


1Department of Dermatology, Graduate School of Medicine, University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655 and 2Koenji-Ekimae Dermatology Clinic, Tokyo, Japan. E-mail: yasano-tky@umin.ac.jp
Accepted Nov 27, 2020; Epub ahead of print Dec 7, 2020
Acta Derm Venereol 2020; 100: adv00348.
doi: 10.2340/00015555-3713
Argyria is a rare skin disease characterized by blue-grey discolouration due to chronic exposure to silver-containing products. As the discolouration associated with silver deposition is permanent, patients generally experience long-term cosmetic problems. Treatment options for argyria and their efficacy are limited, but there is increasing evidence proving that laser therapy is effective for this skin condition (1, 2). We describe here a case of generalized argyria that was treated successfully with Q-switched alexandrite laser.
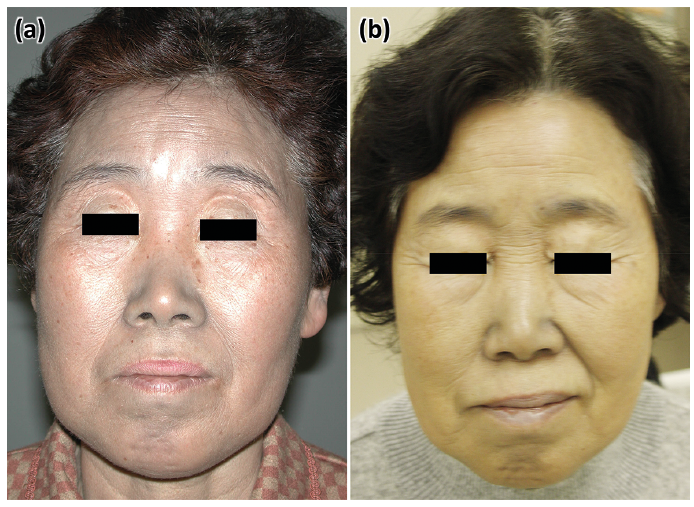
A 62-year-old Japanese woman presented to our hospital with a 10-year history of a blue-grey skin discolouration, especially on her face (Fig. 1a), which initially started on her nose, and gradually expanded to her face, neck and whole body (Fig. S1a). Her fingernails showed a bluish discolouration extending from the lunula to the middle of the nail plate (Fig. S1b). No colour change was observed in mucus membranes. She was frequently subjected to chemical cauterization with silver nitrate for chronic tonsillitis in her childhood, while she had never been administered colloidal silver ingestion or amiodarone. She had worked as a solderer for approximately 20 years, possibly exposed to lead. Skin biopsy from her neck revealed fine depositions in the dermis and hair follicles and around the basement membrane of eccrine sweat glands (Fig. S2a–c). Electron microscopy revealed that deposits distributed throughout the dermis, especially on the elastic fibres, were approximately 100–200-nm in diameter (Fig. S2d). Mass spectrometry revealed the presence of several metals in the deposits, including silver (Fig. S2e). Based on these results, the patient was diagnosed with argyria. Other than exposure to silver nitrate in her childhood, she had 17 metal dental crowns, which included silver to some extent. However, it is widely recognized that generalized argyria requires exposure to silver at a total dose of 6 g orally or 1 g intravenously (3). In addition, to date, there have been no reported cases of argyria related to dental metal crown, despite its widespread use worldwide. Therefore, it was concluded that her metal crowns were unlikely to be related to the widely distributed depositions of silver.
Fig. 1. Gross appearance before and after laser therapy. (a) Blue-grey discolouration on the face before treatment. (b) Her facial complexion was restored after laser therapy. Photograph taken 15 years after treatment. Permission is given to publish these photos.
The discolouration on her face was treated with a Q-switched 755-nm alexandrite laser. In a skin biopsy from the treated site 8 months after the initial laser treatment, the deposits on the elastic fibres were found to be completely fragmented into 10–20-nm in diameter particles, including a lower amount of silver (Fig. S3a, b). It is notable that some deposits, consisting mainly of silver, were detected in the endoplasmic reticulum of macrophages (Fig. S3c, d). She underwent additional laser therapy 4 times, and the favourable response has persisted for more than 10 years without any long-term adverse effects (Fig. 1b).
It is currently unknown how laser therapy normalizes dyspigmentation of argyria and how long the therapeutic effect lasts. In the current case, biopsies were performed before and after treatment, providing a useful clue to the above-mentioned issues. In the specimen before treatment, deposits were observed under electron microscopy as 100–200-nm in diameter particles on elastic fibres. After treatment, those deposits were fragmented into much smaller pieces. Using the corresponding skin samples, mass spectrometry was conducted over the electron-dense granules. Before the laser treatment, there were high peaks specific for silver and low peaks for selenium and copper. In general, the copper peak is due to the copper mesh used for the electron microscopy techniques. Importantly, silver nitrate-associated dyspigmentation is caused by deposition of silver selenide (4), plausibly explaining the peaks of silver and selenium in the present case. In addition, there was a small peak for lead, which is probably because the patient was occupationally exposed to lead for ~20 years. After the laser treatment, of note, the peaks of silver were remarkably decreased, in parallel with the complete fragmentation of electron-dense particles into smaller pieces. In addition, the deposits in the endoplasmic reticulum of macrophages revealed high peaks of silver, suggesting clearance of silver by macrophages.
Based on these findings, we speculate that fragmentation of silver particles and their clearance by macrophages may explain the favourable outcome of laser therapy for discolouration in the current case.
A case of argyria relapse reported by Krase et al. (5) provided us with a useful clue to better understand the mechanism by which the laser application improves discolouration characteristic of argyria. Their case underwent the recurrence of milder discolouration in sun-exposed areas after the initial favourable clearing. It is generally accepted that discolouration of argyria is attributable to the conversion of colourless silver salts to black silver sulphide tarnish via an ultraviolet-induced reduction (also known as “intradermal photograph”) (6). Taking this notion into account, argyria relapse in sun-exposed areas suggests that the laser treatment converts silver sulphide tarnish back to elemental silver, the residual of which can again be reduced to black silver sulphide due to ultraviolet exposure. As demonstrated in the current case, the laser treatment fragmented silver deposits into smaller pieces, and they were cleared, at least partially, by macrophages. However, as shown in mass spectrometry, the fragmented particles on elastic fibres still included silver, even though a limited amount was detectable. Therefore, avoidance of ultraviolet seems to be quite important to reduce the risk of argyria relapse after laser therapy. In the current case recurrence of discolouration could be prevented by using sunscreen cream. To date, it is unclear whether the risk of recurrence of argyria depends on ultraviolet avoidance and/or the efficiency of silver clearance. It is notable that, in the current case, the efficacy of Q-switched alexandrite laser lasted more than 10 years. To our best knowledge, this is the longest follow-up report of argyria after laser therapy.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize