


Departments of 1Dermatology, 5Virology and 6Pathology, Ho?pital Cochin, APHP.CUP, Site Tarnier- 89 rue d’Assas, FR-75006 Paris, 2University of Paris, Paris, Departments of 3Dermatology and 9Ophthalmology, Ho?pital Henri Mondor, AP-HP Créteil, 4Université Paris-Est Créteil, Val de Marne, Créteil, 7Department of Pathology, Hôpital Pitié Salpêtrière, AP-HP Paris, 8Sorbonne University, Paris, and 10Reference Center for Toxic Bullous Dermatoses and Severe Drug Reactions, Créteil, France. *E-mail: nicolas.dupin@aphp.fr
Accepted May 28, 2020; Epub ahead of print Jun 8, 2020
Acta Derm Venereol 2020; 100: adv00181
Erythema multiforme (EM) is an acute polymorphous mucocutaneous eruption characterized by target lesions typically located on acral extremities. Erythema multiforme major (EMM) is defined as EM involving at least two mucosal sites (1). Unlike Stevens-Johnson syndrome (SJS), which is mostly caused by drugs, EM is a hypersensitive response to infection (2). Herpes simplex virus (HSV) and Mycoplasma pneumoniae are the most common triggers.
Human adenovirus (HAdV) has been implicated in both EMM and SJS (3, 4), and has also been linked to a clinical entity resembling EMM called ectodermosis erosive pluriorificialis (5).
HAdV is a double-stranded DNA virus, classified into 7 species (A to G), with at least 100 different types (6). HAdV-D37 is a frequent cause of keratoconjunctivitis that has also been reported in urethritis, sometimes concomitantly (7, 8). Its contagiousness necessitates isolation of the patient (9). We describe here two cases of EMM induced by adenovirus. We investigated the role of adenovirus in the pathogenesis of the various mucosal lesions observed.
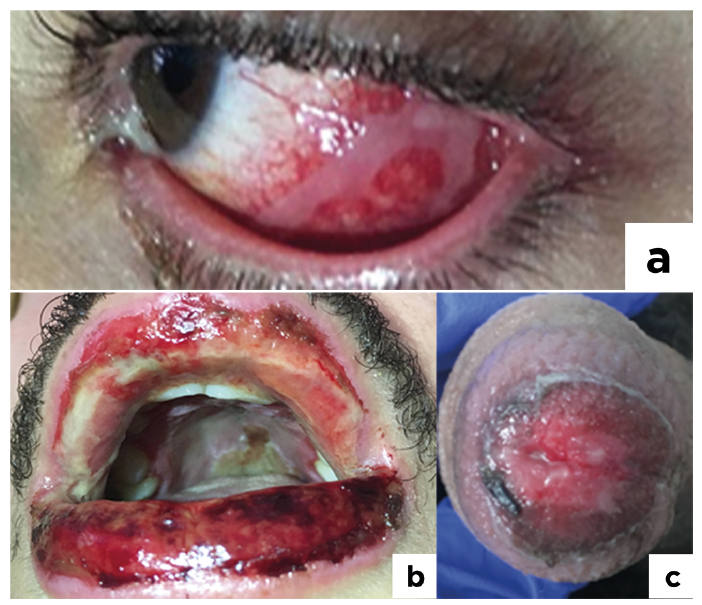
Case 1. A 23-year-old man was admitted to the dermatology department with painful red eyes and oral lesions associated with dysphagia, dysuria and fever. Examination showed bilateral conjunctival inflammation with purulent flow and pseudomembranes on the left eye (Fig. 1a), haemorrhagic crusts on the vermilion zone of the lower and upper lips and extensive erosions involving the buccal mucosa (Fig. 1b), periurethral meatus erosion (Fig. 1c) and 5 targetoid lesions on the upper and lower limbs. Serological tests for HSV and Mycoplasma pneumoniae, and PCR tests on mouth, penis head and ocular lesions were negative. Serological tests for adenovirus were positive (titre > 256). HAdV PCR detected high titres of the virus in lacrimal and genital swabs (Table I), with genotype D37 identified in all positive samples. No viral DNA was detected in blood, urine, skin or saliva specimens. Microscopy analysis of a skin biopsy sample revealed a combination of basal cell hydropic degeneration and focally rounded, intensely eosinophilic, apoptotic keratinocytes associated with a moderate superficial dermal lymphocytic infiltrate. Immunohistochemistry on the skin biopsy specimen with a monoclonal antibody against adenovirus was negative. Symptomatic treatments, such as intravenous hydration, analgesics, and ocular steroid therapy, were introduced, and the lesions regressed within 7 days.
