


1Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Würzburg, Germany, 2Center for Dermatooncology, Department of Dermatology, University Medical Center Tübingen, Tübingen, Germany, 3Health Care Direction, Portuguese Air Force, Lisbon, Portugal, 4Department of Dermatology, University Medical Center Göttingen, Göttingen, Germany, 5Department of Dermatology, Skin Cancer Center, Elbekliniken Buxtehude, Buxtehude, Germany, and 6Department of Dermatology, University Hospital Schleswig-Holstein, Kiel, Germany
The approval of BRAF and MEK inhibitors has significantly improved treatment outcomes for patients with BRAF-mutated metastatic melanoma. The 3 first-line targeted therapy trials have provided similar results, and thus the identification of predictive biomarkers may generate a more precise basis for clinical decision-making. Elevated baseline lactate dehydrogenase (LDH) has already been determined as a strong prognostic factor. Therefore, this indirect analysis compared subgroups with elevated baseline LDH across the pivotal targeted therapy trials co-BRIM, COMBI-v and COLUMBUS part 1. The Bucher method was used to compare progression-free survival, objective response rate and overall survival indirectly. The results show a non-significant risk reduction for progression in the subgroup with elevated baseline LDH receiving vemurafenib plus cobimetinib compared with dabrafenib plus trametinib and encorafenib plus binimetinib. Al-though an indirect comparison, these data might provide some guidance for treatment recommendations in melanoma patients with elevated LDH.
Key words: melanoma; BRAF; lactate dehydrogenase.
Accepted May 18, 2020; Epub ahead of print May 25, 2020
Acta Derm Venereol 2020; 100: adv00174.
Corr: Bastian Schilling, Department of Dermatology, Venereology and Allergology, University Hospital Würzburg, Josef-Schneider-Str. 2, DE-97080 Würzburg, Germany. E-mail: schilling_b@ukw.de
Targeted therapy has significantly improved the prognosis of patients with BRAF-mutated metastatic melanoma. Since there are 3 different targeted therapy regimes available, the identification of predictive factors may generate a more precise basis for clinical decision-making. An increased level of lactate dehydrogenase has been determined as a strong prognostic factor. Therefore, the aim of this study was to determine if approved targeted therapy regimes differ significantly in terms of efficacy in patients with elevated lactate dehydrogenase. The study used the Bucher method to indirectly compare the outcome of melanoma patients with elevated lactate dehydrogenase across the pivotal trials co-BRIM, COMBI-v and COLUMBUS part 1.
Small molecule BRAF and MEK inhibitors have clearly improved the prognosis for patients with BRAF mutant metastatic melanoma (1–3). In the coBRIM (NCT01271803) and COMBI-v trials (NCT01597908), combined BRAF and MEK inhibition with vemurafenib plus cobimetinib (coBRIM) or dabrafenib plus trametinib (COMBI-v) improved progression-free survival (PFS), overall response rate (ORR) and overall survival (OS) compared with vemurafenib monotherapy in BRAF-V600-mutated metastatic melanoma. A third trial (COLUMBUS part 1, NCT01909453) compared combined encorafenib plus binimetinib with vemurafenib monotherapy, and also demonstrated an advantage for PFS and ORR in the combination arm (3). While these 3 trials have provided similar results in terms of efficacy in treatment-naive patients with BRAF-V600-mutated metastatic melanoma, the identification of predictive biomarkers may generate a more precise basis for clinical decision-making and patient management.
Well-accepted prognostic factors in patients with metastatic melanoma include disease stage, baseline Eastern Cooperative Oncology Group performance status (ECOG PS) and baseline lactate dehydrogenase levels (LDH) (4, 5). In particular, an elevated baseline level of LDH has been determined as a strong negative prognostic factor in patients with advanced melanoma (6–8), now incorporated into the AJCC staging system as an independent factor (9). LDH is a ubiquitous enzyme that plays a key role in cell metabolism and growth. By catalysing the reduction of pyruvate to lactate, the so-called Warburg effect, LDH creates an acidic milieu that is favourable for tumour angiogenesis and suppression of anti-tumour immune responses (10). In prospective clinical trials evaluating dual MAPKi, an elevated LDH (defined as > local upper limit of normal (ULN)) predicted inferior outcome compared with patients without elevated LDH. The extent of this association was different in coBRIM, COMBI-v and COLUMBUS part 1. However, the clinical significance of these differences has not been analysed comprehensively. To this end, this study conducted an indirect analysis (1) to compare PFS, ORR and OS in the subgroups with elevated baseline LDH from the clinical trials coBRIM, COMBI-v and COLUMBUS part 1 and consequently (2) to interrogate if a particular regime in this particular subgroup might provide greater benefit to patients.
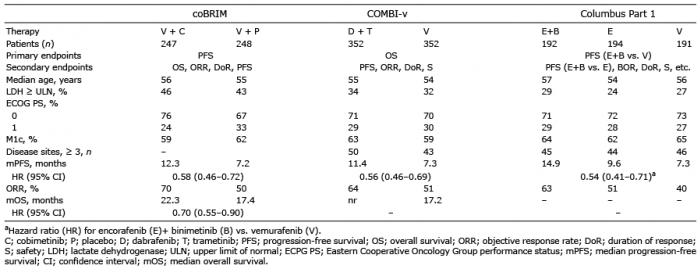
Detailed methods of the particular trials have already been reported (1–3). Briefly, coBRIM, COMBI-v and COLUMBUS part 1 were randomized, double-blind phase 3 trials comparing oral vemurafenib, 960 mg twice daily, plus cobimetinib, 60 mg once daily, for 21 days with placebo and vemurafenib (coBRIM), oral dabrafenib, 150 mg twice daily, plus trametinib, 2 mg once daily, with vemurafenib, 960 mg twice daily, (COMBI-v) or oral encorafenib, 450 mg once daily, plus binimetinib, 45 mg twice daily, with vemurafenib, 960 mg twice daily, or encorafenib, 300 mg once daily, (COLUMBUS part 1). Baseline patient characteristics are summarized in Table I. The primary endpoint of coBRIM and COLUMBUS trial was PFS. Primary endpoint of COMBI-v was OS. Key inclusion criteria were comparable across the studies including patients with unresectable stage III or stage IV BRAF-V600-mutated melanoma, adequate organ functions and ECOG PS 0 or 1. Patients with untreated brain metastases were not eligible.
In this analysis the subgroups with normal and elevated LDH have been statistically analysed using a model for making indirect comparisons of the magnitude of treatment effects without losing the power of randomization (Bucher analysis) (11).
Table I. Patient characteristics
Statistical analysis
The aim of this analysis was the indirect comparison of PFS and OS as well as ORR in the subgroups with elevated LDH levels using the Bucher method. For our analysis, data cut-off dates of 9 May 2014 (PFS), 16 January 2015 (ORR) and 28 August 2015 (OS) for coBRIM; 17 April 2014 (PFS, ORR) and 13 March 2015 (OS) for COMBI-v and 19 May 2016 (PFS) and 7 November 2017 (OS) for COLUMBUS part 1 were used. Due to data availability, the PFS analysis comparing coBRIM with COMBI-v was done using local assessment data, while the comparison with COLUMBUS part 1 used data from the independent central review. As defined by the particular study protocol, all enrolled patients were included in the analysis. The Bucher analysis was based on the assessments of benefit of the Federal Joint Committee (G-BA) for vemurafenib plus cobimetinib (module 5), dabrafenib plus trametinib (module 4) and encorafenib plus binimetinib (module 4) as well as data from Dummer et al. (3). Median OS and PFS were calculated using the Kaplan–Meier method.
Patients’ characteristics
Baseline patients’ characteristics of the 3 studies are summarized in Table I. The percentage of patients with elevated baseline levels of LDH was higher in the coBRIM cohort being treated with vemurafenib plus cobimetinib (n = 112, 46%) than in the combination arms of the COMBI-v (n = 118, 34%) and the COLUMBUS (n = 55, 29%) trials (χ2, p < 0.001). Other prognostic factors, such as ECOG PS and number of patients with M1c disease according to the AJCC 2009 staging system, were comparable across the 3 trials (Table I) (2, 12, 13). Of note, there was a low number of patients with first-line modern immunotherapy in the COLUMBUS part 1 trial (encorafenib + binimetinib group: 7 (4%) ipilimumab, 1 (1%) anti-PD-1 or anti-PD-L1; vemurafenib group: 7 (4%) ipilimumab, 0 (0%) anti-PD-1 or anti-PD-L1).
Progression-free survival
Median PFS in the combination arms was 12.3 months for vemurafenib and cobimetinib (coBRIM, data cut-off 16 January, 2015, median follow-up 14.2 months), 11.4 months for dabrafenib and trametinib (COMBI-v, data cut-off 17 April, 2014, median follow-up 10 months) and 14.9 months for encorafenib and binimetinib (COLUMBUS part 1, data cut-off 19 May, 2016, median follow-up 14.4 months) (1–3). In all 3 studies median PFS was significantly longer in the combination arms than in those treated with vemurafenib monotherapy. Table I shows the corresponding hazard ratios (HR) for progression or death comparing vemurafenib and dual MAPKi regimes.
Across the 3 trials, the subgroups with normal baseline level of LDH clearly benefited from the combination therapy (Fig. 1), whereas only the coBRIM trial could show an equal advantage for the subgroup with elevated baseline levels of LDH (HR 0.57 (95% confidence interval (95% CI), 0.42–0.78), data cut-off 16 January 2015) (Fig. 1) (1). Kaplan–Meier estimates of PFS for the subgroups with elevated LDH derived from coBRIM and COMBI-v are shown in Fig. 2A.
Fig. 1. Progression-free survival (PFS) subgroup analyses for lactate dehydrogenase (LDH) for coBRIM (data cut-off 16 January 2015), COMBI-v (data cut-off 17 April 2014) and COLUMBUS Part 1 (data cut-off 19 May 2016). C: cobimetinib; V: vemurafenib; D: dabrafenib; T: trametinib; E: encorafenib; B: binimetinib; CI: confidence interval; ULN: upper limit of normal (references 1–3, 14 and G-BA-Bericht: Dossier zur Nutzenbewertung von Dabrafenib. Stand 16.09.2015).
Fig. 2. Kaplan–Meier estimates for (A) median progression-free survival (mPFS) and (B) median overall survival (mOS) in the subgroups with elevated lactate dehydrogenase (LDH) for coBRIM (data cut-off 16 January 2015 for PFS and 28 August 2015 for OS) and COMBI-v (data cut-off 17 April 2014 for PFS and 13 March 2015 for OS). C: cobimetinib; V: vemurafenib; D: dabrafenib; T, trametinib; HR: hazard ratio (reference 1, and Robert C. ESMO 2016. Oral presentation).
Using the Bucher method, an indirect comparison of PFS, OS and ORR data from coBRIM, COMBI-v and COLUMBUS part 1 was performed. In this indirect comparison, a non-significant risk reduction for progression or death for patients with elevated baseline LDH receiving vemurafenib plus cobimetinib (data cut-off 9 May 2014) was found. When compared with dabrafenib plus trametinib (data cut-off 17 April 2014), a 24% risk reduction (HR 0.76 (95% CI, 0.48–1.23)) and compared with encorafenib plus binimetinib (data cut-off 19 May 2016), an 11% risk reduction (HR 0.89 (95% CI, 0.50–1.58)) was observed (Table II).
Table II. Bucher analysis for the subgroups with elevated lactate dehydrogenase (LDH)
Overall response rate
The objective response rate was 70% (172/247 patients) in the vemurafenib plus cobimetinib group vs. 50% (124/248 patients) in the vemurafenib plus placebo group (coBRIM, data cut-off 16 January 2015); 64% (226/351 patients) in the dabrafenib plus trametinib group vs. 51% (180/350 patients) in the vemurafenib monotherapy group (COMBI-v, data cut-off 17 April 2014) and 63% (121/192 patients) in the encorafenib plus binimetinib group vs. 40% (77/191 patients) in the vemurafenib monotherapy groups (COLUMBUS part 1, data cut-off 19 May 2016) (1–3). The indirect comparison showed an advantage for vemurafenib plus cobimetinib (data cut-off 16 January 2015) compared with dabrafenib plus trametinib (data cut-off 17 April 2014) in the subgroup with elevated baseline levels of LDH (HR 1.35 (95% CI, 0.88–2.07). ORR data for COLUMBUS were not available.
Overall survival
Median OS in the combination arms was 22.3 months for vemurafenib and cobimetinib (coBRIM, data cut-off 28 August 2015) and was not reached for dabrafenib and trametinib (COMBI-v, data cut-off 17 April 2014) (2) and encorafenib and binimetinib (COLUMBUS, data cut-off 19 May 2016) (3). In updated analyses, the OS was significantly longer in the combination arms compared with BRAF inhibitor monotherapy across all 3 trials (Fig. 3) (14, 15). Fig. 2B shows OS survival curves for coBRIM and COMBI-v for the subgroups with elevated LDH. For COLUMBUS, such OS data from patients with elevated LDH were not available.
In the subgroup of patients with elevated baseline levels of LDH, the indirect comparison showed a similar risk of death for patients receiving vemurafenib plus cobimetinib (data cut-off 28 August 2015) or dabrafenib plus trametinib (data cut-off 13 March 2015) (HR 0.95 (95% CI, 0.61–1.49)) (Table II). A slight and non-significant risk reduction for death by 19% was found when coBRIM was compared with COLUMBUS part 1 (data cut-off 7 November 2017) (HR 0.81 (95% CI, 0.48–1.37)) (Table II).
Fig. 3. Overall survival (OS) subgroup analyses for lactate dehydrogenase (LDH) for coBRIM (data cut-off 28 August 2015), COMBI-v (data cut-off 17 April 2014) and COLUMBUS Part 1 (data cut-off 17 November 2017). C: cobimetinib; V: vemurafenib; D: dabrafenib; T: trametinib; E: encorafenib; B: binimetinib; CI: confidence interval; ULN: upper limit of normal. (1–3, 14 and G-BA-Bericht: Dossier zur Nutzenbewertung von Dabrafenib. Stand 16.09.2015).
This study undertook an indirect analysis in BRAF-V600 mutated patients treated with combined BRAF and MEK inhibition with elevated baseline levels of LDH. In pooled analyses reported recently, baseline levels of LDH, ECOG PS, number of involved organ systems and baseline sum of longest diameter of target lesions (SLDs) were identified as key predictive factors for PFS and OS in BRAF-V600-mutated patients treated with combined BRAF and MEK inhibition (6–8). In particular, baseline LDH level was the strongest predictive factor across all 3 trials. Therefore, our analysis focused on the comparison of patients with elevated baseline LDH level to further investigate PFS, ORR and OS comprehensively across the 3 first-line targeted therapy (TT) trials in this particular subgroup.
Two major clinical decisions need to be addressed in patients with advanced BRAF-mutant melanoma. Firstly, patients can either receive an anti-PD-1 based immunotherapy or dual MAPKi. Since no prospective head-to-head data are available, this decision is based mainly on patient characteristics and preference as well as the physicians’ preference. Looking at data from a survey conducted in melanoma experts, symptomatic disease, a high tumour burden and elevated baseline LDH are features associated with using dual MAPKi as first-line treatment (16). Recently, we were able to show this association in a retrospective study (17). When comparing consecutive patients receiving either dual MAPKi (n = 195) or PD-1 monotherapy (n = 106), the TT cohort was significantly enriched with patients showing non-pulmonary visceral metastases and an elevated LDH. Secondly, the specific regime needs to be chosen. If dual MAPKi is recommended, 3 different combinations are approved by FDA and EMA. In terms of overall efficacy, no regime seems to be superior to the others. However, a given combination might provide greater benefit in a particular subgroup of patients.
Although indirect comparisons of pivotal trials warrant great caution, the usage of vemurafenib as comparator coBRIM, COMBI-v and COLUMBUS part 1 allows to perform a Bucher analysis (18). Looking at the vemurafenib monotherapy arms, results indicate similar response to treatment and prognosis due to resemblance across multiple endpoints (e.g. PFS and OS) in the respective vemurafenib groups (1, 3, 17). Prognostic factors, such as ECOG PS and degree of organ involvement, were comparable across the trials (Table I) (2, 12, 13). However, the coBRIM trial included the highest percentage of patients with elevated baseline levels of LDH in the combination arm (46%) compared with only 34% in the COMBI-v and 29% in the COLUMBUS trial (1–3). In real-world datasets, up to 48% of patients receiving dual MAPKi first-line showed an elevated LDH resembling the coBRIM cohort (19, 20). Although an elevated baseline LDH accounts for a worse outcome, the HR for progression or death in the total trial populations was comparable across the 3 trials (Table I). This indicated an advantage of vemurafenib plus cobimetinib in the subgroup with elevated baseline LDH. The coBRIM data confirmed this hypothesis regarding a PFS advantage of combined BRAF and MEK inhibition with vemurafenib plus cobimetinib compared with a vemurafenib monotherapy independent of the baseline LDH level (Fig. 1). Consequently, BRAF-V600 mutated patients with an elevated baseline LDH level might benefit from a combined TT with vemurafenib and cobimetinib to a similar extend as patients with normal LDH do when compared with vemurafenib monotherapy. This could not be demonstrated for dabrafenib plus trametinib or encorafenib plus binimetinib (Fig. 1). The Bucher analysis confirmed these findings showing a non-significant advantage for vemurafenib plus cobimetinib in the subgroup with elevated baseline LDH compared with dabrafenib plus trametinib and encorafenib plus binimetinib regarding PFS (Table II). Although this retrospective indirect Bucher analysis does not allow an exclusion of all selection bias, our results indicate that the LDH level should be considered when choosing a specific BRAF and MEK inhibitor to achieve disease control.
In contrast to the PFS data our analysis did not affirm a beneficial effect of vemurafenib plus cobimetinib compared with dabrafenib and trametinib, and showed only a slight advantage compared with encorafenib and binimetinib regarding OS. Likewise, the coBRIM data do not provide an OS advantage for combined TT compared with vemurafenib monotherapy. Therefore, the choice of a particular BRAF and MEK inhibitor combination seems to have no impact on OS. However, when interpreting efficacy results, such as OS, prior and subsequent treatment regimens, such as immunotherapies, as well as prognostic factors apart from LDH have to be taken into consideration, creating a potential bias.
Besides efficacy, safety and tolerability are of high clinical relevance and have an impact on treatment recommendations. Distinct patterns of treatment-related adverse events can be found in melanoma patients receiving dabrafenib + trametinib, vemurafenib + cobimetinib or encorafenib + binimetinib. Pyrexia is most frequently observed in patients receiving dabrafenib + trametinib, while vemurafenib + cobimetinib causes the highest number of cutaneous adverse events (AEs), and encorafenib + binimetinib leads to more nausea and constipation than the other combinations (1–3). In an indirect comparison similar to ours, a lower incidence of treatment-related AEs was found for dabrafenib + trametinib compared with vemurafenib + cobimetinib (18). However, when looking at any AE, serious AEs or AEs leading to treatment discontinuation, no differences were observed. Regarding OS and PFS (dabrafenib + trametinib vs. vemurafenib + cobimetinib), Daud et al. calculated a HR of 0.94 and 1.05, respectively, when applying the Bucher method. In contrast to our indirect comparison, earlier data cuts were used and most importantly, the total patient populations of the combination arms were analysed.
We cannot provide any data explaining the differences observed. Lactate accumulating in the tumour microenvironment might cause acidification, decreasing the pH (19). Since it is known that bioavailability of dabrafenib is dependent on pH, while that of vemurafenib is not (20), our hypothesis is that antineoplastic activity of dabrafenib, but not vemurafenib, is pH dependent. Experimental and pharmacokinetic data are needed to test this hypothesis.
Elevated LDH is a very important biomarker in advanced melanoma, and has been incorporated into the AJCC Melanoma Staging system since 2009 (5). Three recent pooled analyses confirmed an elevated LDH as predictive factor for shorter PFS and OS in melanoma patients receiving combined TT (6–8). In the real-world setting, melanoma patients receiving palliative MAPKi first-line have poor prognostic features, including, but not limited to, elevated LDH (21, 22). There might be other subgroups in which a particular treatment regime might tend to be superior to the others. However, taking other biomarkers, such as involvement of particular organs or the sum of lesions diameters, into account was not possible. Patient cohorts are slightly heterogeneous across the 3 trials and more importantly, the way the trials are reported limits the availability of data for comparisons.
In conclusion, there is no statistically significant difference in efficacy between the 3 TT couples using the Bucher method. However, our data indicate a trend towards a lower risk for progression or death in melanoma patients with elevated LDH when receiving vemurafenib + cobimetinib in comparison with dabrafenib + trametinib and encorafenib + binimetinib as first-line therapy. In light of the current preference to use dual MAPKi instead of immune-checkpoint blockade in patients with poor prognostic features including elevated LDH, our indirect analysis might provide a rationale to use a specific treatment regime. However, this finding needs to be validated prospectively. Although a Bucher analysis partially retains the randomization of the individual trials, data provided by an indirect comparison must be interpreted with caution.
The authors would like to thank Susanne Schwenke from Schwenke Consulting for performing the statistical analyses. No specific funding was received to perform this study. This publication was supported by the Open Access Publication Fund of the University of Wuerzburg.
Conflicts of interest. VG has received honoraria from Bristol-Myers Squibb (BMS) and reports travel support from Novartis, Pierre Fabre Pharmaceuticals, BMS, Merck Sharp & Dohme (MSD) and Sanofi Genzyme; outside the submitted work. TA reports travel support from Novartis, personal fees and travel support from BMS, outside the submitted work. CG reports grants and personal fees from Novartis, personal fees from Pierre Fabre, grants and personal fees from Roche, during the conduct of the study; personal fees from Amgen, grants and personal fees from BMS, personal fees from MSD, grants and personal fees from Neracare, personal fees from Philogen, personal fees from Sanofi, outside the submitted work. K-MT reports advisory roles for or has received honoraria from Roche, Novartis, Pierre Fabre, BMS, MSD and LEO; travel support from Roche, Novartis, Pierre Fabre, BMS and LEO; outside the submitted work. PM reports personal fees, non-financial support and other from Pierre Fabre, GSK, MSD, Merk Germany, Roche, BMS, Novartis and Sanofi; outside the submitted work. AH has received clinical trial support from Amgen, BMS, Merck Serono, MSD, Novartis, Philogen, Pierre Fabre, Provectus, Regeneron and Roche and honoraria or consultancy fees from Amgen, BMS, Merck Serono, MSD, Novartis, OncoSec, Philogen, Pierre Fabre, Provectus, Regeneron and Roche. BS reports advisory roles for or has received honoraria from Pierre Fabre Pharmaceuticals, Incyte, Novartis, Roche, BMS and MSD, research funding from BMS, Pierre Fabre Pharmaceuticals and MSD, and travel support from Novartis, Roche, BMS, Pierre Fabre Pharmaceuticals and Amgen; outside the submitted work.


 Click to show fullsize
Click to show fullsize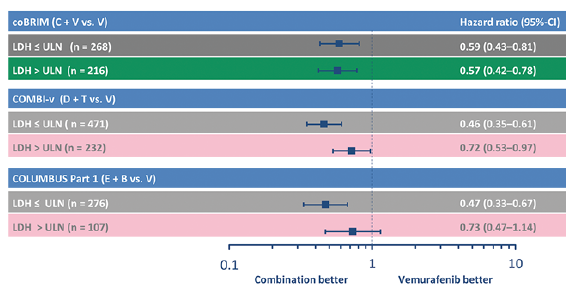 Click to show fullsize
Click to show fullsize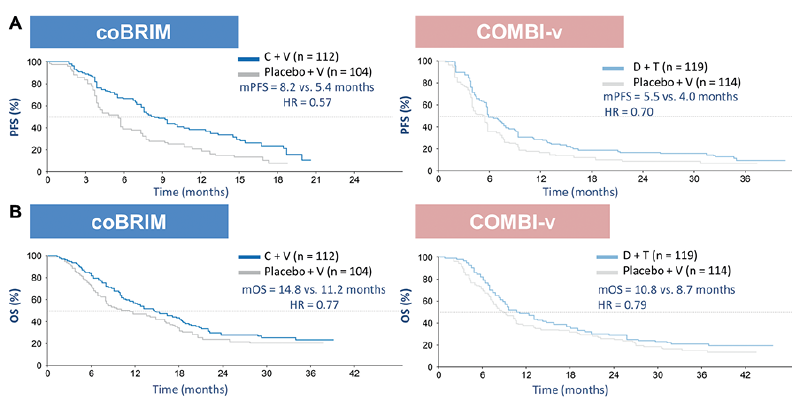 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize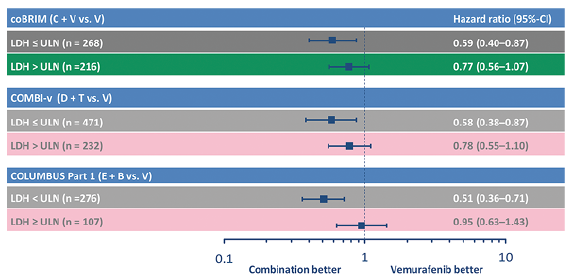 Click to show fullsize
Click to show fullsize