


1Fondazione Policlinico Universitario A. Gemelli IRCCS, UOC di Dermatologia, and 2Università Cattolica del Sacro Cuore, Dermatologia, Rome, Italy
Ultrasonography has proven useful for diagnosis and treatment monitoring in patients with hidradenitis suppurativa. The aim of this study was to assess the clinical response to adalimumab using ultrasound findings. This prospective study collected data on demographic features, disease severity, and hidradenitis suppurativa findings from patients with hidradenitis suppurativa treated with adalimumab. Generalized estimating equations investigated relationships between disease severity measures and clinical/demographic variables. The study included a total of 41 patients with hidradenitis suppurativa who were treated with adalimumab for a mean ± SD period of 50.8 ± 32.2 weeks; range 6–108 weeks). Clinical improvement was observed during adalimumab therapy, with a progressively greater number of patients achieving HiSCR50 response (36.4% at week 52). Disease duration was identified as the most relevant clinical variable affecting disease severity and treatment response. Treatment response was also influenced by treatment duration, with a 4% greater likelihood of achieving HiSCR50 response at each time-point. At the ultrasound examination, subcutaneous involvement of hidradenitis suppurativa lesions was identified as a predictive negative factor for clinical response to adalimumab (HiSCR50 achievement).
Key words: hidradenitis suppurativa; adalimumab; HiSCR50, real-world; ultrasound; eco-color-Doppler.
Accepted May 11, 2020; Epub ahead of print May 18, 2020
Acta Derm Venereol 2020; 100: adv00172.
Corr: Andrea Chiricozzi, Institute of Dermatology, Catholic University, Largo Agostino Gemelli 8, IT-00168 Rome, Italy. E-mail: chiricozziandrea@gmail.com
Adalimumab is the only biologic therapy approved for the treatment of patients with hidradenitis suppurativa, a -chronic and disabling skin condition. This study assessed the effectiveness and safety of adalimumab treatment. The results show that having long duration of disease at the time of starting adalimumab therapy is a negative factor impacting on clinical response. By performing ultrasonography evaluation on skin lesions, hypodermal involvement of hidradenitis suppurativa lesions was identified as a negative predictive factor for clinical response to adalimumab.
Hidradenitis suppurativa (HS) is a chronic, inflammatory, recurrent skin disease, clinically characterized by painful, deep-seated, inflamed lesions in the apocrine gland-bearing areas of the body, most commonly the axillae, groin, and anogenital regions. The estimated prevalence in Europe and the USA varies from 0.1 to 4% (1–4). Epidemiological data suggest that patients with HS may have a higher comorbidity burden than the general population (5–11). Moreover, HS has a significant impact on patient’s quality of life (QoL), causing loss of work productivity, absenteeism, work disability, and impairment of both social life and physical activities (12, 13).
Clinical evaluation of HS, which is commonly performed using both static and dynamic tools, may underestimate the severity of the disease. The use of ultrasonography (US) examination has proven useful for diagnosis as well as for monitoring treatment efficacy, highlighting that higher disease stage and severity are underestimated by clinical scores. US induced management changes in up to 82% of patients with HS (14–16).
Disease severity mostly drives the treatment approach, which includes a number of surgical techniques as well as medical therapies, such as antibiotics, retinoids, immunosuppressive drugs, and biological agents (17). Adalimumab is, to date, the only biologic approved in USA and the EU for treatment of moderate-to-severe HS, although different anti-tumour necrosis factor (TNF)-α and anti-interleukin (IL)17 agents have been used off-label for treating HS (17). Adalimumab demonstrated efficacy in reducing the severity of HS and improving patients’ QoL, as described in 2 large phase 3 trials (PIONEER I and II) (18, 19). Additional studies have reported small cohorts of patients treated with adalimumab in a real-world setting, suggesting an improvement of both clinical manifestations and patient’s QoL (reduction in Sartorius score and Dermatology Life Quality Index (DLQI), respectively) (20).
This study provides evidence of the efficacy and safety of adalimumab in the treatment of HS in a real-world setting, correlating clinical assessment of the therapeutic response with ultrasound findings.
A prospective study was designed including patients affected by moderate-to-severe HS, treated with adalimumab originator at the labelled schedule during the period June 1, 2016–January 31, 2019, at the Institute of Dermatology, Catholic University, Rome, Italy.
Inclusion criteria were: male and female subjects, age ≥ 18 years, with a diagnosis of HS since at least one year, and Hurley stage II–III.
Exclusion criteria were: previous treatment with anti-TNF-α, patients unable to understand and provide informed consent, patients declining a cutaneous ultrasound scan, and those diagnosed with psychiatric disorders. The use of systemic antibiotics for a maximum of 4 weeks or acitretin for 12 weeks was allowed in case of disease flares during adalimumab treatment.
For each patient, the following demographic characteristics and clinical/anamnestic data were collected: age, sex, height, weight and body mass index (BMI), comorbidities, smoking habit, family history of HS, disease duration, age of HS onset, age at diagnosis, anatomical site of lesions, previous and current medical and surgical treatments. Hurley staging system and International HS Severity-Score System (IHS4) were used to assess disease severity (21). Skin symptoms, namely itch and pain, were evaluated by each patient using a 0–10 visual analogue scale (identified as VAS-I and VAS-P, respectively), while patient’s QoL was rated using the DLQI.
Safety and tolerability were assessed by incidence of adverse events (AEs), including mild and serious AEs, clinically significant changes in laboratory values and physical examinations. Quantiferon-TB gold tests and serology for hepatitis B virus (HBV), hepatitis C virus (HCV) and human immunodeficiency virus (HIV) were performed at baseline. The study was approved by the local ethics committee (Protocol ID: 2159 - 28415/18) and conducted in accordance with the guidelines of the Declaration of Helsinki. All eligible patients provided written informed consent.
Ultrasound evaluation
The US examination of HS lesions was conducted by one dermatologist, certified for skin US assessment. Lesions were evaluated using standard real-time compound imaging ultrasound system (Full Digital MyLab Touch, Linear Probe SL3235 High Frequency (Esaote S.p.A, headquartered in Genoa, Italy)) with a 15–18 MHz linear probe. US evaluation included the following features: pseudocyst, abscess, simple tunnel and complex tunnel (connected to each other). In addition, US examination may reveal the presence of 2 specific features of HS lesions: (i) connected fistula, which are usually located in the dermis and upper subcutis and are connected to the base of widened hair follicles; and (ii) hair tracts, consisting of hyperechoic linear structures and representing retained hair tract fragments (22).
Severity of disease was classified according to SOnographic Score of Hidradenitis Suppurativa (SOS-HS) staging (16) at baseline and at weeks 16, 24 and 52, as follows:
In addition to SOS-HS staging, the involvement of dermis and/or subcutis was evaluated.
Each fistula was described according to the Wortsman classification as:
Each lesion was also investigated by power eco-color Doppler to assess the activity of vascularization (meant as surrogate of inflammation) and to describe its distribution in the lesion context (peripheral or central). The activity of vascularization was evaluated semi-qualitatively as mild, moderate, and high. Vascular distribution was assessed as peripheral or internal.
Statistical analysis
Descriptive statistics were calculated for each variable (namely, sex, age, age at HS onset, smoking habit, BMI, waist circumference, disease duration), using frequencies and percentage for categorical variables and mean ± standard deviation (SD) for continuous ones. χ2 test or Fisher’s exact test were used as appropriate for categorical variables. Student’s t-test or Mann–Whitney test were used, as appropriate, for continuous variables (statistical significance was set at p ≤ 0.05). Clinical variables were analysed using the “as observed analysis” to handle missing data. A cross-sectional analysis was conducted through logistic regression with the aim to determine if disease severity at baseline was associated with peculiar ultrasound features of HS. Longitudinal analysis entailed the use of generalized estimating equations (GEE) to investigate whether clinical and demographic variables, and ultrasound findings (independent variables) could predict disease severity measures (dependent variables); each measure was used separately as outcome in different models). Based on the correlation of the outcome(s) scores between time-points, the exchangeable correlation structure was used. The trend over time of some categorical outcomes, such as power Doppler score (0–3) and fistula type (1–3) was analysed by a 2-by-2 comparison between time-points, which was considered more explanatory than GEE, given the low number of patients in each category. The analyses were run analysing the whole study population and a subgroup of patients who completed 52 weeks of continuous adalimumab therapy. Analyses were performed using Stata SE V.12 (Statacorp, College Station, TX, USA).
