


1Department of Dermatology and Venereology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg and 2Department of Dermatology and Venereology, Region Västra Götaland, Sahlgrenska University Hospital, Gothenburg, Sweden
Facial high-risk basal cell carcinomas are preferably treated with Mohs micrographic surgery, but only 10% of patients are offered Mohs micrographic surgery in Sweden. The aim of this retrospective study was to examine the differences between primary and recurrent or incompletely excised facial high-risk basal cell carcinomas undergoing Mohs micrographic surgery, with regard to the number of stages, final defect sizes, reconstructive techniques and other consequences. The study was performed during the period 2012 to 2019 at our centre. A total of 903 basal cell carcinomas in 813 patients (70.1% primary, 10.4% incompletely excised and 19.5% recurrences) were included. The mean number of Mohs micrographic surgery stages was significantly lower for primary basal cell carcinomas compared with recurrences (p = 0.03), and the mean final defect size was significantly smaller in primary basal cell carcinomas compared with both recurrent (p < 0.0001) and incompletely excised (p = 0.003) tumours. Primary basal cell carcinomas tended to more often be reconstructed by primary closure (p = 0.08). Mohs micrographic surgery indications for facial high-risk basal cell carcinomas should be respected and used more frequently on primary basal cell carcinomas, in order to enable better utilization of resources and improved outcomes for the patient.
Key words: basal cell carcinoma; non-melanoma skin cancer; Mohs micrographic surgery; recurrence; incomplete excision.
Accepted Nov 16, 2020; Epub ahead of print Nov 18, 2020
Acta Derm Venereol 2021; 101: adv00381.
doi: 10.2340/00015555-3698
Corr: Hannah Ceder, Department of Dermatology and Venereology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, SE-413 45 Gothenburg, Sweden. E-mail: hannah.ceder@vgregion.se
In most European countries, Mohs micrographic surgery is underused and is often reserved for patients with facial high-risk basal cell carcinomas in which previous treatments have failed. This study shows that following international guidelines and using Mohs micrographic surgery as indicated when deciding on the primary management of high-risk facial basal cell carcinomas would probably increase the number of less complex procedures, i.e. fewer stages, smaller defects and a higher probability of primary closures.
Basal cell carcinoma (BCC) is the most common form of skin cancer, and its incidence is increasing (1). The risk of recurrence after treatment depends on the size of the tumour, the aggressiveness of the histopathological subtype, and its localization (2–4). Metastasis and death are extremely rare, but BCCs can cause significant morbidity due to aggressive and destructive local growth (5, 6). Given the large number of tumours that occur, costs to society are high (7).
Internationally, BCCs are classified into 2 broad categories on the basis of histopathological features: low-risk and high-risk subtypes. Low-risk subtypes include nodular and superficial BCCs. High-risk subtypes, which tend to cause extensive local destruction and have a higher recurrence rate, include infiltrative, micronodular, morpheaform, and basosquamous tumours (2, 3, 8–11). However, Swedish pathologists historically classify BCCs according to the “Sabbatsberg model”, which includes 3 risk categories: (i) “low-risk” nodular and superficial subtypes; (ii) “medium-risk” less aggressive infiltrative subtypes; and (iii) “high-risk” more aggressive infiltrative and morpheaform subtypes (9).
Surgical excision (SE) is generally considered the treatment of choice for BCCs (12–14). Facial high-risk BCCs, especially on or in close proximity to the nose, lips, ears, eyelids and eyebrows, are preferably treated with Mohs micrographic surgery (MMS), which allows for complete examination of all tissue margins guaranteeing complete removal, and minimizing the risk of recurrence, while sparing as much healthy tissue as possible (5, 15, 16). However, only slightly more than 300 MMS procedures are performed each year in 3 Swedish cities (Gothenburg, Lund and Stockholm) despite approximately 3,000 high-risk (according to the Swedish classification) facial BCCs being diagnosed each year (8, 17, 18). Resource shortage, low accessibility, long waiting times, and poor knowledge about the technique seem to be the main reasons for the low number of MMS procedures (19, 20).
Studies have shown that 25–31% of high-risk BCCs are incompletely excised using regular SE (21, 22). The recurrence risk is also greater after SE compared with MMS (19, 20, 23). Furthermore, failed treatments resulting in incompletely excised BCC (IE-BCC) or recurrent BCC (R-BCC) increase the healthcare costs and worsen outcomes for patients (24, 25). According to the principle that the first treatment should be the final treatment, using MMS to treat high-risk primary BCC (P-BCC) may be better than using MMS as rescue therapy following previously failed treatments.
