


Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, Tottori University, Yonago, Japan
The pathogenesis of seborrhoeic dermatitis is controversial and remains unclear. Malassezia is considered to be a commensal fungi and is found not only in the stratum corneum but also in hair follicles. It is an important pathogenic factor in seborrhoeic dermatitis. The aim of this study was to clarify the pathogenesis of seborrhoeic dermatitis, morphologically, through comparison with psoriasis vulgaris. Fifteen cases of seborrhoeic dermatitis, 7 of psoriasis, and 6 of normal skin were examined using routine histopathology, immunohistochemistry, and electron microscopy. Macrophages were found to be diffusely distributed in the upper dermis of seborrhoeic dermatitis and psoriasis. In contrast, a significant increase in the number of dendritic cells in the follicular epithelium and dendritic cell clusters in the perifollicular dermis were found only in seborrhoeic dermatitis. Ultrastructural examination of the clusters demonstrated that dendritic cells interacted with lymphocytes, macrophages, and other dendritic cells. In conclusion, folliculotropic distribution of dendritic cells as well as dendritic cell-immune cell clusters play an important role in the pathogenesis of seborrhoeic dermatitis.
Key words: Langerhans cell; inducible skin-associated lymphoid tissue; hair follicles; psoriasis; macrophage; electron micro-scopy.
Accepted May 11, 2020; Epub ahead of print May 18, 2020
Acta Derm Venereol 2020; 100: adv00183.
Corr: Kazunari Sugita, Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, Tottori University, 86 Nishi-cho, Yonago, 683-8503, Japan. E-mail: sugita@tottori-u.ac.jp
Seborrhoeic dermatitis is a common refractory skin disease. The causal factors and disease mechanisms are unknown. The aim of this study was to investigate the morphology of seborrhoeic dermatitis. It was found that dendritic cells, which could control several immune-related cells, had a unique distribution in the skin and formed cell clusters around hair follicles. It was also shown that there was a strong interaction of dendritic cells with other inflammatory cells in the clusters. These suggest the central role of dendritic cells and hair follicles in the aetiology of seborrhoeic dermatitis. This knowledge may be used in developing treatments for the disease.
Seborrhoeic dermatitis is a common, chronic, and relapsing skin disease, with clinical characteristics, such as flaking, scaling, and pruritic erythema in the seborrhoeic areas of the body, including the scalp, face, and trunk (1). The incidence is 1–3% of the general adult population (2, 3). Seborrhoeic dermatitis is a multifactorial disease that needs endogenous and exogenous predisposing factors for its development. The pathogenesis is not completely understood, and there is much controversy in this regard (4–6).
One of the important pathogenic factors of seborrhoeic dermatitis is a fungi of the genus Malassezia (previously known as Pityrosporum), which is a lipid-dependent superficial commensal of skin. This is supported by the fact regarding the positive correlation between yeast density on the skin and the severity of seborrhoeic dermatitis, as well as a high therapeutic efficacy of antifungal agents in seborrhoeic dermatitis (7). Malassezia can hydrolyse human sebum triglycerides through its lipase activity and release metabolites that can disrupt the epidermal barrier function and activate inflammatory responses (8, 9). Furthermore, it is known that Malassezia activates murine macrophages through macrophage-inducible C-type lectin (mincle). Malassezia also induces NLRP3 inflammasome activation and subsequent interleukin (IL)-1β secretion in human antigen-presenting cells including dendritic cells (DC) (10, 11). Seborrhoeic dermatitis is much more common in immunosuppressed patients, such as organ transplant recipients, patients with human immunodeficiency virus infection/acquired immunodeficiency syndrome (HIV/AIDS), and various other malignancies, suggesting that the immune system is important in its pathogenesis (1, 4). Recently, a T-cell receptor transgenic mouse model implicated fungal organisms and CD4+ T-cell lymphopenia in the development of a seborrhoeic dermatitis-like condition (12). There are several studies concerning seborrhoeic dermatitis in the aspect of immunity (6, 9, 13–15), but the exact immunological mechanism is still unknown.
Histopathological features of seborrhoeic dermatitis include spongiosis, psoriasiform hyperplasia, parakeratosis around the follicular opening (“shoulder parakeratosis”), and neutrophils in the crust at the margins of the follicular ostia. Marked psoriasiform hyperplasia and parakeratosis are the main characteristics, especially in chronic lesions, similar to psoriasis (16). There are many clinical similarities between seborrhoeic dermatitis and psoriasis. Differential diagnosis between the 2 conditions can be difficult when both conditions are localized on the scalp with no involvement of other skin sites (17). Current research demonstrates that psoriasis is initiated by an inflammatory immune reaction against autoantigens of the skin, in which dendritic cells, T lymphocytes, macrophages, and neutrophils play a pivotal role (18–20).
To investigate the pathogenesis of seborrhoeic dermatitis, this study focused on the clinical and histopathological similarities between seborrhoeic dermatitis and psoriasis vulgaris. It was hypothesized that the immune reaction of DCs and macrophages against Malassezia or its metabolites may initiate seborrhoeic dermatitis, and it may have a partially overlapping mechanism with psoriasis. There have been no reports focusing specifically on those cells for detailed morphological observation in seborrhoeic dermatitis. Thus, the aim of this study was to investigate the presence and distribution of DCs and macrophages in human seborrhoeic dermatitis skin compared with psoriasis and healthy skin.
Patients
This study retrospectively analysed skin biopsy specimens from 15 patients with seborrhoeic dermatitis of the scalp, who visited our hospital from 2008 to 2017, and received skin biopsies for diagnoses (9 men and 6 women, mean age 55.0 years, range 20–78 years). The study was approved by the ethics committee of the Faculty of Medicine, Tottori University (number 2346) and was conducted in compliance with the principles of the Declaration of Helsinki. The diagnosis was based on both clinical and histological findings, as follows; flaking, scaling, and pruritic erythema localized in the seborrhoeic area, psoriasiform hyperplasia, and spongiosis in the follicular area, with parakeratosis. Normal skin was also obtained from the scalp (3 men and 3 women, mean age 55.8, range 33–73 years). In addition, 7 psoriatic skin biopsy specimens were analysed as a disease control (6 men and 1 woman, mean age 52.9, range 28–70 years). Biopsies were taken from the scalp (n = 2), trunk (n = 2) and limbs (n = 3). All specimens contain hair follicles.
Immunohistochemistry
Immunohistochemical analysis was performed on the sections obtained from formalin-fixed, paraffin-embedded tissue, using antibodies to CD1a (monoclonal mouse antihuman, dilution: 1:100; Dako, Glostrup, Denmark), langerin (CD207) (monoclonal mouse antihuman, dilution: 1:200, Dendritics, France), CD68 (monoclonal mouse antihuman, dilution: 1:1, Dako, Glostrup, Denmark), CD163 (monoclonal mouse anti-human, dilution: 1:50; Novocastra, Newcastle, UK), and dendritic cell lysosome-associated membrane glycoprotein (DC-LAMP) (CD208) (rabbit polyclonal, anti-human, dilution: 1:50; Novus, Centennial, USA). Cell populations were counted by 2 observers at 3 different high-power fields, which were chosen randomly in the follicular or non-follicular areas of the epidermis or dermis. Mean counts from 2 observers were used as data points for quantitative immunohistochemistry analysis. Statistical analysis was performed using the Mann–Whitney test with a 2-tailed p-value of < 0.05 considered statistically significant. These analyses were performed using Statcel version 4.0 software (OMS, Tokyo, Japan).
Transmission electron microscopy
The biopsy specimens, obtained from 3 cases of scalp lesions with seborrhoeic dermatitis, were also cut into several small pieces and processed for transmission electron microscopy (TEM). These samples were fixed in 2.5% glutaraldehyde in 0.1 mol/l phosphate buffer (PB) for 8 h and then washed and post fixed in 1% osmium tetroxide (OsO4) in PB for 1 h. After dehydration through a graded ethanol series, specimens were placed in QY-2 and embedded in Epoxy Resin (TAAB 812 Resin kit, TAAB Laboratories Equipment Ltd, Berkshire, UK). Ultrathin sections, stained with uranyl acetate and lead citrate, were examined with a JEM-1400 transmission electron microscope (JEOL, Tokyo, Japan).