Fig. 1. Case 1. (a) Conjunctival inflammation with pseudomembranes. (b) Erosive and crusted lesions of the lips. (c) Peri-meatal erosions.
Table I. Adenovirus PCR (qualitative and quantitative) and genotyping results for Case 1
Case 2. A 37-year-old man was referred to our dermatology department for pruritic lesions of the extremities, lip erosions and impaired visual acuity. Clinical examination revealed typical target lesions on the palms and soles (Fig. 2), severe bilateral conjunctivitis, with haemorrhagic and reversible pseudomembranes, extensive erosions of the lips, hard palate, and inner cheeks. Serological tests and nasopharyngeal PCR for Mycoplasma pneumoniae were negative. Serological tests for HSV were positive for IgG, but PCR for HSV 1 and 2 on buccal lesions was negative. Adenovirus PCR was positive for the nasopharyngeal sample, and negative for blood. Ocular specimens were not collected for viral testing. The patient was given oral prednisone (1 mg/kg per day) for one week, and valaciclovir, which was introduced before obtaining the PCR results. Topical treatments, including steroids for skin lesions, Vaseline and ocular ointments containing vitamin A, led to a rapid regression of the pseudomembranes, within a week.
Fig. 2. Case 2. Typical target lesions of the palm.
We report two cases of EMM secondary to adenovirus, with a severe specific ocular phenotype. Adenovirus is often responsible for severe contagious pseudomembranous keratoconjunctivitis, sometimes concomitant to urethritis (7, 8). EMM is considered to be a hypersensitivity reaction to microorganisms, the pathophysiology of which remains unclear. In cases of HSV-associated EMM, HSV DNA has been detected in skin lesions (10), but this finding remains controversial, and some authors consider HSV-associated EMM to be due to autoimmune cross-reactivity (11). Both our cases had keratoconjunctivitis with pseudomembranes. In case 1, the high ocular and genital loads of adenovirus D 37 suggested a direct viral origin. By contrast, adenovirus DNA was not detected in skin lesions, buccal erosions, blood or urine. These findings strongly suggest that ocular and genital damage was directly linked to the presence of the adenovirus in the absence of viremia, whereas buccal and cutaneous lesions seemed to be reactional and typical of EMM (12). The symptoms of our patients resemble ectodermosis erosive pluriorificialis, which has been attributed to adenoviral infection in the past (5). We recommend searching for adenovirus in patients presenting EMM with a predominantly ophthalmological phenotype. Adenoviruses are highly contagious pathogens. Rapid diagnosis is, therefore, vital, and patient isolation is recommended (13), to prevent contamination and dissemination of the viral infection to the patient’s contacts and nursing staff.


 Click to show fullsize
Click to show fullsize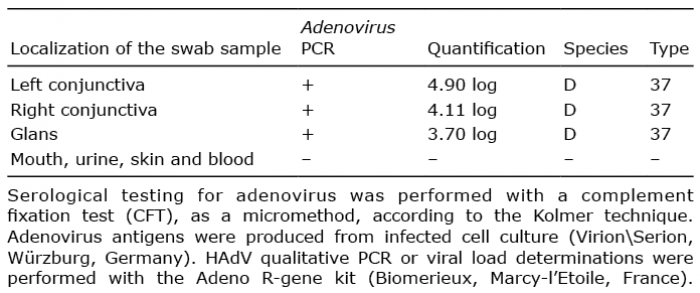 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize