


1Dermatology Outpatient Office Dr Daniela Kasche, Hamburg, 2Dermatology Outpatient Office Dr Uwe Kirschner, Mainz, Germany, and 3Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chalubinskiego 1, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Accepted Jun 4, 2020; Epub ahead of print Jun 9, 2020
Acta Derm Venereol 2020; 100: adv00193
Hidradenitis suppurativa (HS) is a chronic, inflammatory skin disease characterized by nodular inflammation, abscesses, fistulas and pus discharge, mainly located in the intertriginous areas of the skin (1). Considerably reduced quality of life (QoL) in patients with HS has been well documented (2). In recent years, new medical treatment modalities for HS have emerged (3). However, the guidelines and the treatment algorithms highlight the necessity for surgical interventions, especially in patients with Hurley stages II and III HS (4). The Mandatory Surgical Indications According to Bechara for Hidradenitis Suppurativa Surgery (MIBHS) has been presented recently. MIBHS include fistulas/sinus tracts, accordion-like scars, contracted scars, mutilating HS and suspected malignancy (5). However, patients are often reluctant to undergo surgery.
In 2017, LAight® therapy (LENICURA, Wiesbaden, Germany), a non-invasive, device-based treatment utilizing a combination of intense pulsed light (IPL) and radiofrequency (RF), was approved throughout the European Union (EU) for all severities of HS (https://www.lenicura.com/laight-therapy). LAight® therapy comprises 3 treatment passes differing with respect to applied IPL pulses. Detailed technical data are shown in Table I (6). The treatment is beneficial for patients, with improvements in skin lesions and QoL (6). We report here 2 additional patients with HS who declined surgical procedures, but improved markedly with LAight® therapy.
Table I. Technical characteristics of LAight® therapy (6)
Case 1. A 39-year-old Caucasian woman presented with Hurley stage II disease with lesions located on both axillae, the groins and the buttocks (Fig. 1A). The patient had previously undergone several incisions, drainage procedures and 2 additional excisions with primary closures. These resulted in temporary improvement; however, they recurred after a few years.
On admission, the patient’s QoL was substantially impaired (Dermatology Life Quality Index (DLQI) score 17 points) and the pain intensity, evaluated on an 11-point numeral rating scale (NRS), was 6 points.
Taking all the above into consideration, the patient underwent LAight® monotherapy every second week. After 10 treatments, her condition had improved considerably, especially the inflammation, which reduced significantly. The DLQI score decreased to 4 points; however, the intensity of pain remained at a similar level (NRS 5 points). The patient continued the therapy, and after 24 additional consecutive sessions the inflammatory lesions were almost eliminated. DLQI was assessed as 2 points, and the pain level decreased to 3 points. The scarring process remained unchanged. However, the patient reported softening of the scars (Fig. 1B).
Fig. 1. Case 1: (A) female patient’s axillary area on admission. (B) Axillary area after 34 treatment sessions.
Case 2. A 32-year-old Caucasian man presented with Hurley stage II HS with lesions in both axillae, the suprapubic area and the buttocks. He had previously undergone numerous incisions, drainage procedures and simultaneous excisions of 30 cm2 from each axilla. However, the disease progressed (Fig. 2A). The patient declined further surgical interventions. On admission, the patient’s DLQI was 6 points and he assessed his pain intensity with the NRS as 6 points.
The patient began LAight® therapy on a regime of every second week. After 10 treatment sessions, his inflammation and scar texture improved. This resulted in a marked improvement of the patient’s QoL. The DLQI score decreased to the level of 1 point, indicating normal QoL. In addition, the pain intensity reduced to 3 points. After a total of 34 treatment sessions, this therapy resulted in almost complete reduction of inflammation, and pain (NRS=0 points), and marked softening of the scars (in the patient’s opinion) (Fig. 2B). At this time, the patient’s DLQI was 1 point.
Fig. 2. Case 2: (A) male patient’s axillary area on admission. (B) Axillary area after 34 treatment sessions.
