


Centre of Evidence-Based Dermatology, University of Nottingham, Nottingham, UK
Despite advances in atopic dermatitis (AD) treatments, research into AD prevention has been slow. Systematic reviews of prevention strategies promoting exclusive and prolonged breastfeeding, or interventions that reduce ingested or airborne allergens during pregnancy and after birth have generally not shown convincing benefit. Maternal/infant supplements such as Vitamin D have also not shown any benefit with the possible exception of omega-3 fatty acids. Systematic reviews suggest that probiotics could reduce AD incidence by around 20%, although the studies are quite variable and might benefit from individual patient data meta-analysis. Skin barrier enhancement from birth to prevent AD and food allergy has received recent interest, and results from national trials are awaited. It is possible that trying to influence major immunological changes that characterise AD at birth through infant-directed interventions may be too late, and more attention might be directed at fetal programming in utero.
Key words: atopic dermatitis; atopic eczema; eczema; prevention.
Accepted May 7, 2020; Epub ahead of print May 15, 2020
Acta Derm Venereol 2020; 100: adv00166.
Corr: Prof. Hywel C. Williams, Nottingham University Hopsitals NHS Trust Queen’s Medical Centre Campus, Nottingham, NG7 2UK, UK. E-mail: Hywel.williams@nottingham.ac.uk
Just like we can prevent infectious diseases like polio, it should be possible to prevent eczema (atopic dermatitis), food allergy and asthma. Most things that have been tried so far to prevent eczema including exclusive breastfeeding, timing of starting solids, supplements like Vitamin D and reducing house dust mite do not seem to work. Taking probiotics (friendly gut bacteria) during pregnancy probably reduces the risk of eczema by around 20%, although we are still not sure what combination is best. New research is trying to find out if special creams that make a baby’s skin barrier stronger can prevent eczema.
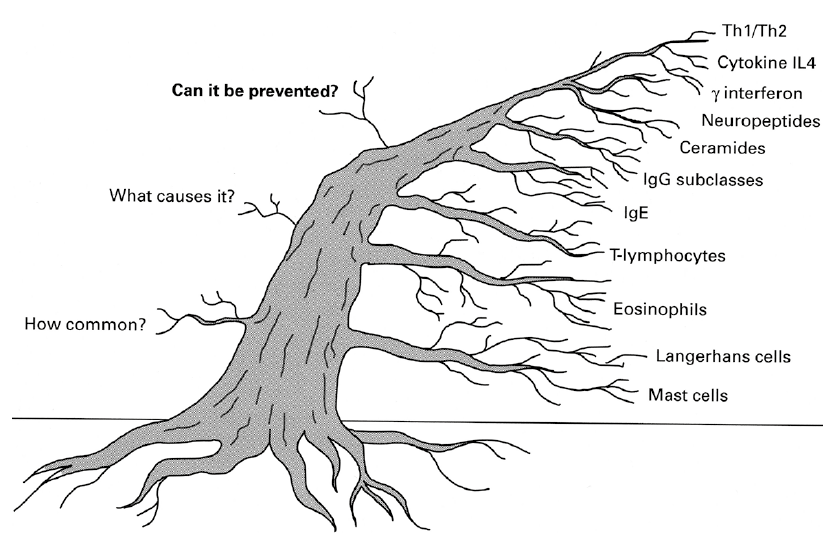
Despite the familiar adage that “prevention is better than cure”, prevention of atopic dermatitis (AD) has been a relatively neglected topic of research until recently. A PubMed search (using the terms [atopic dermatitis OR eczema] AND treatment (August 14th 2019) revealed 19,755 hits, compared with just 3,150 when disease terms were combined with “prevention”. Reasons for lack of research could include a lack of interest in population-based research in favour of basic science (Fig. 1), lack of research skill capacity in prevention research, lack of funding and a limited choice of identifiable risk factors that are amenable to public health manipulation. However, the number of AD prevention studies has increased over the last 10 years, especially in the field of probiotics and interventions to enhance the skin barrier. Basic science discoveries into the human microbiome and genetics of AD may have played a part in contributing to this recent trend (1, 2). Whilst identifying risk factors that can be manipulated is an essential part of prevention research, understanding the mechanisms by which the effects of prevention are mediated is interesting but not essential. For example, the benefits of stopping smoking to prevent lung cancer became apparent from simple epidemiological research long before the mechanisms and precise carcinogens were discovered (3). Prevention of disease is arguably a much more logical and cost-effective way to manage the burden of a disease such as AD than focussing solely on drug treatment of sick individuals who seek medical help after a long chain of irreversible pathological events (Fig. 2). Whilst some drugs such as penicillin for streptococcal infection can be curative, most only modify rather than cure chronic diseases like AD, they are often expensive, and all are associated with potential adverse effects.
Fig. 1. A skewed interest toward cellular and molecular atopic dermatitis (AD) mechanisms relative to research into AD populations. Research into AD over the last 50 years has been dominated by interest in cells rather than broader questions such as whether disease prevention is possible.
Fig. 2. Where is intervention most effective? Although the concept of prevention of atopic dermatitis is rarely discussed at international meetings, an upstream approach is a far more logical approach to reduce the burden of disease at a population level than the current approach of treating sick individuals with expensive drugs who present to secondary care after a long chain of pathological events.
This article attempts to critically review the current state of science on the prevention of atopic dermatitis. Throughout this article, we will refer to the disease of interest as AD, which is synonymous with atopic eczema or just “eczema” (4). We use the term atopic dermatitis to describe the clinical phenotype, rather than the scientific definition of clinical phenotype plus evidence of IgE sensitisation to environmental allergens. We start by introducing the reader to key considerations when designing or critically appraising studies of AD prevention, using our direct experience in designing and running a randomised controlled trial (RCT) of emollients to prevent AD. We then explore the main interventions that have been used to try and prevent AD such as maternal and infant dietary restrictions or supplements, aeroallergen avoidance and approaches designed to enhance the external skin barrier. The authors have chosen to use systematic reviews of evidence and RCTs as the evidence source where possible. Systematic reviews were harvested from the Centre of Evidence-Based Dermatology international collection of systematic reviews which is updated monthly by a senior information scientist (Dr. Douglas Grindlay) (5). Rather than summarise all 102 systematic reviews on AD prevention in this collection, we instead refer to overviews of systematic reviews or the most recent and comprehensive systematic reviews where possible (6, 7). We used the Global Resource for Eczema Trials (GREAT) database for RCTs that might not yet be included in systematic reviews (8).
The power of prevention
Because prevention strategies act at a population level, their power is often not appreciated by individuals compared with treatments for a disease. Yet the power of prevention is potentially huge. In his article entitled “The power of prevention and what it requires” Woolf draws our attention to the fact that whereas new diabetes drugs that reduce glycohemoglobin levels by 0.5% often make the headlines, exercise, that can lower the incidence of diabetes by 50%, rarely achieves such publicity (9). The conquest of many infectious diseases such as diphtheria, smallpox, polio and measles are testament to the power of prevention, yet individuals who would have contracted these diseases are seldom “grateful” to those developing and implementing vaccines as it is unclear who would have contracted the disease in the first place. The recent re-emergence of measles due to misguided beliefs about vaccine safety, termed “vaccine hesitancy”, are timely reminders of the “invisible” and powerful effects of population-based interventions (10).
Primary, secondary and tertiary prevention
Primary prevention typically refers to intervening before health effects occur. Secondary prevention implies detecting a disease at an early stage to prevent worsening, whereas tertiary prevention is the reduction of symptoms or improvement in quality of life of those with established disease – i.e. where health care professionals normally operate (11).
Application of the Participant, Intervention, Comparator and Outcomes framework to atopic dermatitis prevention studies
Participant, Intervention, Comparator and Outcomes (PICO) is a framework used in evidence-based medicine to understand the structure of RCTs and is useful when considering the design and critical appraisal of AD prevention trials (12).
Participants. Most AD prevention studies target a high-risk population e.g. babies born to families with a first-degree relative with AD or associated allergic diseases such as asthma, hay-fever or food allergy. The advantage of this approach is that parents who have experienced AD themselves or witnessed it in family members are often highly motivated (during pregnancy or soon after) to undertake interventions that could prevent AD in their new baby. The disadvantage is that if the selected population is too narrow, the intervention may have a limited overall population impact. However, tackling an entire population such as all newborns is challenging, especially if the behaviour change modification is substantial, as parents will be less motivated to act on something that will be of little perceived benefit to their child. This phenomenon is known as the prevention paradox – a term coined by Rose to denote “a measure that brings large benefits to the community offers little to each participating individual” (13). Fig. 3 illustrates the possible trade-off between high and low risk approaches to AD prevention suggested previously (14).
Fig. 3. Hypothetical example of the prevention yield from a high risk vs low risk prevention approach for atopic dermatitis. Depicts an average Western population where 40% of 1,000 adult couples have a strong family history of atopy and 60% do not. If 30% of the high risk babies develop AD compared with 15% without such a family history, a high risk approach would only prevent 57% (120/120+90) of AD cases at a population level. Adapted from Williams HC. Atopic Dermatitis. In: Williams HC, Strachan DP (eds). The Challenge of Dermato-Epidemiology. Boca Raton, CRC Press Inc., 1997.