Clinical data of the patients
No significant difference in mean age of patients with seborrhoeic dermatitis (55.0 years) was seen compared with the normal healthy sample (55.8 years) and those with psoriasis vulgaris (52.9 years). The mean disease duration was 3 months (1–60 months). Ten patients were treated with topical steroids before their first visit to our hospital (66.7%). Two had received combination therapy of topical steroids and topical antifungals (13.3%). In order to examine the effect of the treatment, the current study compared the mean number of CD1a+ cells in the follicular epithelium and dermis between treated (n = 10) and untreated seborrhoeic dermatitis groups (n = 5). The number of CD1a+ cells in the follicular epithelium and dermis was significantly higher in both treated and untreated groups compared with the normal group (n = 6). However, there was no statistically significant difference between treated and untreated groups (data not shown).
Distribution of dendritic cells
In order to compare the distribution of DCs and macrophages, immunohistochemical analyses were performed on serial tissue sections from normal skin, psoriasis, and seborrhoeic dermatitis.
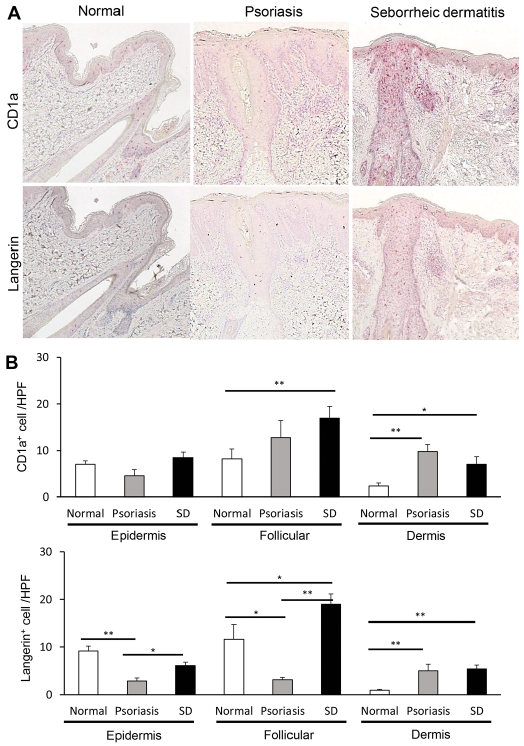
In seborrhoeic dermatitis, both CD1a+ cells and langerin positive cells were nodularly infiltrated and formed cell clusters in the upper dermis. In psoriasis, CD1a+ cells were nodularly infiltrated and formed cell clusters; however, langerin-positive cells were infiltrated in a scattered pattern in the upper dermis (Fig. 1A). Quantitative analysis of immunostaining showed that CD1a+ cells were significantly increased in the follicular epithelium and dermis in seborrhoeic dermatitis, but not in the epidermis, compared with normal skin (Fig. 1B). In psoriasis, CD1a+ cells increased only in the dermis, and there was no significant difference between the normal skin of the epidermis and that of the follicular epithelium. The number of langerin-positive cells was almost the same as that of CD1a+ cells in seborrhoeic dermatitis, but they were significantly reduced in the epidermis and follicular epithelium, in psoriasis. Intriguingly, in seborrhoeic dermatitis, DCs were localized mainly to the follicular epithelium, particularly the infundibulum and isthmus.
Fig. 1. Distribution of dendritic cells in seborrhoeic dermatitis (SD), psoriasis vulgaris, and normal skin. (A) Immunohistochemical staining for CD1a and langerin. (Original magnification, ×200). (B) Mean counts of CD1a+ cells and langerin+ cells per high-power field (HPF) in the epidermis, follicular epithelium, and dermis. *p ≤ 0.05; **p ≤ 0.01.
Distribution of macrophages
Macrophages are classified into classically activated (M1) and alternatively activated (M2) cells. M1 macrophages exhibit potent microbicidal properties and promote strong IL-12-mediated Th1 responses and play a role in the resolution of inflammation (21). To evaluate the distribution of macrophages, CD68 were used as a pan-macrophage marker and CD163 as an optimal M2 macrophage marker. CD68+ cells and CD163+ cells were disseminated throughout the dermis with focal exocytosis in the epidermis and follicular epithelium in seborrhoeic dermatitis and psoriasis (Fig. 2A). The number of these cells in the dermis of both diseases was significantly increased compared with that of normal skin. However, there was no difference in the distribution of macrophages between seborrhoeic dermatitis and psoriasis (Fig. 2B).
Fig. 2. Distribution of macrophages in seborrhoeic dermatitis (SD), psoriasis vulgaris, and normal skin. (A) Immunohistochemical staining for CD68 and CD163. (Original magnification, ×200). (B) Mean counts of CD68+ cells and CD163+ cells per high-power field (HPF) in the epidermis, follicular epithelium, and dermis.
Dendritic cell clusters in the perifollicular areas of the dermis
DCs were nodularly infiltrated and formed cell clusters, whereas macrophages were disseminated in the dermis of seborrhoeic dermatitis and psoriasis (Figs 1A and 2A). Intriguingly, the DC clusters in seborrhoeic dermatitis were observed mainly in the perifollicular area, while those in psoriasis lined up over the upper dermis (Fig. 3A). In other words, DC clusters were found only in the perifollicular dermis of 12 of 15 cases with seborrhoeic dermatitis (80%) and in 2 of 7 cases with psoriasis (28%) (Fig. 3A). This study considered that the DC clusters in the perifollicular area may play a role in the pathogenesis of seborrhoeic dermatitis.
To investigate the function of cell clusters in the perifollicular area of seborrhoeic dermatitis, this study analysed DC-LAMP, which is a mature marker of DC. DC-LAMP-positive cells were observed only in the dermis (Fig. 3B, C). Quantitative analysis showed that increasing of DC-LAMP-positive cells was significant in the dermis, but not in the follicular epithelium or non-follicular epidermis (Fig. 3B).
Fig. 3. Dendritic cell clusters in the dermis. (A) Immunohistochemical staining for CD1a (original magnification, ×200). CD1a+ cell clusters in seborrhoeic dermatitis (SD) were observed in the perifollicular area, while that in psoriasis vulgaris lined up over the upper dermis. Graphs show percentage of cases with perifollicular clusters of CD1a+ cells. (B) Immunohistochemical staining for DC-LAMP (original magnification, ×200). (C) Number of DC-LAMP+ cells in the epidermis, follicular epithelium, and dermis.
Transmission electron microscopy confirmed direct cell-to-cell contact of dendritic cells with other immune cells
To further examine the morphological features of perifollicular DC clusters and the relationship between hair follicles and DC clusters in seborrhoeic dermatitis, ultrastructural analysis of the lesions with TEM was performed. In all 3 cases examined, macrophages, DCs, Langerhans cells (LCs), and lymphocytes were assembled and close to each other in the perifollicular dermis (Fig. 4A, B). The pseudopods of some LCs attached to lymphocytes with electron-dense membrane sites (Fig. 4C). LCs were also attached to macrophages (Fig. 4D). Interactions between DC-DCs, DC-Ly, and DC-Mac were also seen (data not shown). In the follicular epithelium, exocytosis of activated lymphocytes, macrophages, DCs and LCs was observed. These cells were assembled to form “micro-clusters” consisting of 3–5 cells (Fig. 4E), especially at the dermo-epidermo junction. Interactions between DC-DC, DC-LC, and DC-Mac were seen in the “micro-clusters”. Table I presents a summary of the TEM findings.