Standard treatment options for HS involve both the conservative and the surgical approach (7). Surgery is considered the only effective treatment option, as conservative therapy does not cure irreversible skin tissue damage caused by HS (4, 5). Based on our experience and available literature data, many patients decline radical surgical interventions (8). We believe that a non-invasive approach (e.g. LAight® therapy) could be a promising alternative for this group of HS patients.
Previously it was indicated that mono-therapy with IPL reduced inflammation in patients with HS (9). Moreover, it is also known that RF may stimulate collagen remodelling, leading to improvement in the texture of the scars (10, 11). It was suggested that IPL blue light has anti-inflammatory properties via reduction of IL-1a and ICMA-1 (2). Furthermore, superficial desquamation of the epidermis might reduce hair follicle blockage, which is one of the major initial causes of development of HS (2). A positive effect on HS might also be that RF mediates liquefaction of enclosed lipids, releasing blockage of the hair follicles (4). In addition, a synergetic effect of the 2 components was supported by Seok et al. (12), who analysed the effect of RF and IPL in an acne-induced rabbit ear model. In combination, the 2 had an additive effect in treatment (5).
This has been confirmed recently by the study by Wilden et al. (6) dealing with 47 subjects with HS. They showed that combined IPL+RF treatment (LAight®) was superior to the monotherapy of both IPL and RF. After 12 weeks of therapy, they reported a 10% reduction in count of active lesions among patients treated with IPL+RF, compared with a 5% reduction with RF, and 6% increase with IPL monotherapies. The effectiveness of the combined therapy was more prominent for patients with Hurley I/II stage compared with Hurley III stage, resulting in reductions in the number of active lesions of 32% and 2%, respectively (6).The analysis of DLQI score reduction (between week 0 and week 12) in the 3 different treatment arms revealed that the decrease in DLQI was much less pronounced in the IPL group (mean change –1.3 points) compared with the RF+IPL and RF patient groups (mean –5.1 and –6.6; respectively), which achieved the level of minimal clinically important difference (MCID) (13). The MCID (reduction of at least 4 points) in DLQI scores (14) was also achieved in both of the current patients. We found a 15-point reduction in the first subject and a 5-point reduction in the second. A similar effect was obtained for pain assessed with NRS. Both of the patients reported a substantial decrease in pain intensity (3 points), indicating achievement of MCID for reduction in NRS pain intensity (15).
In conclusion, LAight® therapy could be beneficial for patients with HS, especially those who are reluctant to undergo surgical procedures. It is well tolerated; no adverse effects were observed. LAight® therapy can be used as monotherapy, but it might also be combined with both topical and/or systemic agents. Particular attention should be paid to the combination of LAight® therapy with resorcinol, as Theut Riis et al. (16) reported an increased risk of adverse events after treatment with a combination of IPL and resorcinol. Moreover, it is also clear that systemic tetracycline should be used with caution with any light treatment (16). Further research studies are required into the combined therapies.


 Click to show fullsize
Click to show fullsize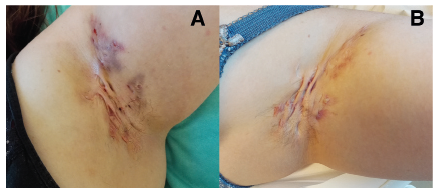 Click to show fullsize
Click to show fullsize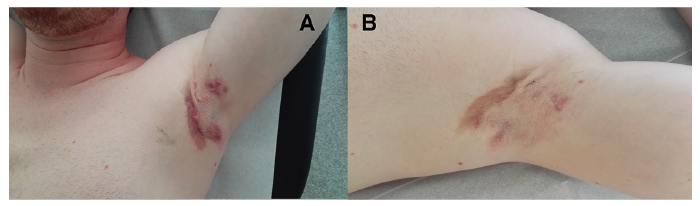 Click to show fullsize
Click to show fullsize