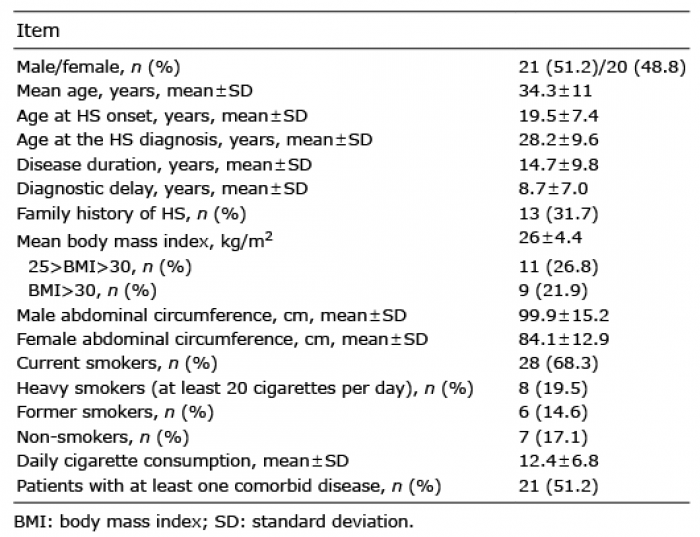
A total of 41 patients affected by moderate-to-severe HS were included in the study. The study population comprised 21 (51.2%) male and 20 (48.8%) female patients, with a mean ± standard deviation (SD) age of 34.3 ± 11.0 years.
Patients’ demographic and clinical features are shown in Table I. Distribution of patients according to disease severity assessed by IHS4 and Hurley score is shown in Table II. At baseline Hurley Stage III, compared with Hurley Stage II, was significantly associated with longer disease duration (24.4 ± 7.9 vs. 10.7 ± 6.9 years, p < 0.00001), more frequent obesity (47.8% vs 14.2%, p = 0.002), and higher waist circumference (101.2 ± 16.6 cm vs. 87.7 ± 13.9 cm, p < 0.00001). Prior to adalimumab therapy, all patients had been treated with at least one systemic therapy. Mean ± SD adalimumab treatment duration was 50.8 ± 32.2 weeks; range: 6–108 weeks), with 87.8% (36/41), 63.4% (26/41), and 53.7% (22/41) of patients achieving at least 16, 24, and 52 weeks of adalimumab treatment, respectively. In a consistent portion of patients (34.2%, 14/41) adalimumab was used in monotherapy. In 65.8% (27/41) of patients the association of adalimumab with other systemic therapies, mostly due to HS flares or disease progression, was performed. Antibiotics were combined with adalimumab in 41.4% (12/27) of cases requiring combination therapy. Two HS cases (one Hurley III male patient and one Hurley III female patient) underwent minor surgical treatments (fistula excision in both cases) without interrupting adalimumab therapy.