Fig. 4. (A–D) Ultrastructural findings of perifollicular immune cell clusters in seborrhoeic dermatitis. (B–D) Langerhans cells (LC) and macrophages (M) were assembled and attached to lymphocytes (Ly) with an electron-dense membrane site. In the dermo-epidermo junction of the follicular epithelium, dendritic cells that did not have Birbeck granules (DC). Langerhans cells (LC) and macrophages (M) formed “micro-clusters”. (Bars: (A, E) 10 μm; (B) 5 μm; (C, D) 200 nm).
Table I. Summary of ultrastructural findings of seborrhoeic dermatitis
This study clarified the distribution of DCs and macrophages in seborrhoeic dermatitis and the differences between seborrhoeic dermatitis and psoriasis. First, the number of DCs was significantly increased in the follicular epithelium in seborrhoeic dermatitis. The unique folliculotropic distribution of DCs indicated significance of hair follicles in the pathogenesis of the disease. Hair follicles is equipped with specific immunological properties. This fact gives various microorganisms a residence and allows them to invade into hair follicles (22). Malassezia yeasts also reside in the infundibulum because it contains sebum, a lipid-rich energy source (23). Recent evidence suggests an important role of individual susceptibility to irritant contact dermatitis due to the metabolites of Malassezia (24, 25). It has been reported that the number of DCs in the epidermis is remarkably decreased in irritant contact dermatitis (26–28). In contrast, in our study, the number of DCs in the epidermis was comparable between normal control and seborrhoeic dermatitis (Fig. 1B). In general, ballooning of keratinocytes in the upper epidermis with variable necrosis is noted in irritant contact dermatitis; however, these observations are unusual in the upper epidermis as well as hair follicles in seborrhoeic dermatitis (29). Although the distribution of DCs in the hair follicle in irritant contact dermatitis is unknown, these results, together with the findings of the current study, suggest that the pathogenesis of seborrhoeic dermatitis is somewhat different from that of conventional irritant contact dermatitis. Recently, CD1a, a lipid-presenting molecule on LCs, was found to be important for Th17 cell-mediated dermatitis and facilitates Th17 cell-driven psoriatic skin inflammation (30). LCs in follicular epithelium may be activated by the lipid-antigen and induce psoriasis-like inflammation in seborrhoeic dermatitis.
Secondly, there were DC clusters containing mature DCs and LCs in the perifollicular dermal area in seborrhoeic dermatitis. Ultrastructural examination demonstrated that DCs interacted with lymphocytes and macrophages in the clusters. The clusters might have immunological functions, such as local antigen presentation to lymphocytes or activating macrophages (31). Recently, a leukocyte-clustering structure, named inducible skin-associated lymphoid tissue (iSALT), was proposed to serve as a site for efficient antigen presentation in the skin in mice (32). Although it remains unclear whether iSALT is formed in human skin, iSALT-like leukocyte clusters, which may present antigens to effector T cells, are found in some inflammatory skin diseases, including allergic contact dermatitis, psoriasis, and secondary syphilis (22). In psoriasis, it was reported that the clusters of DC-LAMP positive DCs and T cells were detected in the dermis and the clusters disappeared after treatment with tumour necrosis factor inhibitors (33). In contrast, DC clusters dominantly seen in the perifollicular area of seborrhoeic dermatitis indicate the disease-specific site of local antigen presentation consistent with iSALT.
Furthermore, ultrastructural examination revealed the existence of DCs in the follicular epithelium, which are large cells with dendrites and irregular nuclei, but no Birbeck granules. There were no reports that examined the ultrastructural features of seborrhoeic dermatitis. Hair follicles were known as portal sites where LC precursors enter the epidermis after LCs were depleted (34). The identity of the DCs, without Birbeck granules, in our observations is not clear; however, DCs in the follicular epithelium interacted between themselves or with macrophages and true LCs and formed “micro-clusters”. They might be closely associated with the pathogenesis of seborrhoeic dermatitis, not just the replacement of LC precursors.