The primary objective of this study was to measure differences in the number of stages and the final defect sizes following MMS when used for P-BCC, IE-BCC and R-BCC, respectively. The secondary objective was to analyse other consequences of not offering MMS in the first place, such as the complexity of the required reconstructive techniques.
The study was conducted at the Department of Dermatology, Sahlgrenska University Hospital, Gothenburg, Sweden. All consecutive patients who had undergone MMS for BCC at our department between 2012 and 2019 were retrospectively analysed. The study was approved by the Swedish Ethical Review Authority. Patients were excluded if they were treated for any other diagnosis, if the BCC was a recurrence after MMS, or if data were missing regarding the number of stages, final defect size or any previous treatment prior to MMS. A detailed description of the traditional MMS technique on fresh frozen tissue used at our department has been published previously (19).
Data regarding the following demographic, clinical and surgical parameters were collected: patient age and sex, date of diagnosis, date of surgery, tumour location and diameter, histopathological subtype, previous treatments, physician specialty treating the tumour prior to MMS, physician specialty referring for MMS, number of MMS stages, the largest and smallest diameter of the final defect, as well as the reconstructive technique. Surgical defect areas were calculated using the formula: area=Π×(major axis/2)×(minor axis/2).
All data were analysed using “R” version 3.0.3 (The R Foundation for Statistical Computing, Vienna, Austria). Kruskal–Wallis tests were used to compare 3 or more groups. To compare 2 groups, Wilcoxon rank sum test was used. Fisher’s exact test was used to compare proportions between groups. p-values < 0.05 were considered significant and tests were 2-sided. Based on previous data, in which IE-BCCs were not recognized as a different category (20), a power calculation was performed estimating P-BCCs relative to R-BCCs undergoing MMS during the study period at the current ratio of 3.75:1. To achieve 80% power with an α-error of 0.05, 656 P-BCCs and 175 R-BCCs were needed regarding differences in number of stages, while 480 P-BCCs and 128 R-BCCs were required regarding differences in the final defect size.
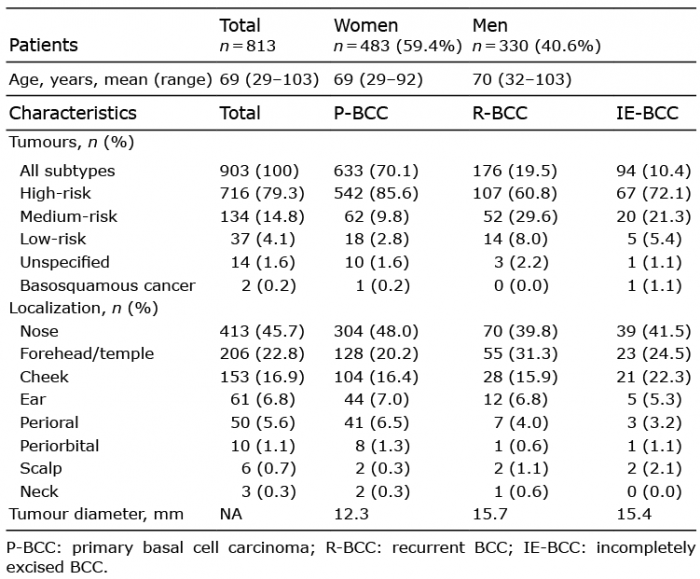
During the study period, MMS was performed on a total of 913 tumours in 817 patients. Nine tumours were excluded for being recurrences after previous MMS and one squamous cell carcinoma was also excluded. Thus, a total of 903 tumours in 813 patients were included (Table I). There were 71 patients who were treated with MMS for more than one tumour. Of the 813 patients, the majority were women, 59% (n = 483). Of the 903 tumours, 70.1% (n = 633) were P-BCCs, 10.4% (n = 94) were IE-BCCs, and 19.5% (n = 176) R-BCCs.
Table I. Demographic data and characteristics of the tumours at time of Mohs micrographic surgery
The mean number of stages among all tumours was 1.93 (95% confidence interval (95% CI) 1.87–1.98) with a maximum of 10 stages. The mean number of stages differed significantly between P-BCCs, IE-BCCs and R-BCCs (p = 0.013) (Fig. 1). R-BCCs required significantly more stages (2.11; 95% CI 1.96–2.27) than P-BCCs (1.89; 95% CI 1.84–1.94; p = 0.03) and IE-BCCs (1.82; 95% CI 1.64–2.00; p = 0.007). There were no significant differences in the number of stages between P-BCCs and IE-BCCs (p = 0.09).