Intervention. An essential step in the prevention of any disease is a thorough knowledge of risk factors that can be manipulated. For example, filaggrin gene mutations cannot be directly manipulated in utero at present (although it may be possible in time) whilst a reduction in house dust mite in the home environment is achievable. Another key consideration is the acceptability of interventions given that healthy people are being asked to undergo elaborate changes to their lives in order to prevent disease in a proportion of people – the identity whom will remain unknown to them. Here, there is often a trade-off between intensity of intervention which might achieve a larger effect (such as applying emollient twice a day to their child for 2 years, wash only in soft water and use no soap) versus those that are likely to have wider population reach (such as advice to use emollients once daily for the first year of life as in the BEEP trial) (15). Testing acceptability of interventions is essential before proceeding to full scale evaluation (16). Assessing safety is paramount in prevention studies. Whilst individuals with severe AD might accept the risk of nausea and liver disease from methotrexate therapy, healthy individuals will have a low threshold for rejecting interventions with even small risks, such as the slipping on emollients spilt on a bathroom floor. Furthermore, minor adverse effects such as transient stinging after emollient application can reduce adherence to an intervention.
Comparator. In the absence of a clear reference standard of an effective active treatment, control interventions for AD prevention trials are typically “standard care” (which is often not defined), an attention control, or some form of placebo (e.g. inactive probiotics). Convincing parents with a family history of AD to take part in a study with a 50:50 chance that their new baby will be allocated to the “no treatment” group can be challenging, and unless equipoise is carefully explained, parents may drop out if they don’t get the “new active” intervention. Feasibility studies that test randomisation and retention are essential and offer the opportunity to develop patient information materials with patients that imply active monitoring and altruistic rewards to overcome the notion of “control neglect” that can result in resentful demoralisation (17).
Outcomes. Whereas clinical trials of people with AD (prevalent cases) seek to reduce disease severity, one is trying to prevent new (incident) cases from developing in a prevention study. There is a lack of research on defining an incident case of AD. Simpson et al. (18) undertook a systematic review of definitions of an incident case of AD used in prevention studies. Of 102 included studies, 27 did not define an incident case, 28 used the Hanifin & Rajka criteria (19), and 21 used definitions unique to that study without referencing the source. It is important to note that “chronic relapsing course” (a major criterion for the Hanifin & Rajka criteria), whilst acceptable for measuring cumulative incidence, is problematic when defining a new case which, by definition, has not yet become chronic. Yet diagnosing AD confidently in a baby on the first day they develop an eczematous rash is also fraught with problems as transient irritant eczematous dermatoses (which are probably not true AD) are common in infancy. Simpson et al. (20) suggested a compromise whereby the UK refinement of the Hanifin & Rajka criteria are used to denote a continuous or intermittent itchy skin condition lasting at least 4 weeks.
Ideally outcome assessment should be separated from the intervention period by a clear margin to separate treatment effects from prevention effects. For example, in the two small preliminary studies that suggested emollients might prevent AD, outcomes were assessed at the end of the intervention period, making it difficult to assess whether the apparent benefit was due to emollients preventing AD or actively treating new mild AD (16, 21). This is why the main BEEP trial of emollients used during the first year is assessing the primary outcome of AD (those fulfilling the UK refinement of the Hanifin & Rajka criteria in the last year) at the age of 2 years (15). Whilst complete prevention of disease is the ultimate goal, prevention of more severe forms of the disease (which cause the most morbidity and result in most healthcare usage) is also an important goal in AD prevention trials. Because the shape of AD prevalence in any population is skewed to the left (Fig. 4), even small shifts in the reduction of population severity can result in large gains in absolute terms for the number switching from severe to moderate or mild to very mild/subclinical disease. Time to onset of AD is another outcome that can be considered although it is debatable whether simply delaying onset of a miserable disease to an older age is really a bonus. Given that AD is closely related to other “atopic” diseases such as food allergy, asthma and hay fever, AD prevention studies also need to evaluate whether benefits are seen in these diseases too. Measuring other atopic diseases present their own challenges, e.g. true food allergy has a low incidence making it unlikely that beneficial effects will be precisely measured even in large studies, and conditions like asthma have a later age of onset adding to the cost of following up individuals from RCTs that start at birth to older ages.
Reducing bias. In addition to standard approaches to reduce RCT biases such as registration of study protocols before recruitment starts and ensuring randomisation is truly random and concealed, two biases require special consideration in AD prevention trials. The first is performance bias which results from treating intervention and control groups differently. More attention given to the intervention group can result in different ancillary behaviours that can affect AD risk, so it is important that both groups are treated in the same way in terms of regularity of contact and incentives from the research team, and any post-randomisation behaviours that could confound the study result are recorded. Sometimes such behaviours can include contamination of the intervention in the control group (because they think they are missing out on something beneficial), which can be a particular problem if the intervention is something that can be easily accessed by participants without the need for healthcare professionals, such as reduction of house dust mites in the home. Contamination should therefore be measured and explored in the analysis. A second challenge lies in the fact that because many interventions such as emollient application or installing a water softener cannot be blinded, it is essential to include some form of objective outcome assessment (e.g. visible eczema recorded by investigators blinded to intervention status) to mitigate the risk of information bias. Studies should present findings as absolute risk reductions as well as the more impressive sounding relative risk reductions in order to provide a more realistic indicator of population benefit.
Fig. 4. Schematic representation of atopic dermatitis severity (x-axis) versus number with atopic dermatitis in two hypothesized populations. Even if atopic dermatitis cannot be prevented completely, shifting the population severity distribution of disease to the left (red curve) could have a huge impact on pushing more into subclinical disease and reducing the absolute proportion with severe disease who suffer the most and who consume most health resources.
Primary prevention
The 2011 overview of systematic reviews of primary prevention. In an attempt to reconcile the increasing number of Cochrane and non-Cochrane systematic reviews on AD prevention, a group (including the two authors) undertook an overview of all such systematic reviews in 2011 (search date up to August 2010). Quantitative and qualitative methods were used to collate and combine data where possible using Cochrane methods. Included reviews had to include some quantitative data that could be combined, search date within the last 5 years, and included participants between the ages of zero and 18 years. Seven systematic reviews containing 39 RCTs and 11,897 participants met the inclusion criteria. All 7 reviews were considered methodologically sound, although the data from the review on probiotics had to be re-analysed as data from one trial had been included more than once in the same meta-analysis. Interventions included use of hydrolysed formula milk (extensive and partial), extended duration of exclusive breastfeeding, dietary supplementation with omega-3 and omega-6 oils, maternal dietary antigen avoidance during pregnancy, lactation or both, soy formula milks, along with prebiotics and probiotics. Participants were from a mixture of high and lower risk families, although risk was rarely adequately defined. None of the pooled interventions showed clear evidence of benefit for AD prevention. A subgroup analysis of those at high risk of developing AD based on just one RCT found that prebiotics (ingested substances that favour the growth of beneficial bacteria in the gut) decreased AD incidence by 58% (RR: 0.42; 95% CI: 0.21, 0.84) compared with no prebiotics. Data on whether those developing AD were truly atopic was missing from most of the studies, and in those that did, there was no evidence that the interventions decreased atopy. One non-randomised study suggested that prolonged exclusive breastfeeding (at least 6 months) reduced AD incidence by 60% (RR 0.40, 95% CI 0.21 to 0.78). Despite the lack of any convincing signals for any of the interventions tested, the risk estimates for most interventions had low precision, indicating that some interventions with no evidence of benefit could still be useful.
The post 2011 overview era
Interventions that are ingested by mothers and/or infants. Also known as the “inside out” approach, ingested maternal/infant interventions include exclusive breastfeeding, delay or early introduction of foods other than milk, dietary restrictions, and dietary supplements. Although breastfeeding (exclusive or prolonged) has clear benefits for infants, a systematic review of 16 moderate quality observational studies suggests that it does not appear to be protective of AD (22). One large cluster RCT (the PROBIT trial in Belarus) that promoted breastfeeding found a reduction in self-reported flexural eczema but not lung function, a finding that needs to be replicated (23). Around a half of milk feeding studies have been judged to be at high risk of bias (24). A Cochrane review of 5 trials failed to show any benefit of maternal avoidance of allergenic foods for AD prevention (25). A 2019 systematic review of mainly observational studies of complementary feeding (whereby other foods and drinks complement human or formula milk) found no clear evidence between the age at which complementary feedings is started and the risk of AD, food allergy or asthma (moderate evidence) (26). The same review found limited to strong evidence that introducing allergenic foods in year one of life to try and induce tolerance does not increase AD or food allergy risk, but may prevent egg and peanut allergy. The one well-conducted RCT included in the review found no benefit for AD prevention from early introduction of allergenic foods (27).
Interest in vitamin D supplementation as a possible preventative intervention stems from the association between low vitamin D levels and increased incidence and severity of AD. Vitamin D is also known to have a regulatory influence on skin barrier function and the immune system and skin barrier function, both of which are involved in AD development (28). A 2017 systematic review (search date January 2016) found one RCT and 3 non-RCTs that addressed vitamin D supplementation in women and children as a means of preventing allergic diseases found no clear evidence of benefit but with low certainty of evidence (29). A more recent and well conducted RCT found no clear benefit of infant vitamin D supplementation in the primary prevention of AD (30). A systematic review of omega-3 long-chain polyunsaturated fatty acids (such as from fish) intake during pregnancy found mixed results for AD prevention from observational studies, but a possible protective effect in the 3 included RCTs for early onset AD (31).
