


1Division of Dermatology, Rabin Medical Center – Beilinson Hospital, Petach Tikva, and 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
The long-term effect of intra-anti-interleukin-17-class switch on drug survival is unclear. The aim of this study was to evaluate the efficacy and long-term survival of ixekizumab in bio-experienced psoriatic patients with and without previous exposure to anti-interleukin-17 treatment. Retrospective search of a tertiary medical centre database for 2017 to 2019 yielded 73 patients treated with ixekizumab: 50 previously exposed to secukinumab and 23 anti-interleukin-17-naïve. Median baseline Psoriasis Area Severity Index (PASI) was 23.0. Median number of received biologics was 4. Mean drug survival was 16.4 and 16.8 months in the anti-interleukin-17-exposed and naïve groups, respectively (p = 0.878). There was no between-group difference in proportion of patients achieving ≥ 75 PASI response. At study end, 25 anti-interleukin-17-exposed patients (50.0%) and 17 anti-interleukin-17-naïve patients (73.9%) were still on ixekizumab. The use of multiple previous biologic treatments was associated with substantially reduced ixekizumab survival. In conclusion, previous anti-interleukin-17-exposure was associated with an initially favourable response and did not further reduce ixekizumab survival.
Key words: psoriasis; ixekizumab; secukinumab; anti-IL-17; drug survival; switch.
Accepted Nov 27, 2020; Epub ahead of print Dec 7, 2020
Acta Derm Venereol 2020; 100: adv00349.
doi: 10.2340/00015555-3714
Corr: Lev Pavlovsky, Division of Dermatology, Rabin Medical Center – Beilinson Hospital, Petach Tikva 4941492, Israel. E-mail: levpav@gmail.com
Intra-class secukinumab-to-ixekizumab switch was effective in patients with moderate-to-severe psoriasis. In this first direct comparison of heavily pretreated psoriatic patients with/without anti-interleukin-17 switch, ixekizumab drug survival was decreased regardless of previous exposure to secukinumab. Efforts should be made to optimize first-line biologic treatment in order to prevent multiple drug switching.
Biologic drug survival is relatively low in Israeli patients with psoriasis (1), leading to inter- and intra-class switching. Several studies have found evidence of successful switching among anti-tumour necrosis factor (TNF)-alpha drugs (2–8).
Anti-interleukin (IL)-17 (anti-IL-17) agents have been associated with a high and durable response rate in randomized controlled and extension trials of psoriatic patients (9–12). The UNCOVER-3 extension trial, in which 15% of the cohort had had previous biologic treatment, reported good efficacy for the IL-17 inhibitor ixekizumab over 108 weeks of treatment (12). However, some real-life studies of secukinumab, the first anti-IL-17 drug approved for clinical use, found that drug survival was reduced (13–15). There are few real-life drug survival studies of ixekizumab (16–24), and most of those performed were short term (16, 18, 20).
The effect of switching among anti-IL-17 agents on the efficacy of treatment and drug survival is currently under investigation. However, data on ixekizumab are limited. The aim of the present single-centre study was to evaluate ixekizumab efficacy and survival in heavily pretreated psoriatic patients, some of whom were previously exposed to secukinumab (i.e. intra-class secukinumab-to-ixekizumab switch) and others were not (no intra-class switch).
Study design and setting
A retrospective cohort study was conducted between 1 August 2017, when ixekizumab was approved for use in Israel (2 years after secukinumab), and 1 November 2019 in the outpatient psoriasis clinic of Rabin Medical Center, a tertiary hospital. Rabin Medical Center belongs to Clalit Health Services, the largest public health maintenance organization in Israel, serving over 4.3 million patients.
According to Israeli regulatory guidelines for the treatment of psoriasis, patients are eligible for biologic treatment if they fulfil the following criteria: involvement of > 50% body surface area (BSA) or Psoriasis Area and Severity Index (PASI) > 50 or involvement of sensitive areas defined as the face, neck, intertriginous areas, palms, soles and genitals; and failure of at least 2 previous standard systemic treatments (including phototherapy). The internal guidelines of Clalit Health Services stipulate that ustekinumab, an IL-17 inhibitor, or guselkumab may be prescribed to patients with psoriasis following the sequential failure of 2 TNF-α inhibitors (etanercept, adalimumab, infliximab) or apremilast. Both secukinumab and ixekizumab are administered as specified by the US Food and Drug Administration-approved label.