Fig. 1. Number of Mohs micrographic surgery stages (mean, 95% confidence interval (95% CI)) for primary basal cell carcinoma (P-BCC), incompletely excised BCC (IE-BCC) and recurrent BCC (R-BCC).
The mean area of the final defects among all tumours was 4.26 cm2 (95% CI 3.91–4.60 cm2). The mean area differed significantly between P-BCCs, IE-BCCs and R-BCCs (p < 0.0001) (Fig. 2). The final defect areas were significantly smaller in P-BCCs (3.55 cm2; 95% CI 3.27–3.83 cm2) than in IE-BCCs (5.10 cm2; 95% CI 3.98–6.21 cm2; p = 0.003) and R-BCCs (6.34 cm2; 95% CI 5.07–7.60 cm2; p < 0.0001) There was no significant difference in the final defect size between IE-BCCs and R-BCCs (p = 0.54). When comparing R-BCCs and IE-BCCs with P-BCCs, respectively, regarding the difference between the maximum diameter of the defect size after MMS and the clinically measured maximum diameter of BCCs before MMS, the difference was also significantly greater for R-BCCs (13.4 vs 9.6 mm, p < 0.001) and IE-BCCs (12.0 vs 9.6 mm, p = 0.015).
Fig. 2. Final defect size in cm2 (mean, 95% confidence interval) for primary basal cell carcinoma (P-BCC), incompletely excised BCC (IE-BCC) and recurrent BCC (R-BCC).
As shown in Table II, the most common reconstructive technique for all tumours was primary closure, which was used in over half of cases, followed by various types of flaps and then grafts. A smaller proportion of defects were left to heal by secondary intention or required combinations of different techniques. Only one patient needed to be referred to a plastic surgeon for reconstruction. Primary closures were used more often among P-BCCs compared with IE-BCCs and R-BCCs, but the difference was not significant (p = 0.08).
Table II. Reconstruction methods used after Mohs micrographic surgery for primary basal cell carcinoma (P-BCC), recurrent BCC (R-BCC) and incomplete excised BCC (IE-BCC)
Overall, the median waiting time from diagnosis to final curative treatment with MMS was 7.5 months (range 0–352.9 months). The median waiting time was 6.4 months (0–46.9 months) for P-BCCs, 9.4 months (2.3–214.9 months) for IE-BCCs and 38.8 months (3.2–352.9 months) for R-BCCs.
Of all included tumours, 94.0% were referred for MMS by a dermatologist. In cases of P-BCC and R-BCC, MMS was suggested by a dermatologist in over 90% of cases. In the IE-BCC group, otorhinolaryngologists and plastic surgeons accounted for approximately one-third of referrals for MMS (Table III).
Table III. Physician specialty referring for Mohs micrographic surgery
Among all R-BCCs, 77.8% had been treated with one method previously, 27.2% had been treated with 2 different methods previously, and 1.1% had undergone 3 different treatment methods prior to MMS. Each R-BCC was treated unsuccessfully a mean of 1.8 times (1–6 treatments regardless of method) before finally undergoing MMS. In cases in which the treating physician’s specialty was known (265 of 314 treatments), 65.4% of the unsuccessful treatments had been performed by dermatologists, 19.9% by otorhinolaryngologists, 8.6% by plastic surgeons, 4.5% by general practitioners and 1.1% by general surgeons. The most common previously unsuccessful treatments were SE (58.3%) and cryotherapy with or without curettage (29.9%).
IE-BCCs had undergone failed SE a mean of 1.5 times (range 1–6 times) before MMS was performed. In 43.6% of these cases, SE had been performed by dermatologists, in 29.8% by otorhinolaryngologists, in 10.6% by plastic surgeons, and in 6.4% by general practitioners. In the remaining 7.5% of cases, more than one specialty had been involved.
This study indicates that P-BCCs require significantly fewer MMS stages compared with R-BCCs, but not compared with IE-BCCs. Furthermore, P-BCCs lead to significantly smaller final defect sizes than both IE-BCCs and R-BCCs. For all tumours, the most common reconstructive technique was primary closure, the second most common were flaps and the third most common was grafts. Although no significant difference was shown, defects from P-BCCs treated with MMS were more often reconstructed using primary closure compared with those from both IE-BCCs and R-BCCs. Unsurprisingly, curative treatment with MMS was significantly delayed for patients with both IE-BCCs and, especially, R-BCCs. The decision to perform MMS was usually taken by dermatologists and SE was the most common previously failed treatment for both IE-BCCs and R-BCCs.
