


Section of Dermatology - Department of Health Sciences, University of Genoa, Ospedale Policlinico San Martino – IRCCS, Genoa, Italy. E-mail: rs.gallo@unige.it
Accepted May 28, 2020; Epub ahead of print Jun 8, 2020
Acta Derm Venereol 2020; 100: adv00191
Dupilumab is the first targeted biological therapy approved for the treatment of adult patients with moderate-to-severe atopic dermatitis (AD). It is a human monoclonal antibody that targets the alpha subunit of the interleukin (IL)-4 receptor shared by both IL-4 and IL-13, which are secreted by CD4+ lymphocytes. Its main adverse effects include injection site reactions, nasopharyngitis and conjunctivitis (1). Although it has been reported to improve alopecia areata (AA) (2) there have been increasing reports of AA and AA-like reactions in patients with AD treated with dupilumab (2–12). We report here a patient who developed massive hair shedding, mimicking AA, after 8 weeks of starting dupilumab.
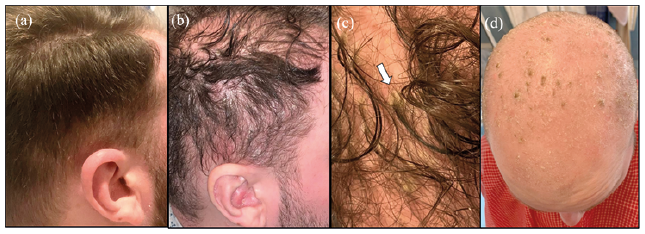
A 24-year-old man, with neither family nor personal history of AA or psoriasis, presented with severe adult-onset AD of 5-year duration that was recalcitrant to topical corticosteroids and systemic, 3 mg/kg/day, ciclosporin. Further to a diagnosis of ulcerative colitis, he had also been taking 10 mg/day prednisolone and 800 mg ×3/day salazopyrin for one year. His Eczema Area and Severity Index (EASI) score was 24. Hence, after a loading dose of 600 mg, dupilumab, 300 mg subcutaneously, was started, while cyclosporine and prednisolone were tapered and stopped. The patient experienced rapid improvement in his AD. However, after 6 weeks he developed dermatitis suggestive of inverse psoriasis in the armpits, navel and intergluteal cleft, associated with erythema and scaling of the scalp. Itraconazole, 200 mg/day, and an antifungal/corticosteroid medication induced remission of the psoriasis-like lesions on the body within 10 days. However, the scalp dermatitis persisted and 8 weeks after starting dupilumab the patient developed abrupt shedding of hair on the entire scalp, with tufts of hair held together by conglomerated scales or casts, on a background of diffuse erythema and scaling (SALT (Severity of Alopecia Tool) scored 71.6) (Fig. 1). Topical clobetasol was started and dupilumab was continued until 4 weeks later, when both his atopic dermatitis and alopecia worsened (Fig. 1d). The patient declined a biopsy of the scalp. Dupilumab was then discontinued and ciclosporin, 3 mg/kg/day, was re-started. Within 4 weeks, the patient experienced partial hair regrowth and his AD improved. After 3 months, hair regrowth was complete.
Fig. 1. Patient’s scalp. (a) Baseline; (b) 8 weeks after starting dupilumab; (c) tufts of hair held together by conglomerated scales or casts; (d) 12 weeks after starting dupilumab, diffuse hair loss on a background of erythema and scaling.
To the best of our knowledge, 13 patients who developed abrupt shedding of hair following treatment with dupilumab have been reported in literature (2–12) to date. They include 2 different patterns of alopecia: classic AA (2–8) and AA-like hair loss associated with erythema and scaling (10–14). Table SI shows the main characteristics of these patients.
Classic AA was reported in 8 patients (5 men and 3 women, 20–51-year age range). The diagnosis was based on both clinical and dermatoscopic features in one patient (5) and on clinical features only in 7 (2–4, 6–8). None of the patients was biopsied. A history of previous AA was present in 2 patients (3, 4), absent in 4 (2, 7, 8), and not reported in 2 (5, 6). All of the patients had severe atopic dermatitis that markedly improved with dupilumab. The time lapse between starting dupilumab and the onset of AA ranged between 2 days and 28 months. Dupilumab was discontinued in 2 patients (3, 7) and continued in 5 (3–6, 8). In one case, the authors do not report whether the drug was continued (4). All patients experienced hair regrowth within 3 weeks to 6 months.
AA-like reactions, characterized by abrupt shedding of hair, associated with erythema and scaling, as in the current case, were reported in 5 patients (5 men, 27–33 years) who were affected by severe AD that greatly improved on dupilumab. A personal or family history of AA was absent in 4 (8–10, 12) and unknown in one patient (11). In 4 out of 5 patients, histology was performed, showing psoriasiform epidermal features and alopecia areata-like dermal changes (Table SI). Alopecia developed within 5–7 weeks of starting dupilumab in 3 patients (9, 10, 12), and within 18–40 weeks in 2 patients (8–11). Dupilumab was withdrawn in 2 patients and continued in 3 patients. Hair regrowth of different degrees was reported in 4 patients (8, 9, 11, 12).
Although it cannot be proven on histological grounds, the clinical characteristics and timing of the alopecia in the current patient are highly suggestive of a psoriatic-like reaction induced by dupilumab. His alopecia developed shortly after starting the drug, was not responsive to potent topical steroids, and resolved after discontinuation of dupilumab and the reintroduction of cyclosporine. It is noteworthy that a transient body dermatitis resembling inverse psoriasis had preceded his alopecia.
IL-4 is a known negative regulator of Th1- and Th17-mediated inflammation. It has been suggested that its blockade by dupilumab may create a Th2/Th1 imbalance and enhance or promote Th1/Th17. This imbalance may increase expression of interferon-gamma (13) causing skin manifestations, such as psoriasis (14), psoriatic alopecia (15) and paradoxical psoriasiform reactions (16). Moreover, expression of IL4 and IL13 is correlated with the development of sebaceous glands, and it has been suggested that alterations in the expression of these factors may cause sebaceous gland atrophy (17). Our case seems to confirm this hypothesis. Some AA-like reactions occurring during treatment with dupilumab (17) may, in fact, be forms of psoriatic alopecia, i.e. an uncommon entity that has also been reported as a possible side-effect of anti-tumour necrosis factor-α therapy (18).


 Click to show fullsize
Click to show fullsize