Table I. Demographic and hidradenitis suppurativa (HS) features of the study population (n = 41)
Table II. Clinical improvements during adalimumab therapy
Overall, 7 patients were lost to follow-up at different time-points: 2 because of loss of efficacy (one at week 52, and one at week 79), 2 because of adverse events (diffuse plaque psoriasis (week 3) and severe asthenia (week 16)), 2 continued adalimumab therapy in other centres (one at week 45 and one at week 53 moved to another dermatology centre) and one because of patient’s decision (week 94). Overall, mean ± SD IHS4 value from baseline (22.2 ± 14.5) decreased to 15.2 ± 12.2, 15.5 ± 12.2, and 14.1 ± 10.5, after 16-, 24-, and 52-week adalimumab therapy, respectively. Compared with baseline (severe IHS4 patients: 85.4% (35/41)), the number of severe patients reduced during adalimumab therapy to 52.8% (19/36), 53.8% (14/26), 50% (11/22) at week 16, week 24, and week 52, respectively (Table III). When multiple explanatory variables were longitudinally tested by GEE having IHS4 as outcome, longer disease duration was significantly associated with higher IHS4 score values (beta coefficient 0.83, p < 0.0001, meaning an increase of 0.83 in the IHS4 score for each additional year of disease duration) during adalimumab therapy. Sex, smoking habit, and obesity did not significantly impact on treatment response. Results were very similar whether analyses included only patients who completed 52-week treatment (beta coefficient 0.75, p < 0.0001, meaning an increase of 0.75 in the IHS4 score for each additional year of disease duration).
Table III. Ultrasound parameters assessing hidradenitis suppurativa (HS) severity
Similarly to IHS4 score reduction, an increasing percentage of patients achieved hidradenitis suppurativa clinical response HiSCR50 over time (Table II and Fig. 1). GEE having HiSCR50 as outcome, showed that treatment response seemed to increase over time, with a 4% increase at each time-point (odds ratio (OR): 1.04, p < 0.001), and was not significantly influenced by the fact that lesions were present in derma and/or subcutis. This result was confirmed analysing only patients who completed 52-week treatment (OR: 1.04, p < 0.001). This clinical improvement was associated with a slight amelioration of patient’s QoL (Table II).
Fig. 1. Hidradenitis suppurativa clinical response (HiSCR) at weeks (w) 16, 24 and 52. Clinical response to adalimumab therapy was assessed by HiSCR, showing patient rate achieving HiSCR response at each time-point. As observed analysis was performed to handle missing data.
Neither AEs nor clinically significant changes in laboratory values were detected, with the exception of one case of severe asthenia and 2 cases of adalimumab-induced psoriasis (one case of palmoplantar pustular psoriasis, and one case of diffuse plaque psoriasis). Palmoplantar pustular psoriasis was treated successfully with a combination of oral acitretin and adalimumab, whereas severe asthenia and diffuse plaque psoriasis (treated with acitretin) led to treatment discontinuation.
Ultrasound assessment outcomes
Using US examination at baseline, 15 of 41 patients (36.6%) were classified as Type 3, while 26 patients (63.4%) were classified as Type 2 according to the SOS-HS staging. At logistic regression, increasing values of baseline IHS4 score (independent variable) were associated with higher SOS-HS staging; for each point of IHS4 score, the patients had a 24% odds of having a 1-point higher SOS-HS staging (OR 1.24, p = 0.009) after correction for age and sex.
At baseline examination, type 1 fistulas were observed in 3 patients, type 2 fistulas were detected in 24 patients, and type 3 in 15 patients. In addition, 31.7% (13/41) of patients showed connected fistulous tracts, while the presence of retained fragments of hair tracts was detected in 90.24% (37/41) of patients. During adalimumab therapy, improvement of fistula severity was observed, with an increasingly higher number of patients having type 1 fistulas and a concomitant decrease in patients with type 2 and type 3 fistulas (Table III).
HS lesions with dermal involvement occurred more frequently in Hurley Stage II patients (87.5% vs. 21.7%, p < 0.0001), whereas HS lesions with subcutaneous involvement were observed more frequently in Hurley Stage III patients (95.6% vs. 19.6%, p < 0.0001). In the GEE longitudinal model having the localization of lesions in derma and subcutis as independent variables and IHS4 as dependent variable, corrected for treatment duration, the subcutaneous involvement was significantly associated with higher IHS4 score (beta coefficient 15.02, p = 0.004). This result was confirmed by only analysing patients who completed 52-week treatment (beta coefficient 14.95, p < 0.001). Power eco-color Doppler evaluation was performed on all lesions at baseline, showing moderate activity of vascularization in 24 of 41 patients (58.5%) and a high degree of vascular activity in 17 patients (41.5%). Intensity of vascularization significantly dampened after 16-, 24-, and 52-weeks of treatment (Fig. 2). The distribution of vascularization (peripheral vs. central) differed throughout the treatment period, with peripheral vascularization detected in all lesions at baseline and decreased over time (Table III). Similarly, the central vascularization pattern progressively resolved over time. In 2 GEE models having, respectively, peripheral and central vascularization as outcome, and treatment duration in weeks as independent variable, the odds of observing peripheral and central vascularization decreased over time (OR: 0.92 and 0.91 for each time unit, both p < 0.0001). This result was confirmed by analysing only those patients who completed 52 weeks of treatment (OR: 0.92 and 0.89 for each time unit, both p < 0.001).
Fig. 2. Clinical and ultrasono-graphic changes during adali-mumab therapies in patients with hidradenitis suppurativa (HS). Patients responding to adalimumab showed a progressive clinical improvement associated with reduction of vascularization signals assessed by Power Doppler (PD) ultrasound imaging, obtained with 15–20 MHz linear probe. Clinical amelioration at weeks (w) 16, 24 and 52 of gluteal and intergluteal complex fistula in a 43-year-old woman (Case 1: e–h), and of right armpit complex fistula in a 39-year-old man (Case 2: m–p), was associated with reduced signals of vascularization compared with Baseline (Case 1: a–d; Case 2: i–l).
This prospective real-world study provided evidence that adalimumab is effective and safe in treatment of moderate-to-severe HS, as monotherapy and in combination with other therapeutics. Patients with moderate-to-severe HS showed a significant reduction of disease severity during adalimumab therapy, with 36% of patients achieving the HiSCR50 response and 50% reduction in IHS4 at week 52. Disease severity was significantly associated with obesity, waist circumference, and disease duration. Indeed, this study found HS patients with longer disease duration (24.4 ± 7.9 years vs. 10.7 ± 6.9 years), affected by obesity, or having greater waist circumference (101.2 ± 16.3 cm vs. 87.7 ± 13.9 cm), to be significantly more severe (classified as Hurley III). This finding confirmed the pathogenic relevance of obesity in HS, being identified as both comorbid condition and a major risk factor for HS (24–26). Using GEE analysis, this study identified disease duration as the most relevant clinical variable affecting disease severity and treatment response. In particular, patients with longer disease duration had, on average, a higher IHS4 score (0.83 increase in IHS4 for each extra year of disease duration; p < 0.0001). This evidence highlights the importance of both a timely diagnosis and a prompt therapy, as an early therapeutic intervention may result more successful. In addition, continuous and prolonged adalimumab therapy was significantly associated with better clinical outcome, obtaining 4% greater likelihood of achieving HiSCR 50 response at each time-point (week 16, 24, and 52, p < 0.0001). Thus, drug survival emerged as a crucial factor affecting the overall clinical outcome, and any therapeutic strategy to preserve it should be considered clinically valuable. Nevertheless, no guidelines or recommendations are available regarding combination therapies, as underlined by an International Steering Committee that recently proposed recommendations for the therapeutic management of HS, highlighting that the use of combination therapies in HS is limited and not supported by high-quality scientific data (27). This paper reports our experience in combining adalimumab with other therapeutics in case of HS flares or unsatisfactory response, in order to sustain drug survival and enhance adalimumab effectiveness. Because there is paucity of data (28, 29) describing a therapeutic approach combining adalimumab with other systemic therapies, this article may provide valuable evidence of this successful regimen, increasing patient retention and, thus, drug survival. The most commonly prescribed drugs in association with adalimumab were antibiotics (41.3% of combined therapy), which were safe and efficacious in improving clinical response to adalimumab. However, combined therapies may also represent confounding factors in evaluating adalimumab effectiveness, which, together with the small cohort of treated patients and the short observational period, constitute the limitations of this study. Another limiting factor is the variability in the adalimumab treatment duration, as 53.7% of patients achieving at least 52-week treatment, with a consistent number of patients (24.4%) completing 78-week treatment (mean ± SD treatment duration was 50.8 ± 32.2 weeks).