In conclusion, DCs play an important role in the pathogenesis of seborrhoeic dermatitis. We suggested that LCs recognized lipid antigens derived from Malassezia in follicular epithelium, then migrated to the perifollicular dermis and formed clusters together with DCs, macrophages, and lymphocytes, and subsequently induced psoriasis-like inflammation in seborrhoeic dermatitis. Further study is needed; for example, focusing on the relationship between DCs and hair follicles in seborrhoeic dermatitis.
This work was partially supported by Grants-in-Aid for Scientific Research (18K16061) and Tottori University Faculty of Medicine Grant.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize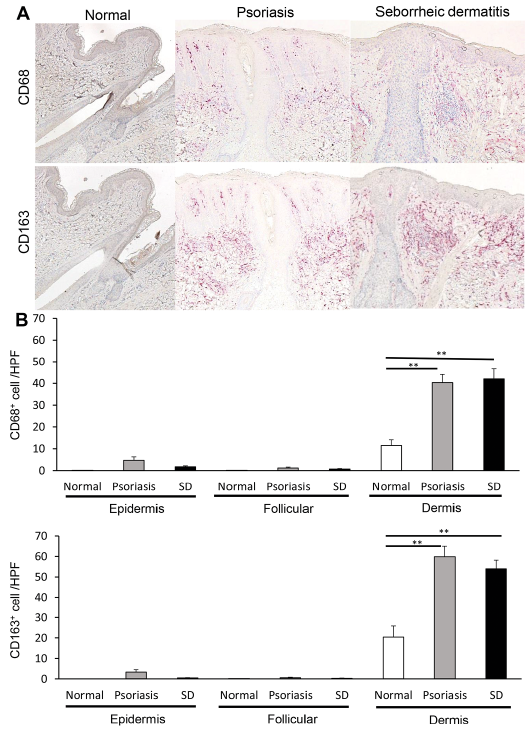 Click to show fullsize
Click to show fullsize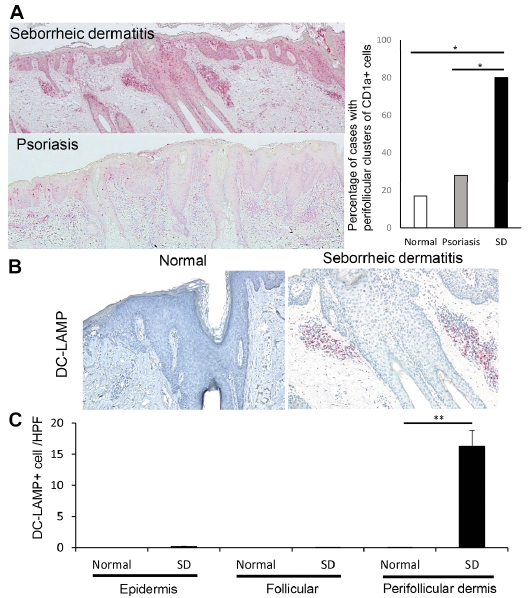 Click to show fullsize
Click to show fullsize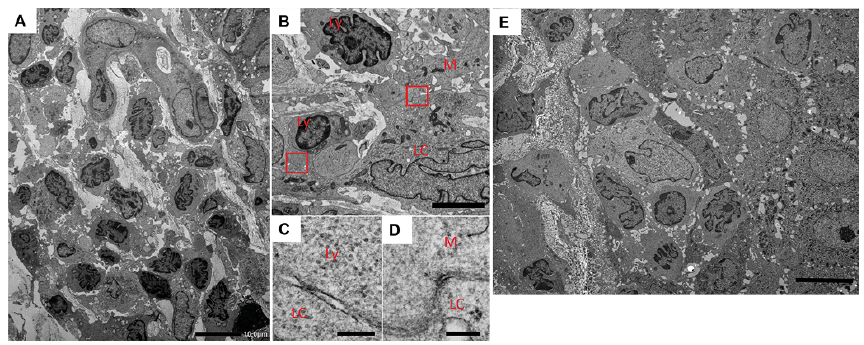 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize