the Children’s Dermatology Life Quality Index [CDLQI] for patients 2–15 years (16, 17)), and severity of AD as measured by ISGA (5-point scale ranging from clear [0] to severe [4] (6)). In this analysis, %BSA was categorized according to previously defined severity bands: clear (0%), mild (> 0 to < 16%), moderate (16 to < 40%), and severe (40–100%) (18). These severity bands were chosen from among a number of different possible strata based on the highest κ-coefficient with a 4-point I(S)GA scale (κ = 0.66) (18). Additional detail regarding scoring of these outcomes can be found in Paller et al. (6).
In this post hoc analysis, ADSI scores were calculated for each patient as the sum of the pruritus, erythema, exudation, excoriation, and lichenification scores that were collected prospectively in the phase 3 trials. ADSI scores were categorized according to previously defined (18) severity bands: clear/almost clear (0 to < 2), mild (2 to < 6), moderate (6 to < 9), and severe (9–15) (Fig. 1). These severity bands were chosen from a number of different possible bands based on having the highest κ-coefficient with a 4-point I(S)GA scale (κ = 0.55) (18).
Fig. 1. Atopic Dermatitis Severity Index (ADSI) score calculation and severity bands. aAdditional detail regarding grading of signs/symptoms can be found in Paller AS, et al (6).
Outcomes
Post hoc outcomes included change from baseline in ADSI scores at days 8, 15, 22, and 29; change from baseline in %BSA at day 29; proportion of patients who experienced ADSI improvement from baseline (defined as a change from moderate-severe to mild-clear/almost clear or from mild to clear/almost clear) and %BSA improvement from baseline (defined as a change from moderate-severe to mild-clear or from mild to clear) at day 29; proportion of patients who had an ADSI score of clear/almost clear at day 29 by baseline ADSI (among patients with baseline ADSI >1) and %BSA categories; and proportion of patients who achieved success in ISGA (defined as ISGA of clear [0] or almost clear [1] with ≥2-grade improvement from baseline), and ISGA of clear/almost clear at day 29 by baseline ADSI and %BSA categories. In addition, correlations between ADSI and ISGA, %BSA, DLQI, and CDLQI and between %BSA and ISGA, pruritus, DLQI, and CDLQI at baseline and day 29 were calculated.
Statistical analysis
Data from AD-301 and AD-302 were pooled for this analysis. ADSI scores were summarized using descriptive statistics. Comparisons between treatment groups for changes from baseline in ADSI and %BSA were analyzed using the Wilcoxon signed rank test. Proportions of patients with ADSI of clear/almost clear were compared between groups using normal approximation. Correlations and associated p values were calculated using Spearman rank correlations. Patients with missing data for any of the 5 signs/symptoms at any given time point were considered to have a missing ADSI score for that time point and, therefore, were not included in the efficacy analysis for that time point.
Demographics and baseline disease characteristics
The pooled intention-to-treat population for AD-301 and AD-302 included 1,016 patients treated with crisaborole and 506 treated with vehicle. Demographics and key baseline disease characteristics were balanced across treatment groups (Table I and Fig. 2). All patients had mild or moderate disease according to baseline ISGA; however, based on ADSI and %BSA severity bands, substantial proportions of patients were classified as having moderate or severe disease (Fig. 2). According to the ADSI, approximately 43% of patients had moderate disease and 33–34% had severe disease, whereas 23–28% had moderate disease and 10–12% had severe disease according to %BSA (Fig. 2). When ADSI was deconstructed into its component signs and symptoms, the average score indicated that most signs and symptoms were mild to moderate except for exudation, which was mild, on average.
Table I. Demographics and baseline disease characteristics (pooled AD-301 and AD-302)
Fig. 2. Baseline atopic dermatitis (AD) severity by outcomes measure (pooled AD-301 and AD-302). aSeverity bands for Atopic Dermatitis Severity Index (ADSI): clear/almost clear (0–< 2), mild (2–< 6), moderate (6–< 9), severe (9–15) (18), bSeverity bands for percentage of treatable body surface area (%BSA): clear (0), mild (> 0–< 16), moderate (16–< 40), severe (40–100) (18). ISGA: Investigator’s Static Global Assessment; SD: standard deviation.
Atopic Dermatitis Severity Index
A decrease in ADSI score was observed in both treatment groups over time; a significantly greater reduction in mean ADSI score was observed in the crisaborole group compared with the vehicle group as early as day 8 and at days 15, 22, and 29 (Fig. 3). The proportion of patients who had improvement in ADSI score at day 29 was significantly greater for crisaborole-treated patients than vehicle-treated patients (62.7% vs. 48.4%; p < 0.0001). The proportion of patients with an ADSI score of clear/almost clear at day 29 was greater in the crisaborole-treated group than the vehicle-treated group across baseline disease severity as assessed by ADSI; however, these differences were only significant for base-line severe ADSI (Fig. 4A). Similarly, the proportion of patients with an ADSI score of clear/almost clear at day 29 was greater in the crisaborole-treated group than the vehicle-treated group across the baseline disease severity as assessed by %BSA; however, these differences were only significant for baseline severe %BSA (Fig. 4B). When analyzed by baseline lichenification, mean change from baseline in ADSI score was greater for crisaborole-treated patients than vehicle-treated patients regardless of baseline score, with significant differences observed for all nonzero baseline scores (Fig. 5). When analyzing ISGA outcomes by baseline ADSI severity, significantly more crisaborole-treated patients achieved ISGA clear or almost clear at day 29 than vehicle-treated patients regardless of baseline ADSI severity; however, for ISGA success, differences between crisaborole and vehicle were only observed for patients with severe baseline ADSI score (Fig. 6).
Fig. 3. Mean change in Atopic Dermatitis Severity Index (ADSI) score from baseline over time (pooled AD-301 and AD-302).
Fig. 4. Proportion of patients with Atopic Dermatitis Severity Index (ADSI) score of clear/almost clear at day 29 by baseline ADSIa (A) and baseline percentage of treatable body surface area (%BSA)b (B) (pooled AD-301 and AD-302). aADSI scores were stratified according to following severity bands: clear/almost clear (0–< 2), mild (2–< 6), moderate (6–< 9), and severe (9–15) (18). Analysis was conducted among patients with baseline ADSI > 1. b%BSA was stratified according to the following severity bands: clear (0), mild (> 0–< 16), moderate (16–< 40), and severe (40–100) (18).
Fig. 5. Change from baseline in Atopic Dermatitis Severity Index (ADSI) score at day 29 by baseline lichenification (pooled AD-301 and AD-302).
Fig. 6. Proportion of patients with (A) success in Investigator’s Static Global Assessment (ISGA)a and (B) ISGA clear or almost clear at day 29 by baseline Atopic Dermatitis Severity Index (ADSI) severityb (pooled AD-301 and AD-302). aISGA success was defined as achieving score of clear (0) or almost clear (1) with a 2-grade or more improvement from baseline. bADSI scores were stratified according to following severity bands: clear/almost clear (0–< 2), mild (2–< 6), moderate (6–< 9), and severe (9–15) (18).
Percentage of treatable body surface area
Mean %BSA decreased from 18.3% at baseline to 10.6% at day 29 in crisaborole-treated patients and 18.1% to 13.6% in vehicle-treated patients. Mean change (95% CI) in %BSA at day 29 was significantly greater in crisaborole-treated patients than vehicle-treated patients (–7.43 [–8.22 to –6.64] vs. –4.44 [–5.55 to –3.33]; p < 0.0001). The proportion of patients with %BSA improvement at day 29 was significantly greater in the crisaborole-treated group than the vehicle-treated group (27.6% vs. 19.7%; p < 0.001). When analyzing ISGA outcomes by baseline %BSA severity, significantly more patients with mild or moderate baseline %BSA who were treated with crisaborole than those treated with vehicle achieved success in ISGA at day 29. Similarly, significantly more patients with baseline %BSA severity of mild or moderate treated with crisaborole compared with vehicle achieved ISGA clear or almost clear at day 29 (Fig. 7).
Fig. 7. Proportion of patients with (A) success in Investigator’s Static Global Assessment (ISGA)a and (B) ISGA clear or almost clear at day 29 by baseline percentage of treatable body surface area (%BSA) severityb. aISGA success was defined as achieving score of clear (0) or almost clear (1) with a 2-grade or more improvement from baseline, b%BSA was stratified according to the following severity bands: clear (0), mild (> 0–< 16), moderate (16–< 40), and severe (40–100) (18).
Correlations
ADSI score was significantly correlated with several treat-ment outcomes, such as ISGA, %BSA, SPS, DLQI, and CDLQI at baseline and at day 29 (Table II). Likewise, %BSA was significantly correlated with ISGA, SPS, DLQI, and CDLQI at baseline and day 29 (Table II).
Table II. Spearman rank correlations for Atopic Dermatitis Severity Index (ADSI) and percentage of treatable body surface area (%BSA) with other outcomes
In this post hoc analysis of pooled data from AD-301 and AD-302, crisaborole showed improvement in disease based on ADSI and %BSA. With use of crisaborole, greater decreases from baseline were seen in mean ADSI score and mean %BSA at day 29 compared with vehicle, and greater proportions of patients treated with crisaborole experienced improvement in ADSI score and %BSA. Change from baseline in ADSI score was greater for crisaborole-treated patients than vehicle-treated patients, even with increasing levels of lichenification at baseline. Lichenification is often resistant to treatment (19) because it may contribute to poorer dermal penetration of topically applied drugs; however, in this analysis, crisaborole-treated patients with severe lichenification had the greatest improvement in ADSI score, whereas in those with no lichenification, no significant difference was observed. These results may also be influenced by lower ADSI overall scores at baseline for patients with no lichenification and/or small sample sizes. Nevertheless, the efficacy of crisaborole in patients with lichenification warrants further prospective study.
Many constructs are used to measure AD severity, such as SCORAD, EASI, I(S)GA, and SASSAD (4, 5). The Harmonising Outcomes in Eczema (HOME) Initiative recommends EASI followed by SCORAD as the pre-ferred assessments of AD signs in clinical trials (20). However, the US Food and Drug Administration requires I(S)GA as the primary endpoint in clinical trials of treatments for AD (21); therefore, it was used in the primary analyses for AD-301 and AD-302. However, I(S)GA omits 2 of the most important aspects of the disease – pruritus and extent of disease (i.e., %BSA). The EASI includes a component that addresses %BSA but not pruritus. Although the ADSI does not include extent of disease, it includes an assessment of pruritus, is relatively simple to calculate, and correlated well with ISGA and %BSA in this analysis. Thus, in the absence of the EASI, the ADSI can be used to assess AD severity. AD-301 and AD-302 included patients with mild-to-moderate AD per ISGA assessment alone. However, our analysis showed that many patients could be classified as having more severe disease per the ADSI and/or %BSA, based on recently established severity bands (18). Because of the bands determined for the ADSI, a patient with moderate severity (score=2) in all 5 components of the ADSI would be considered to have an ADSI score of severe. This characteristic is similar to that seen with the EASI and SCORAD, where a patient with widespread or extensive disease may be classified as having severe disease even if individual symptoms are moderate. Despite the inclusion of patients with more severe disease per the ADSI or %BSA, the use of crisaborole triggered significant improvement in ADSI score and %BSA compared with vehicle at day 29. Similarly, a greater proportion of patients who received crisaborole experienced improvement in these measures than those who received vehicle, regardless of baseline disease severity measured by the ADSI or %BSA. Only crisaborole-treated patients with severe baseline ADSI scores had a significantly higher rate of achievement of ISGA success at day 29 than vehicle-treated patients, but not those with mild or moderate baseline ADSI score, whereas patients with mild or moderate baseline %BSA had higher rates of ISGA success with crisaborole, but not those with severe baseline %BSA. Possible explanations for these results could be the small sample sizes or challenges in adequately treating extensive disease with a topical medication, particularly for those with severe baseline %BSA. Considering the ≥ 2-grade improvement from baseline criteria included in the definition of ISGA success, it is more difficult for patients with mild disease (per ISGA) to achieve this endpoint than it is for those with moderate disease. This may translate to patients with mild or moderate ADSI scores at baseline also having more difficulty achieving ISGA success.
Use of crisaborole has previously shown improvement per the ADSI in other phase 2 trials (13, 14). In one of these, patients with AD lesions and ADSI scores ranging from 6 to 12 (moderate to severe with new ADSI severity banding) experienced a 71% improvement from baseline after 29 days of treatment with crisaborole twice daily (13). Between those phase 2 studies, mean ADSI score with crisaborole was 8.2 at baseline and 2.4 at day 29 in one study (13) and 8.3 at baseline and 2.4 at day 28 in the other (14). Similarly, in this post hoc analysis of the AD-301 and AD-302 studies, mean ADSI score was 7.4 at baseline and 3.9 at day 29. However, these ADSI results from the phase 2 studies were for a target lesion rather than the whole-body assessment, as used in this analysis.
As with any post hoc analysis, these results are limited by not being powered a priori to detect a significant difference in ADSI scores between treatments. In addition, the ADSI has not been validated; however, pruritus was assessed using a validated measure (15).
This post hoc analysis confirms the effectiveness of crisaborole in alleviating AD severity as assessed by both the ADSI and %BSA and allows the results to be put into context of the previous phase 2 trials. This analysis also supports the use of the ADSI to measure AD severity, although further psychometric evaluation is necessary.
Medical writing support under the guidance of the authors was provided by Robert J. Schoen, PharmD, and Jennifer C. Jaworski, MS, at ApotheCom, San Francisco, CA, USA, and was funded by Pfizer Inc., New York, NY, USA, in accordance with Good Publication Practice (GPP3) guidelines (Ann Intern Med 2015;163:461–4).
Funding sources: This study was supported by Pfizer Inc.
Conflicts of interest: JIS served as a consultant and/or advisory board member for and received honoraria from AbbVie, AnaptysBio, Asana, Arena, Boehringer-Ingelheim, Dermavant, Eli Lilly, Galderma, GlaxoSmithKline, Glenmark, Kiniksa, LEO, Menlo, Novartis, Pfizer, Regeneron-Sanofi, and Realm; served as a speaker for Regeneron-Sanofi; and received research grants from GlaxoSmithKline. WCP, HT, RAG, and MAZ are employees and stockholders of Pfizer Inc. AMT is a former employee and stockholder of Pfizer Inc.
