


1Centre for Dermatology Research, The University of Manchester & Salford Royal NHS Foundation Trust, 2NIHR Manchester Biomedical Research Centre, Manchester University NHS Foundation Trust, and 3Centre for Biostatistics, The University of Manchester, Manchester Academic Health Science Centre, Manchester, U.K. E-mail: abigail.langton@manchester.ac.uk
#These authors contributed equally to this work and should be considered as first authors.
Accepted Nov 19, 2020; Epub ahead of print Nov 26, 2020
Acta Derm Venereol 2020; 100: adv00347.
doi: 10.2340/00015555-3708
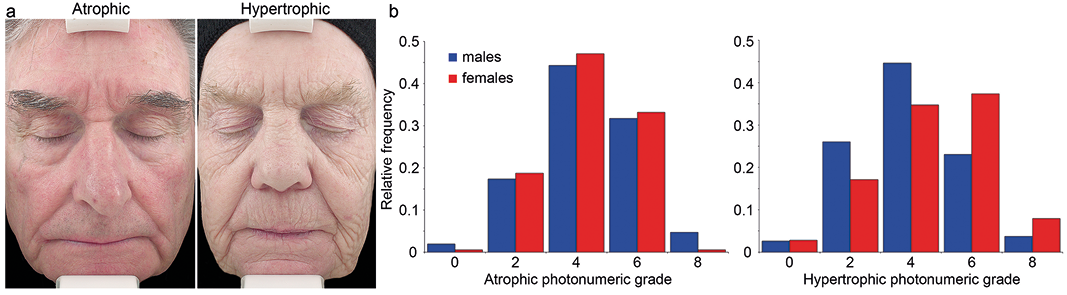
Chronic exposure to solar ultraviolet radiation (UVR), a process known as photoageing, leads to characteristic but complex changes in the skin. Amongst fair-skinned individuals of Northern European descent there is a well-documented polarity in the clinical appearance of photoaged skin, termed hypertrophic (HP) and atrophic (AP) photoageing (1-4). People with HP present clinically with deep, coarse wrinkles and a leathery texture whereas those with AP have minimally wrinkled, translucent facial skin with pronounced telangiectasia and an increased frequency of keratinocyte cancers (Fig. 1a) (2, 4, 5). In addition to these clinical differences, there is evidence that HP and AP may have distinct histological features; the quantity of elastotic material (solar elastosis) in HP facial skin is significantly greater than in AP facial skin (5). To date, these distinct facial photoageing phenotypes have been described in cohorts recruited from dermatology outpatient departments in both the United States of America (5) and the United Kingdom (UK) (1). In the current study we assessed the prevalence of HP and AP in the general population of Greater Manchester (UK).
Fig. 1. Assessment of gender and photoageing severity for atrophic and hypertrophic phenotypes. (a) An 84-year-old man with atrophic photoageing demonstrates paucity of coarse wrinkles and presence of telangiectasia. A 72-year-old woman with hypertrophic photoageing demonstrates characteristic deep, coarse wrinkling of the cheek and minimal to absent erythema. (b) Photonumeric scales were used to assess the degree of photoageing for each participant. Each photonumeric scale ranged from 0–8, where 0 represents absence of the form of photoageing and 8 indicates severe photoageing (atrophic or hypertrophic). The relative frequency of atrophic photoageing severity was not different between males and females; whereas in hypertrophic photoageing, females had a more severe phenotype than males (b).
This observational study was conducted following local ethical approval from The University of Manchester Research Ethics Committee (Ref: 2019-7329-10778). Observational visits were made, by appointment, to golf clubs and garden centres across Greater Manchester during July and August 2019. Observations were made by a single assessor (ZA) without direct interaction or interview of study participants. Study subjects were deemed eligible for observation if their perceived age was over 50 years old and they were of white Northern European ancestry (Fitzpatrick phototypes I-III). For each eligible individual the following observations were made: estimated age range, i.e. from observation only (50-59 years; 60-69 years or 70+ years), sex and photoageing phenotype (HP or AP). The clinical severity of HP and AP were assessed using validated nine-point photonumeric scales (1, 3) where a grade of 0 represented no photoageing and a grade of 8 represented the most severe form of photoageing.
During the study period, observations were made on 1,571 individuals (males, 777; females, 794). The prevalence of AP was highest amongst males (AP: 508 (65.4%); HP: 269 (34.6%)); whereas the converse was true for females, with HP predominating (AP: 187 (23.6%); HP: 607 (76.4%)).
The relationship between sex and the clinical severity of skin photoageing phenotype was investigated (Fig. 1b) using a series of regression models. Severity of skin photoageing was treated as ordinal (higher values depict more severe ageing, but the data values were treated as categories with unknown distances between them) and ordered regression modelling employed. Age-group was initially included as a covariate, but subsequently removed as it was possible that participants’ ages were estimated according to their skin morphology, thus creating a ‘circular path’ between age and severity; that is, does age ‘predict’ skin severity or does skin severity ‘determine’ a participant’s perceived age (given that it was not directly ascertained – see Materials and Methods). Initially, sex and phenotype were treated as main-effects only, but an interaction between them was also investigated. Model output, parameter estimates and their 95% confidence interval are shown in Table I. When included in the model (see Table I, models 1 and 3), age is the dominant covariate. Older participants display significantly more severely aged skin (p < 0.001 in both models). When age is removed from the model, the pseudo R2 falls dramatically, indicating, approximately, that less variation in the outcome is being accounted for.
Table I. Regression models of gender and the clinical severity of skin photoageing phenotype
The main effect of sex is also significant (models 1 and 2), whether (p = 0.013) or not (p = 0.001) age is controlled for: HP males had significantly less severely photoaged skin than HP female participants. There was no difference between AP and HP skin types, including (p = 0.997) or excluding (p = 0.435) age in the main effects-only models. Further modelling included a sex-by-phenotype interaction, which was highly significant (p < 0.001) in both cases. This implies that the effect of phenotype (AP vs. HP) on skin photoageing severity differs significantly between men and women.
This prevalence study has confirmed the existence of two phenotypes of facial photoageing in a sample of the general population in Northern England. Furthermore, both AP and HP phenotypes show sex polarity, with AP prevalence highest amongst males and HP prevalence highest amongst females. Interestingly, when it occurred, the severity of AP was comparable between males and females, whereas in HP, females have a significantly more severe phenotype than do males.
The lesser prevalence and severity of HP amongst males is particularly interesting as it would be expected that men generally have a different behaviour pattern with respect to sun exposure compared to females. Men tend to undertake more outdoor work and enjoy more outdoor recreational hobbies; furthermore there is their notable reluctance to use sunscreen (6). It is therefore unlikely that development of a particular skin photoageing phenotype is a direct result of the degree of sun exposure experienced by the individual. One possibility for the dichotomy in phenotype between males and females is the presence of more skin appendages, such as hair follicles, sweat glands, sebaceous glands and blood vessels in male facial skin compared to the facial skin of females (7–9). The increased presence of sebaceous glands and sweat glands in male perioral skin has been described in association with decreased perioral wrinkle formation (7) and hypothesized that better vascularization of the skin may have a decelerating effect on wrinkle development (7). In addition to differences in the abundance of skin appendage, changes to hormonal status caused by the menopause are known to profoundly affect skin function (10).
Our study is limited to data from one city region in the North of England and, as it is purely observational, we were unable to ascertain information such as menopause status or lifestyle factors (for example diet, smoking, sunscreen use), which would have been valuable additions to the data as these all impact skin ageing (11, 12). Age is difficult to estimate accurately, particularly as it is possible that perceived age is higher for those individuals that have the more severe HP and less for those with AP. For this reason, individuals were placed into estimated age ranges (50–59 years, 60–69 years and 70+ years) and regression modelling performed with age both included and excluded as a covariate. Our use of a single assessor (ZA) was intended to mitigate any variability in the observations; however, we accept that having a single assessor could also be perceived as a limitation as there was no validation by a second observer. Our data collection sites of golf clubs and garden centres were selected as they are public places popular with many older citizens; however, this could potentially introduce bias towards people who favour outdoor activities. Despite these limitations, we believe our successful execution of this study methodology in Greater Manchester can be used as a template for future research exploring the relationship between facial photoageing phenotype, sex and keratinocyte cancer risk in other geographic locations across the UK.
The incidence of facial keratinocyte cancers has been previously shown to be significantly greater in those individuals with AP (2, 5); our study further highlights the importance of educating clinicians about recognising these distinct phenotypes of facial photoageing. Whilst everyone should follow basic sun safety rules, it is clear that individuals with AP should be even more vigilant in avoiding excessive sun exposure, applying sunscreen regularly, and routinely checking their skin for pre-malignant changes.
This study was funded by a programme grant from Walgreens Boots Alliance.
Whilst supported in part by a programme grant from industry, funders had no editorial control over this manuscript.
CEMG is a National Institute for Health Research (NIHR) Emeritus Senior Investigator. CEMG and REBW are supported in part by the NIHR Manchester Biomedical Research Centre.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize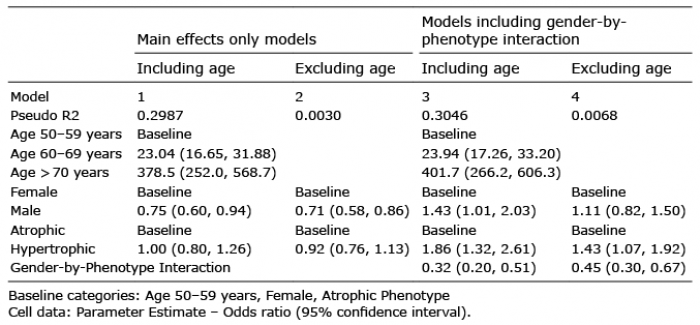 Click to show fullsize
Click to show fullsize