The evidence that ingested probiotics (non-pathogenic live bacteria or yeasts that can restore a dysfunctional pro-inflammatory gut microbiome) or prebiotics (non-digestible food ingredients that encourage beneficial bacteria to thrive) or both (synbiotics) can prevent AD is gathering momentum (32). The field is complicated as probiotics and prebiotics refer to a very wide range of ingredients, and they can be given to the mother during pregnancy, during lactation, to the infant after birth and various combinations of these and for different periods, leading to considerable heterogeneity which impacts on the ability to combine studies. One systematic review exploring the possible health benefits of yoghurt consumption among infants and toddlers that included two older cohort studies suggested a possible benefit for AD prevention, and called for new studies that evaluated such foods in a more contemporary setting (33). A systematic review in 2019 of 22 pooled trials published between January 2008 and May 2018 showed a reduction in AD incidence (RR 0.81, 95% CI: 0.70–0.93) for those receiving probiotic supplementation during pregnancy and/or infancy. Subgroup analysis suggested that benefits were strongest for those receiving Lactobacillus and Bifidobacterium, for those in whom probiotic supplementation occurred during pregnancy and infancy and in preventing AD developing in the first two years of life rather than later (34). Sources of study heterogeneity was also assessed and found to be mainly accounted by follow-up time (I2 62.7%) and length of probiotic supplementation (I2 53.5%). A more extensive systematic review that pooled 28 studies (27 good quality RCTs and one high quality cohort study, search date from inception to March 2018) showed a beneficial effect on AD prevention for probiotics compared with controls (OR 0.69; 95% CI 0.58–0.82, Fig. 5) (35). Analysis of studies whereby probiotics were provided only prenatally or postnatally did not show such benefit, prompting the authors to conclude that benefits are only realised when probiotics are started during pregnancy and continued in the infant for the first 6 months of life. A broader and high-quality systematic review of diet during pregnancy and infancy arrived at similar conclusions regarding a protective effect of probiotics on AD development from 19 probiotic trials (risk ratio 0.78; 95% CI 0.68–0.90; I2 61% and an absolute risk reduction of 44 cases per 1,000; 95% CI 20–64) (24). Subgroup analysis suggested that it was maternal rather than infant probiotic supplementation that was important for realising a protective benefit. The evidence of prebiotics alone was weak due to high risk of bias, inconsistency, imprecision, and indirectness of study results.
Fig. 5. The preventive effect of probiotics in atopic dermatitis. Forest plot depicting a meta-analysis that used a random effects model combining 28 evaluated studies. Although the summary odds ratio (OR) suggests clear benefit (OR 0.69; 95% confidence interval (CI) 0.58–0.82; p < 0.0001), there was considerable heterogeneity between the studies (I2 = 53.6%) (33). Reproduced with kind permission from the American Journal of Clinical Dermatology.
Although the World Allergy Organisation guideline panel has determined that there is a net benefit of probiotics for AD prevention, concerns regarding the heterogeneity of studies remains (36). A comprehensive review of probiotics across all human diseases concluded that the evidence for benefit in allergic diseases was still uncertain and a stimulus for further studies rather than firm clinical recommendations (37). A high-quality individual patient data (IPD) meta-analysis – a type of systematic review that gathers and combines data belonging to individual patient who take part in clinical trials rather than aggregate data – would better identify who benefits most from probiotics, when and why (38).
Interventions directed at the external skin surface. The main “outside in” approaches for preventing AD, sensitisation and food allergy have included attempts to reduce airborne allergens such as house dust mite at the time of birth, increasing exposure to an anthroposophic environment and measures to enhance the skin barrier. A systematic review of house dust mite avoidance strategies (alone or with allergen avoidance) that included 7 RCTs (search date October 2014) concluded such modalities do not decrease the risk of developing AD. Studies that have found strong associations between early exposures to anthroposophic environments such as farm animals have been limited to observational studies so far, but are a fruitful source of ideas for new possible primary interventions (39). Since the discovery of a strong association between AD and loss-of-function mutations in FLG, the gene encoding filaggrin – an essential protein for healthy skin barrier function, interest has increased on the potential benefits of skin barrier enhancement as a means of preventing AD and food allergy (40). Impaired skin barrier may precede eczema development and may be the route by which sensitisation to food allergens occurs (41, 42). Stimulated by the results of two small pilot RCTs that suggested a large benefit from using emollients on the skin of infants born to families with atopy, two large prevention RCTs have been set up to test the hypothesis that emollients from birth can prevent AD (15, 16, 21, 43). The first of these studies (Barrier Enhancement for Eczema Prevention (BEEP) trial) is investigating daily emollient for the first year of life in babies born to atopic families. The second, the Preventing Atopic Dermatitis and Allergies in children study (PreventADALL), is a factorial trial – a trial whereby two or more interventions are carried out and assessed simultaneously. The PreventADALL trial compares (i) no intervention with (ii) skin care (oil-bath at least 5 days/week to age 9 months) and (iii) consecutive introduction of allergenic foods (peanut, milk, wheat, and egg) between 3 and 4 months of age and (iv) both skin and complementary feeding strategies. Results of BEEP and PreventADALL are not available at the time of writing. Two trials were published in 2019, both of which used complex emollients containing ingredients such as ceramide designed to enhance the skin barrier (44, 45). The first study suggested that emollient therapy may reduce AD incidence, but this was not statistically significant, and there was no effect of emollient on barrier measurements (46). The second larger study was a factorial trial of emollient and synbiotics and found no evidence of a protective effect of either intervention (44). At least 10 other similar prevention trials that explore the potential of different skin barrier products to prevent AD in high and low risk populations (46). Together, most of these studies now form part of a prospectively-planned meta-analysis consortium called SCiPAD (Skin care intervention for prevention of atopic disease) (47, 48). Other direct to skin approaches such as “probiotic creams” that serve to influence the early skin microbiome towards one that is less favourable for the development of AD are also worthy of further research (49).
Combined approaches. Whilst it might be easier to implement one simple intervention to prevent AD, it might be possible to combine multiple interventions each of which has a small beneficial effect, especially if they interact to produce more than the sum of the whole. The hazard of a “throw in everything that might work” strategy is that they can become black boxes that are not amenable to replication, unless the components are separated using designs such as factorial trials as currently being done in the PreventADALL study (50).
Secondary prevention
Treating AD more aggressively when it first appears in an attempt to alter the subsequent course of disease in terms of remission or decreasing severity is an attractive notion. One such study of aggressive early treatment is underway in Japan, in which 650 infants who develop AD between the ages of 7–13 weeks old will be randomly assigned to enhanced topical anti-inflammatory treatment or conventional treatment with the aim of preventing food allergy and reducing AD severity (51). Poorly controlled disease resulting in skin damage from scratching can lead to a cascade that results in individuals developing autoimmunity towards their own skin components, a phenomenon that might be key to driving disease chronicity (52). Other non-pharmacological approaches such as behavioural methods to limit skin damage from scratching when AD first appears are also worth considering in this context (53). Like primary prevention, secondary prevention should not be taken lightly, especially with regards to safety. If for example, only 10% of those given early aggressive treatment with prolonged topical corticosteroids benefit from such therapy,
then 90% arguably undergo “overtreatment” and incur side effects in order to benefit the few.
So far, prevention of related diseases such as food allergy and asthma have only been considered in the context of early interventions that primarily aim to prevent AD, but another important question to consider in relation to secondary prevention of AD is whether interventions that are initiated when AD is first identified can prevent the development of conditions such as asthma. Such a concept was the basis of the Early Treatment of the Atopic Child study (ETAC) whereby 795 children with new onset AD between 1 and 2 years of age were randomised to cetirizine or placebo for 18 months. Cetirizine was chosen because it might inhibit eosinophil tracking to the lungs as well as its anti-histamine effect. The ETAC study did not show that asthma could be prevented by such an approach (54). Although urticaria rates were less in the intervention group, severity of AD was not reduced in the cetirizine group either, throwing doubt on the value of anti-histamines in the treatment of AD – an observation that has been confirmed in a subsequent Cochrane review (55, 56). A follow-up RCT from ETAC called the EPAAC study explored the use of levocetirizine for the prevention of asthma in children with AD who were sensitised to grass and/or house dust mite was stopped due to lack of benefit (57).
Tertiary prevention
In its broadest sense tertiary prevention refers to disease treatment, prevention of deterioration, disease complications and sequelae. In relation to AD, one of the most important advances in disease treatment over the last 30 years has been the concept of proactive treatment (two consecutive days per week) for those who have been stabilised. This has been shown to dramatically reduce the number of subsequent flares (58). A meta-analysis by Schmitt et al. showed that topical fluticasone reduced the risk of further flares by around half (relative risk 0.46, 95% CI 0.38–0.55) with more modest reductions in flares with weekly topical tacrolimus (RR 0.78, 95% CI 0.60–1.00) (59). When considering prevention of flares, it is equally important to consider induction of remission before proactive therapy is initiated – the concept of “get control then keep control” as illustrated schematically in Fig. 6 (60). Another review suggested that Vitamin D supplementation for early disease may have a small beneficial effect in reducing later disease severity (61). Given that AD is a chronic relapsing condition, prevention of flares and embracing the concept of overall disease control have become key considerations in improving quality of life of AD sufferers (62). Better prediction of flares in what often appears a random process offers exciting prospects for personalised medicine.
What about adult-onset atopic dermatitis?
Most of the evidence discussed relates to early life. This is with good reason as AD typically starts in the first few years of life. Recent studies have drawn attention to the importance of AD in adults, pointing out that around one in 4 of those with adult AD appear to develop it for the first time in adulthood (63). Less is known about the risk factors for adult-onset AD in order to identify candidates for prevention studies (64). One study of 67,643 US women postulated that niacin intake might protect against adult AD since niacin has been found to decrease transepidermal water loss. Instead, it found that adult AD was paradoxically increased with niacin intake, a finding that needs to be replicated (65).
Fig. 6. The concept of getting control then keeping control in atopic dermatitis. A more subtle interpretation of tertiary prevention is the principle of inducing remission of atopic dermatitis with an initial blast of topical treatment followed by prevention of disease flares with weekly pulses of two consecutive days of topical treatment (also known as the Centre of Evidence-Based Dermatology “get control and keep control” approach). When contrasted against more traditional reactive approaches, the proactive approach results in more disease being pushed into a subclinical state and hence better overall disease control. Reproduced with kind permission from the Journal of Allergy and Clinical Immunology.
The last few decades of research into the prevention of AD have thrown up very few signals of simple, safe interventions that are likely to be effective at a population level. Errors in the design and reporting of studies tend to be repeated rather than learned, and the same old interventions are often tested again and again with little new insight. Past research has also been concerned with a rather fruitless obsession with allergic factors despite the fact that around half of people with “atopic” dermatitis are not atopic in the scientific sense (66). The main exception to the lack of positive findings for AD prevention has been the use of probiotics. Probiotic use has consistently shown modest benefit and good safety when tested in different populations around the world, prompting the World Allergy Organisation guideline panel to determine that there is a likely net benefit from using probiotics resulting primarily from prevention of eczema. The WAO guideline panel suggests using probiotics in: (i) pregnant women at high risk of having an allergic child; (ii) women who are breastfeeding infants at high risk of developing allergy; and (iii) infants at high risk of developing allergy. New evidence is likely to emerge on barrier enhancement as a strategy for AD prevention over the next 5 years, especially through the SCiPAD prospectively planned meta-analysis.
In terms of future research, it is worth exploring new risk factors rather than doing more studies on the same interventions that do not look promising. The comprehensive overview of systematic reviews of epidemiology of allergic diseases conducted by Genuniet et al. (67) is a good place to start and by reconsidering the host of non-specific, specific and internal factors that make up the “exposome” for AD (67, 68). Rather than considering reduction of harmful exposures, exploration of increasing potentially beneficial substances might be considered. Given the inverse relationship between helminth exposure and allergic sensitisation, derivative products that switch off the dysfunctional immune response could be explored further (69). The foetal environment may be a better place to focus than the infant environment. Rather than conducting more probiotic trials, stopping and conducting a more refined analysis of the 28 or so existing studies using individual patient data meta-analysis may help to bridge the gap between cautious recommendation and implementation in order to benefit future generations of children who might otherwise be destined to a life with AD.
Conflicts of interest: Both authors are involved in the Barrier Enhancement for Eczema Prevention (BEEP) study funded by the UK National Institute for Health Research Health Technology Assessment Programme.


 Click to show fullsize
Click to show fullsize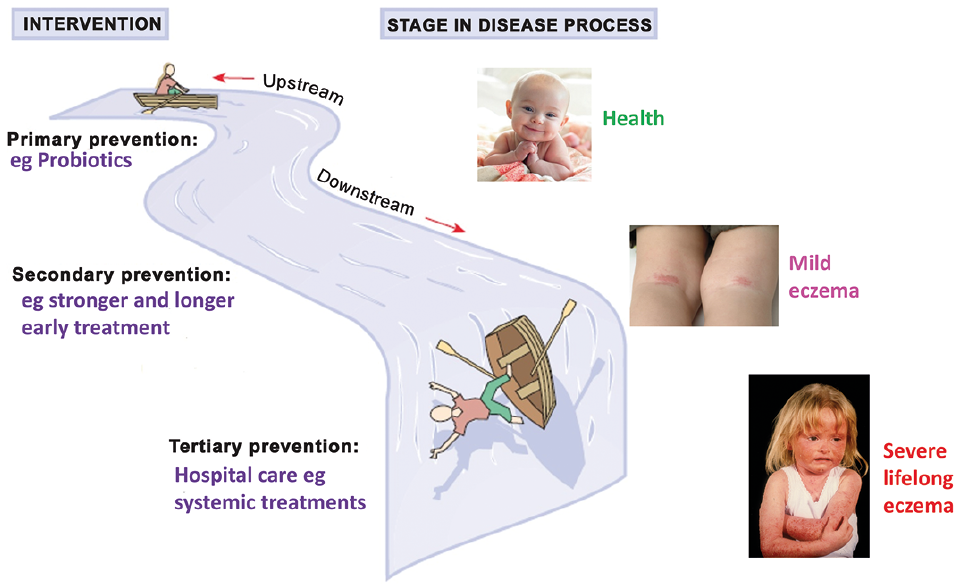 Click to show fullsize
Click to show fullsize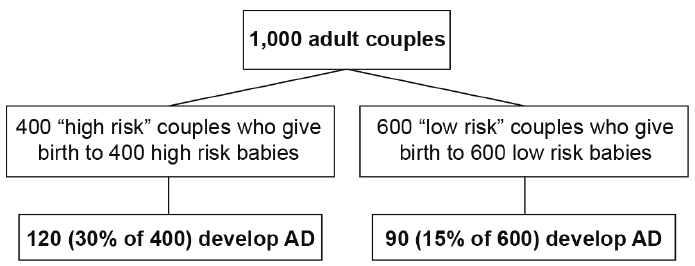 Click to show fullsize
Click to show fullsize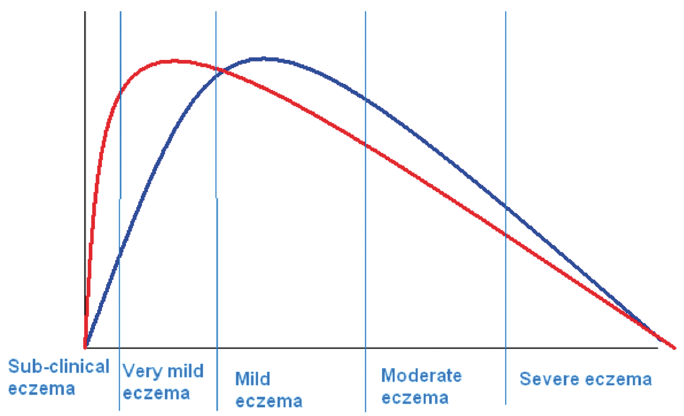 Click to show fullsize
Click to show fullsize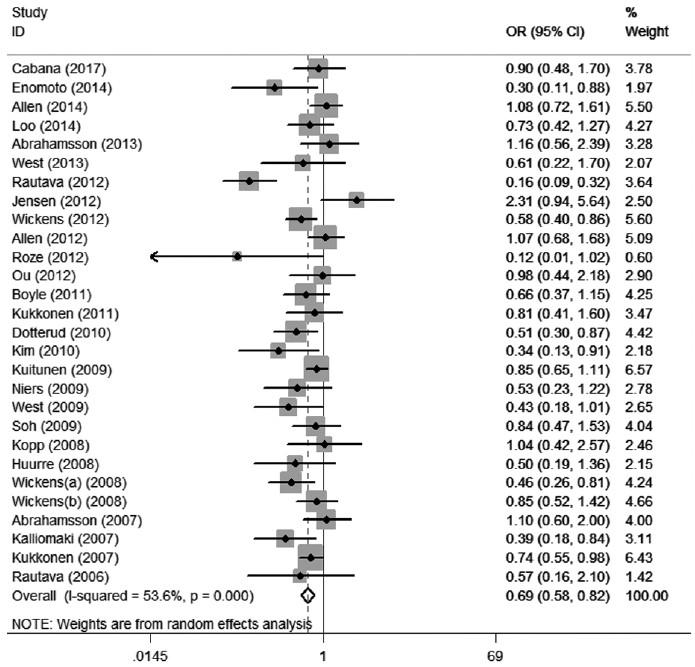 Click to show fullsize
Click to show fullsize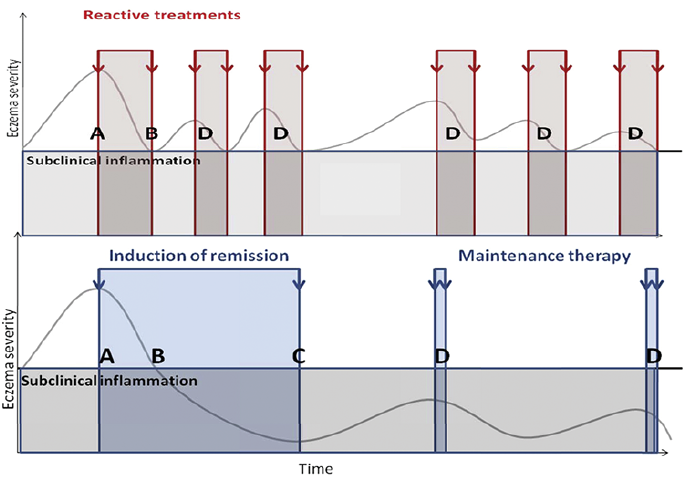 Click to show fullsize
Click to show fullsize