Assessment of the therapeutic response may be challenging, particularly for those HS lesions, such as fistulas, whose improvement is not clinically detectable (14). In these cases, US is proposed as a useful tool to improve the evaluation of treatment response through the assessment of multiple parameters included in the SOS-HS staging, such as the degree of oedema, fibrosis and the distribution of vascularization (assessed by eco-color-Doppler) (14, 16, 30). In the current study, US resulted useful in detecting early signs of therapeutic response (not clinically evident), compared with physical examination. Estimating vascularization, depth of lesions (dermal or subdermal involvement) and whether lesions are interconnected, US detected an overall improvement of US parameters during adalimumab therapy, reflecting the progressive reduction of inflammation (14, 16).
Notably, the vascularization pattern characterizing HS lesions varied during adalimumab therapy: peripheral vascularization and hypervascularization were present in all patients prior to adalimumab therapy, whereas central vascularization was seen in 51.2% of patients. Intensity of vascularization significantly reduced throughout the study period, showing lower peripheral and central vascularization, mostly affected by treatment duration. Indeed, longer treatment duration was associated with lower likelihood in having both peripheral and central vascularization (p < 0.0001).
An additional relevant finding deriving from US examination was represented by the subcutaneous involvement of HS lesions that was associated with significantly lower response to adalimumab therapy (p = 0.004) and, thus, it might constitute a predictive negative factor for clinical response to adalimumab. This evidence is in line with a recently published study identifying fistulas with tendency to deeply penetrate through the subcutaneous fat tissue and muscular fascia without extension to other organs, to be more aggressive as they do not respond appropriately to medical therapies (31). Overall, the implementation of US with clinical examination highly helpful in monitoring disease activity and treatment response, as it detects early signs of therapeutic response (reduction in vascularization) and it identifies negative predictive factors (subcutaneous involvement).
The authors would like to thank Augusta Ortolan, MD, for her valuable support in statistical analysis.
Disclosures. AC served as advisory board member and consultant, and has received fees and speaker’s honoraria or has participated in clinical trials for Abbvie, Biogen, Fresenius Kabi, Leo Pharma, Lilly, Janssen, Novartis, Sanofi Genzyme, and UCB-Pharma. KP served as advisory board member and consultant, and has received fees and speaker’s honoraria or has participated in clinical trials for Abbvie, Almirall, Biogen, Celgene, Galderma, Leo Pharma, Lilly, Novartis, Sandoz, Sanofi Genzyme and Sun Pharma.


 Click to show fullsize
Click to show fullsize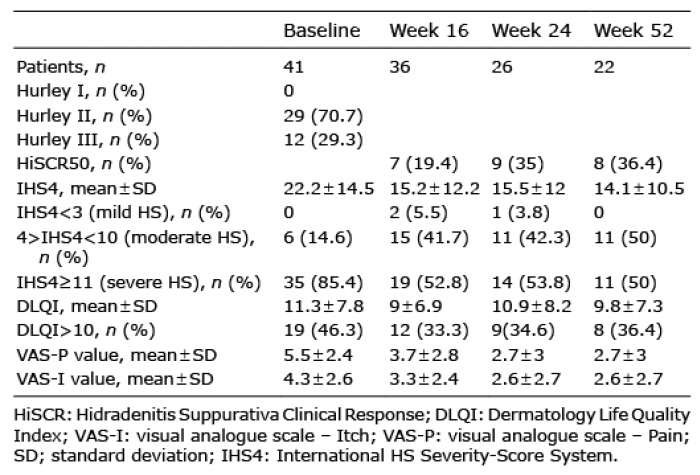 Click to show fullsize
Click to show fullsize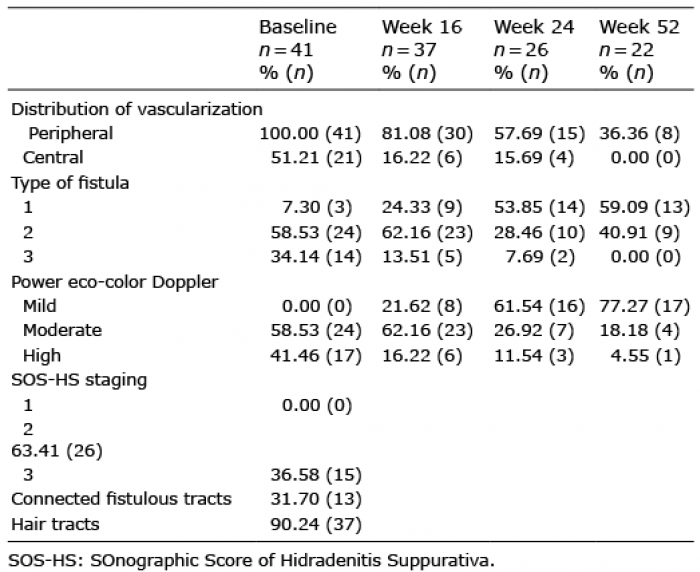 Click to show fullsize
Click to show fullsize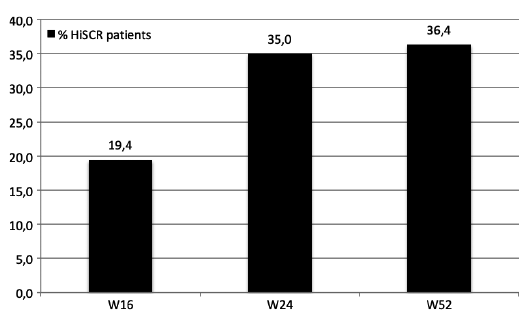 Click to show fullsize
Click to show fullsize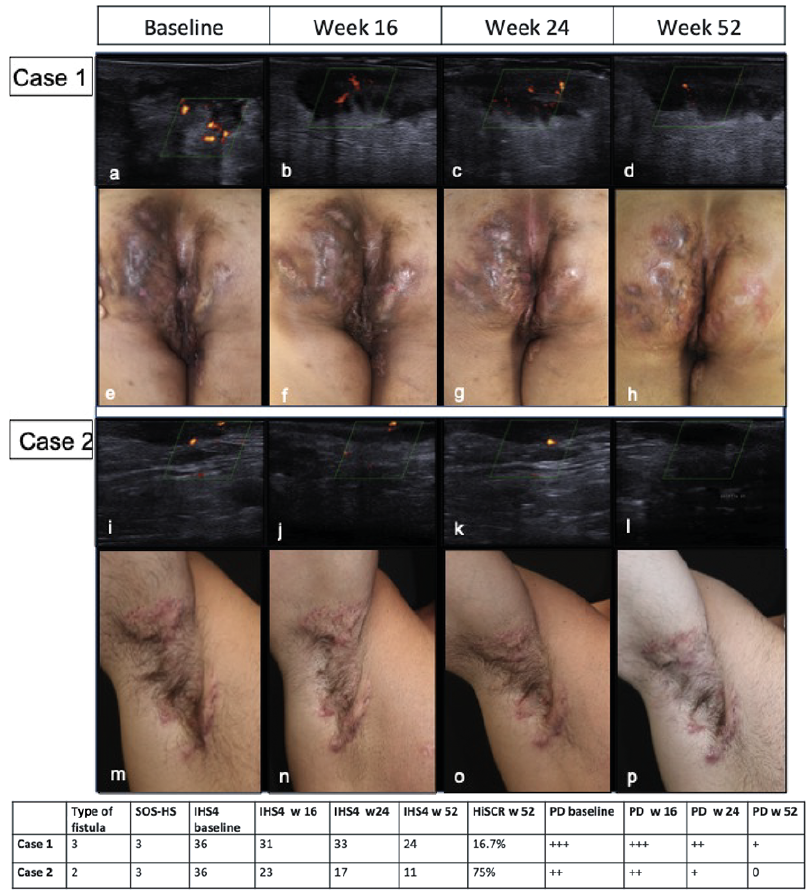 Click to show fullsize
Click to show fullsize