A few previous studies have shown similar results, with P-BCCs requiring significantly fewer MMS stages to be completely excised (20, 26, 27). Our group showed that P-BCCs require 0.2 fewer stages than R-BCCs, but in that study IE-BCCs were not considered as a separate group (20). Leibovitch et al. (26) as well as Santos-Arroyo et al. (27) also showed that P-BCCs required significantly fewer stages than R-BCCs (0.23 and 0.61 fewer stages, respectively) to be completely excised. However, Santos-Arroyo et al. (28) also included squamous cell carcinomas, which may have caused a slightly larger difference. The difference in the number of MMS stages found in this study was similarly small (0.22 stages per procedure) but statistically significant, and could save one stage for every 5 R-BCCs if they had been primarily treated with MMS instead.
Regarding the final defect size, 2 of the above-mentioned studies also showed similar results, with final defect sizes being significantly smaller for P-BCCs (20, 26). A previous study by our group showed that the final median area of P-BCC defects was 1.03 cm2 smaller than defects after MMS for R-BCCs (20). Leibovitch et al. showed that 51.6% of P-BCCs resulted in a defect size < 2 cm in diameter, whereas the corresponding percentage for R-BCCs was 29.5%, which was a significant difference. When looking at defect sizes in diameter in our study for comparison (data not shown), similar results were observed with 48.0% of all P-BCCs compared with 30.1% of all R-BCCs resulting in a defect size < 2 cm in diameter.
We also noticed a trend towards P-BCC defects being able to be closed primarily more often compared with R-BCC defects. Primary closure is considered to be a simple, fast and reliable method with fewer complications (28–30). There are no studies supporting that primary closures are less time-consuming, but this is well-accepted among physicians. Thus, an increased use of primary closures when using MMS more often for P-BCCs could theoretically save time and lower the risks of postoperative complications.
The median waiting time to MMS of over 6 months for P-BCCs at our centre could be considered a long time, but much indicates that any given BCC would not be able to grow significantly during that period. There are few studies on the growth rate of BCC (31, 32), but they are slow-growing tumours (31, 33) and it can take years for BCCs to double in size (32). Thus, a waiting time of 6 months should have little effect on the size of the tumour and should not be a reason not to refer for MMS when it is indicated. However, BCCs may grow more substantially over a period of 3 years, the median waiting time for R-BCCs in this study. Scar tissue in the areas of previous unsuccessful treatments can also make it difficult to demarcate IE-BCCs and R-BCCs, which may explain why more MMS stages are required for complete removal of R-BCCs, and also result in larger final defect sizes for both IE-BCCs and R-BCCs.
When analysing the differences between the size of the lesion before MMS and the final defect size, the mean difference of 9.6 mm for P-BCCs would theoretically indicate that a mean of 4.8-mm margins on either side of the lesion would be required to achieve complete removal. Meanwhile, the 13.4-mm and 12.0-mm differences in R-BCCs and IE-BCCs, respectively, would translate into a need of approximately 6.7-mm and 6.0-mm mean margins around the tumour. This would also explain why standard margins of 5 mm for high-risk P-BCCs and R-BCCs are so often incompletely excised with SE (21, 22).
Although it is not clear why BCCs that fulfil the indications for MMS do not always receive this treatment immediately, this study shows that both dermatologists and physicians within several other specialties were responsible for the failed treatments that gave rise to the R-BCCs and IE-BCCs, which, in the end, required MMS. It is possible that many physicians are unable to recognize high-risk BCCs clinically, have insufficient knowledge about MMS and its indications or believe that 6 months is too long to wait for MMS, and instead hurry unnecessarily to treat the tumour with an inferior method. Furthermore, preoperative biopsies do not always show the true BCC subtype (34–36). Thus, studies focusing on improved preoperative diagnosis with dermoscopy or other imaging techniques and clearer indications for preoperative biopsies are required.
Historically, Sweden and many other European countries have regarded MMS to be a rescue method, making it more difficult and sometimes impossible to implement MMS at more centres. R-BCCs in themselves constitute a predisposing factor for MMS to require 4 or more stages more often (37). Also, recurrence rates after MMS are greater for R-BCC, making it less useful (23, 38–40). At our department, the proportion of P-BCCs undergoing MMS has increased from 56% to 70.1% of all surgeries compared with the previously studied time period of 1993 to 2003, which allows us to perform twice as many MMS procedures per day. The mean number of stages per tumour has decreased from 2.4 to 1.9, the median area of the final defect sizes has decreased from 3.9 to 2.7 cm2, while the proportion of primarily closed defects after MMS has increased from 16.2% to 51.0% of all cases.
Strengths and limitations
The main strength of this study is that data were available for all consecutive cases from the local register of all MMS procedures carried out at our department. The main limitations are the facts that this is a single-centre study, that it is non-randomized and the retrospective nature of the study. Also, scars from previous treatments may have affected the measurements in R-BCC and IE-BCC when estimating the size of the lesion before MMS.
Conclusion
Carrying out MMS more frequently on P-BCCs rather than using it as a rescue method for IE-BCCs and R-BCCs allows for better resource utilization and leads to improved outcomes for the patient. In order to reduce the number of failed treatments, all physicians managing patients with BCCs should have good knowledge about the indications and benefits of MMS. Better diagnostic techniques are also needed to preoperatively recognize high-risk tumours in order to increase the probability of the first treatment being the final one.
The authors thank statistician Martin Gillstedt for his help with the data analysis.
This study was supported by grants from the Anna-Lisa and Bror Björnsson’s Foundation and from the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement (ALFGBG-728261).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize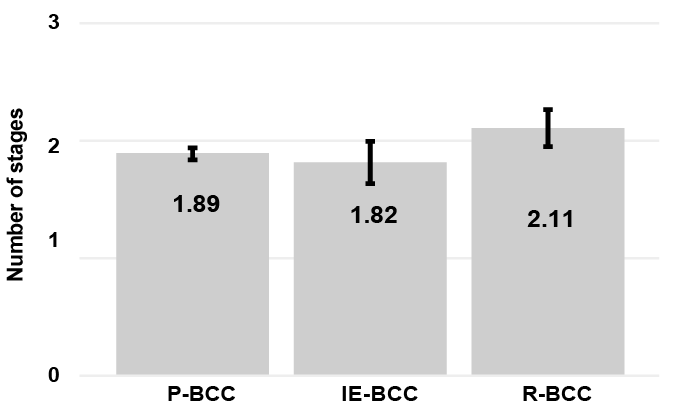 Click to show fullsize
Click to show fullsize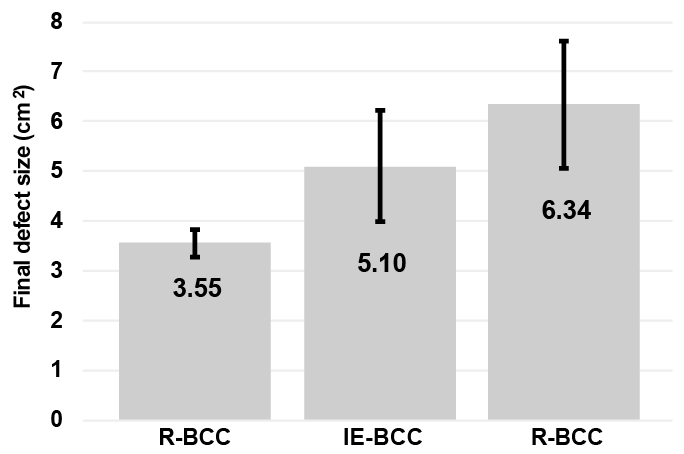 Click to show fullsize
Click to show fullsize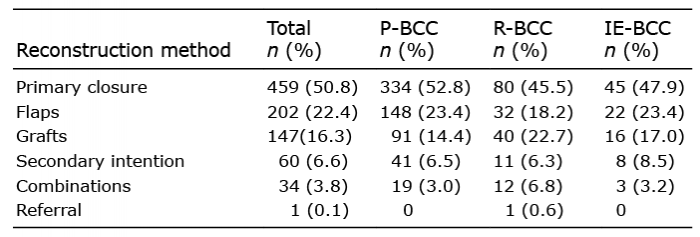 Click to show fullsize
Click to show fullsize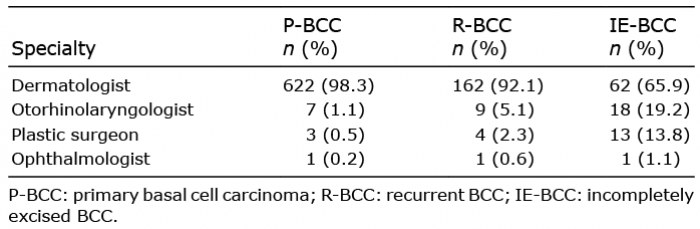 Click to show fullsize
Click to show fullsize