Data sharing statement: Upon request, and subject to certain criteria, conditions and exceptions (see https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information), Pfizer will provide access to individual de-identified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines and medical devices (1) for indications that have been approved in the US and/or EU or (2) in programs that have been terminated (i.e., development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The de-identified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.


 Click to show fullsize
Click to show fullsize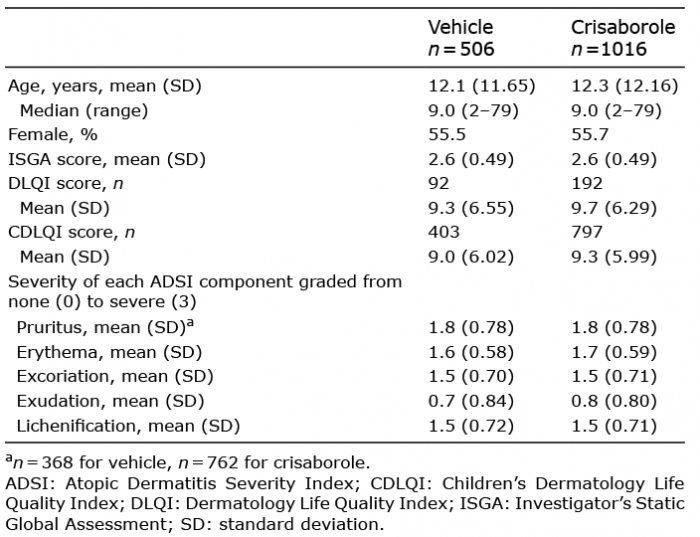 Click to show fullsize
Click to show fullsize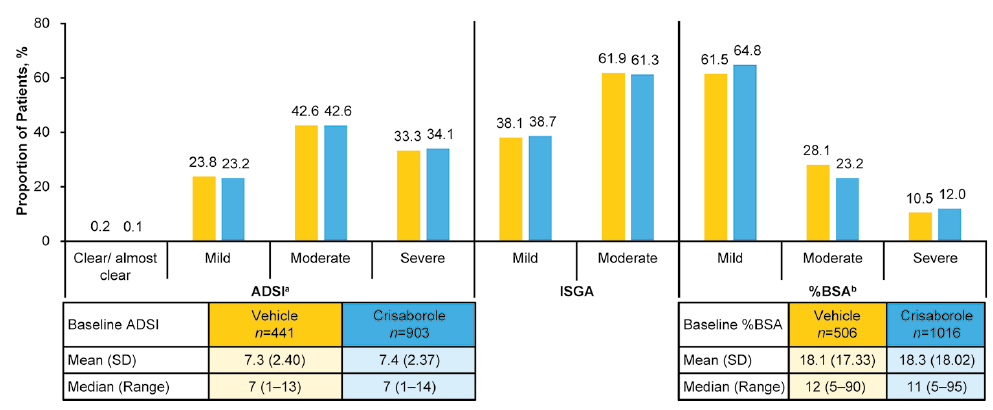 Click to show fullsize
Click to show fullsize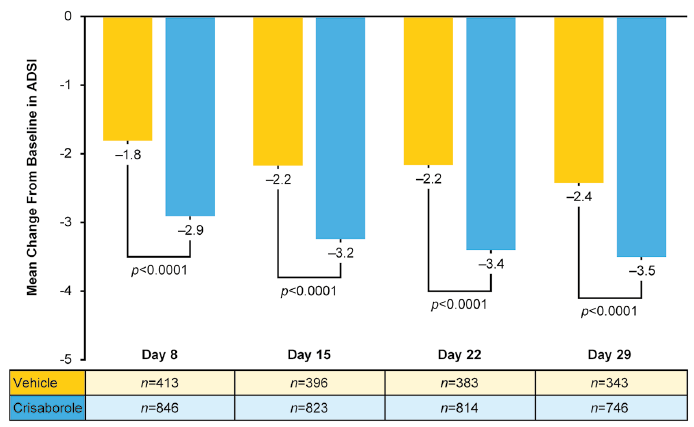 Click to show fullsize
Click to show fullsize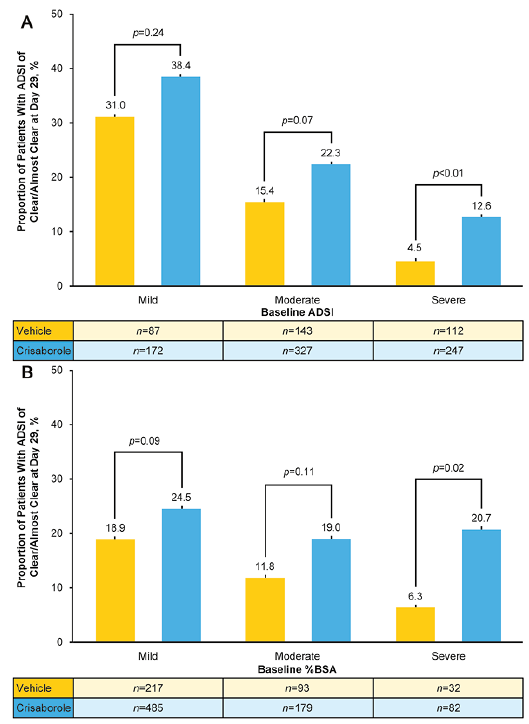 Click to show fullsize
Click to show fullsize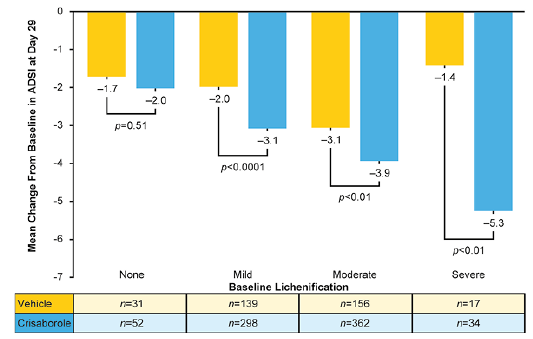 Click to show fullsize
Click to show fullsize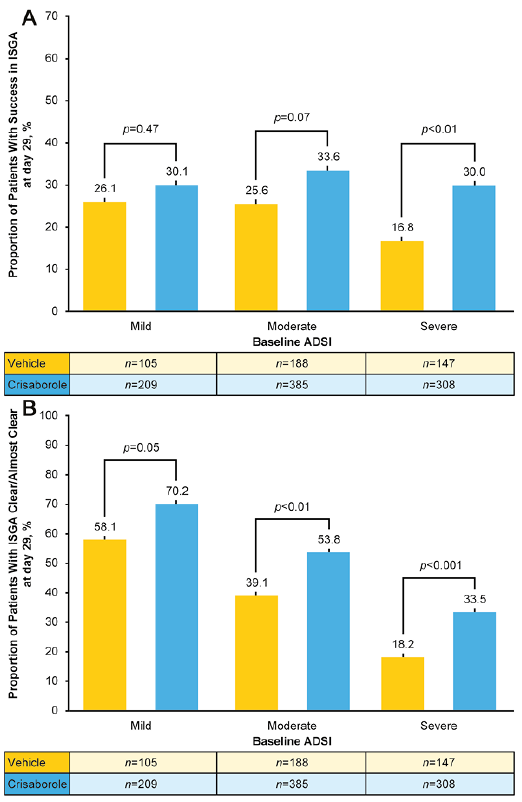 Click to show fullsize
Click to show fullsize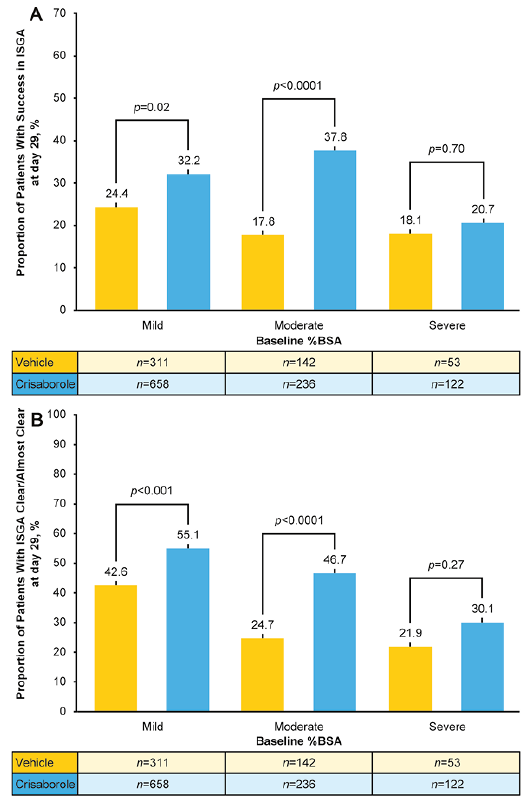 Click to show fullsize
Click to show fullsize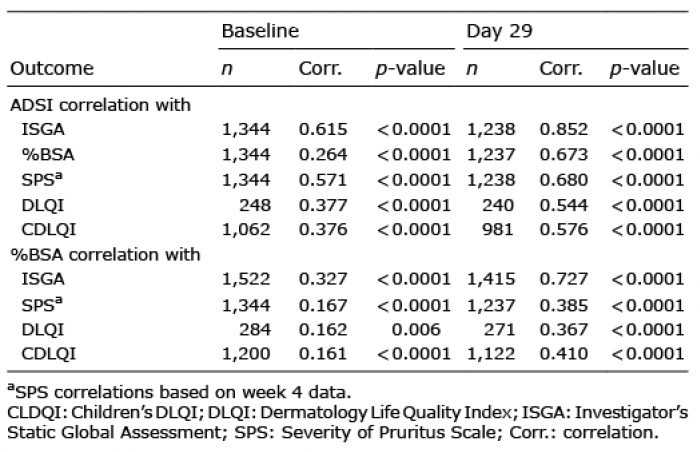 Click to show fullsize
Click to show fullsize