Participants
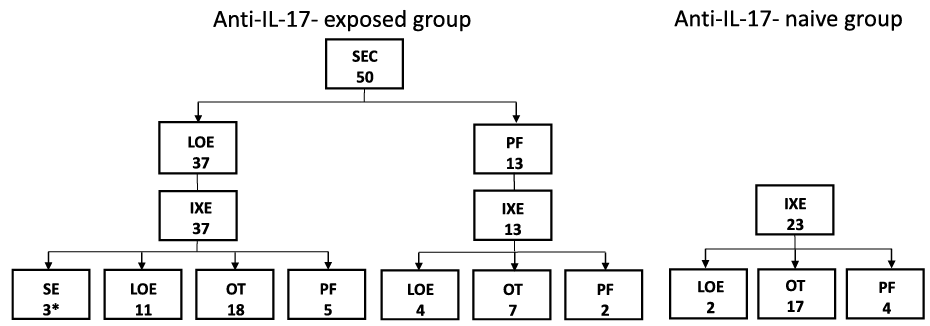
Bio-experienced patients with moderate-to-severe psoriasis who were treated with ixekizumab during the 2-year study period were identified by database search. They were divided into 2 groups according to prior drug use (Fig. 1): those who had previously received secukinumab and were switched to ixekizumab (anti-IL-17-exposed group), and those who had never received secukinumab (anti-IL-17-naïve group). The treating physician decided which anti-IL-17 drug was to be administered first, based on the individual patient’s clinical condition and preferences (2 injections of 150 mg each of secukinumab or 1 injection of ixekizumab, with a longer induction period for secukinumab).
Fig. 1. Flow chart showing rates of survival of ixekizumab and reasons for its discontinuation in the anti-interleukin (IL)-17-exposed and anti-IL-17-naïve groups. SEC: secukinumab; IXE: ixekizumab; PF: primary failure; LOE: loss of efficacy; OT: ongoing treatment; SE: side-effects. *Angioedema and psoriatic arthritis exacerbation.
Demographic and clinical data
Data were collected from the clinic’s electronic registry, as described in our previous study (22), as follows: demographic and baseline characteristics, comorbidities, presence of psoriatic arthritis, previous biologic treatments for psoriasis, baseline disease severity, as assessed by involved BSA and PASI, duration (in months) of secukinumab and ixekizumab treatment, and reason for their discontinuation. Primary failure was defined as the inability to achieve a PASI 50 response within 3 months, and secondary failure, as the loss of an adequate response requiring treatment discontinuation. Effective ongoing treatment was measured by the PASI response in patients still on ixekizumab treatment at the end of the study period (1 November 2019) or at the closest follow-up visit (usually within one month prior to the end of the study period). The duration of effective ongoing treatment was calculated (in months) from the date of drug initiation to study end/closest follow-up. In addition, the electronic prescription-filling patterns were checked at study end. In cases of treatment failure, drug survival was calculated (in months) from the date of drug initiation to the date of withdrawal. In the calculation of the number of previous lines of treatment, we excluded biologic treatments registered for psoriatic arthritis, but not psoriasis (e.g. golimumab) and apremilast. Patients who discontinued a certain line of treatment (whether due to failure or for technical or logistic reasons) and then reused the agent were considered as having received only one line of treatment with the same agent.
The study was approved by the local Institutional Review Board, which waived the need for informed consent.
Statistical analysis
Continuous quantitative variables (age, body mass index (BMI), PASI, BSA, treatment duration) are presented as either mean and standard deviation (SD) or median and interquartile range (IQR) after normality testing. Numeric variables were compared between groups using independent Student’s t-test (with Levene’s test) or Mann–Whitney U test for variables not normally distributed. Kaplan– Meier curves were generated to estimate drug survival, and the Gehan-Breslow-Wilcoxon method was employed to compare anti-IL-17-exposed patients with anti-IL-17-naïve patients. To assess the difference between groups in the proportion of patients achieving PASI improvement at different time-points, we used a generalized estimating equations (GEE) model with a logit link for the repeated measures. A 2-tailed p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed with SPSS ver. 21.
The cohort included 73 patients treated with ixekizumab. Their clinical characteristics are shown in Table I. There were 40 male (54.8%) and 33 female patients; mean age 54.2 years (range 22.3–86.5 years) at ixekizumab initiation. Median BMI was 31.0 kg/m2 (IQR 7.8). Thirty-seven patients (50.7%) had psoriatic arthritis. Median baseline PASI was 23.0 (IQR 15.4) and median involved BSA was 55.0% (IQR 10). Excluded from the baseline BSA and PASI calculations were patients with palmoplantar psoriasis (n = 6), genital psoriasis (n = 2), and facial psoriasis (n = 1), and patients prescribed biologic treatment for psoriatic arthritis by a rheumatologist (n = 4). Patients had been prescribed a median of 4 (IQR 2) lines of treatment before ixekizumab.
Table I. Clinical characteristics in psoriatic patients treated with ixekizumab, whole group and by anti-interleukin (IL)-17 exposure
Clinical and demographic variables
Of the 73 patients in the cohort, 50 had been previously exposed to the anti-IL-17 agent secukinumab; all were switched directly from secukinumab to ixekizumab. The remaining 23 patients were anti-IL-17-naïve. The characteristics of the 2 groups are summarized in Table I. At the time of initiation of ixekizumab treatment (baseline), there were no differences between the groups in sex distribution, mean age, median BMI, involved BSA, and PASI. There was a significant between-group difference in median duration of biologic treatment prior to ixekizumab (5.0 years vs 1.0 year, p = 0.001) and in median number of biologic agents (including ixekizumab) prescribed (5.0 vs 3.0, p < 0.0001).
Ixekizumab drug survival
The median duration of follow-up after ixekizumab initiation was 9.2 months (IQR 11.0). At the end of the study period, 42 patients (57.5%) had used ixekizumab for a median of 10.2 months (IQR 14.1). The estimated 1-year drug survival rate for the whole cohort was 63%. (Data were derived from the survival table). At the end of the study, 25 anti-IL-17-exposed patients (50%) and 17 anti-IL-17-naïve patients (73.9%) were still using ixekizumab. A flow chart showing the final status of ixekizumab use by group is shown in Fig. 1. There was no difference in drug survival between the anti-IL-17-exposed group and the anti-IL-17- naïve group (16.4 vs 16.8 months, p = 0.878; Fig. 2).
Fig. 2. Kaplan–Meier curve of ixekizumab survival in anti-interleukin (IL)-17-exposed and anti-IL-17-naïve patients. *Subjects who had not yet experienced the event before the end of the study (i.e. recruited late during the study).
Ixekizumab efficacy
Comparison of the proportion of patients in in each group achieving PASI 75, PASI 90, and PASI 100 and the reasons for discontinuation of ixekizumab are presented in Table II. Using a GEE model to analyse longitudinal differences in PASI response between groups, no difference was observed in the proportion of patients achieving a PASI 75 and PASI 100 response at weeks 12, 24, 52, 72, and 104. PASI 90 response was marginally different between the groups, owing to the larger proportion of IL-17-naïve patients who achieved PASI 90 after 12 weeks (71.4% vs 43.8%; p = 0.055, χ2 test).
Reasons for discontinuation of ixekizumab
Anti-IL-17-exposed patients were more likely to discontinue ixekizumab because of loss of efficacy (15/25, 60%). By contrast, most of the failures in the anti-IL-17-naïve group (4/6, 67%) occurred during the loading period (i.e. ixekizumab 80 mg biweekly). Among the anti-IL-17 exposed patients, those with primary failure of secukinumab mostly experienced secondary (not primary) failure of ixekizumab (Fig. 1).
Three patients in the anti-IL-17-exposed group discontinued ixekizumab because of side-effects (angioedema and psoriatic arthritis exacerbation).
Table II. Ixekizumab efficacy and survival in psoriatic patients, whole group and by anti-interleukin (IL)-17 exposurea
The assumption that drug efficacy and survival are decreased in bio-experienced patients has gained support from recent real-life studies (13–15, 21, 25). In the present study of heavily pretreated patients with psoriasis, a substantially low drug survival of 16 months was found for ixekizumab, in line with the few available studies of this specific population (15, 22–24). Nonetheless, we are the first to report that previous exposure to another anti-IL-17 inhibitor does not seem to further decrease long-term drug survival, with efficacy being mostly unaffected (except for short-term PASI 90).
Ixekizumab is the second IL-17 inhibitor agent approved in Israel following secukinumab. An extension study of the UNCOVER-3 trial provided evidence of persistent efficacy of ixekizumab for 2 years. PASI 90 response was maintained in more than 70% of patients, and PASI 100 or Static Physicians Global Assessment (sPGA) [0] was maintained in 50% (12). Only 15% of patients in the study cohort had been treated with a biologic agent (12).
The issue of altered drug performance after intra-anti-IL-17 class switch was raised initially by Georgakopoulos et al. (18) who noted a 71% rate of PASI 75 response (or PGA 0/1) at 12 weeks after secukinumab-to-ixekizumab switch. The authors hypothesized that the difference in efficacy compared with clinical studies might be attributable to the number of previous biologic treatments (mean 3.6) and not merely to the switch itself between the IL-17A antagonists. At the same time, a previous favourable efficacy outcome with secukinumab was correlated with a good response to ixekizumab (18). Thereafter, a Slovenian National Registry study of 98 psoriatic patients treated with ixekizumab reported a low (6.1%) drug discontinuation rate after a maximal observation time of 20 months. However, 75% of the patients were treated with ixekizumab as the first or second line of treatment (22).
Our previous study of the performance of ixekizumab summarized outcome after up to one year of treatment in 25 patients who were switched from secukinumab (21). The mean duration of ixekizumab administration was 7.3 ± 2.8 months; 88% of patients were still on ixekizumab at the end of the study, and 68% achieved a PASI 75 response (21). At the time of writing, one year later, in an extended cohort with a longer follow-up, a detrimental effect of multiple previous biologic treatments (median number of 4 lines) has emerged. Only 57.5% of the patients were still being treated with ixekizumab at a median follow-up time of 9.2 months (IQR 11.0). In addition, in the current study, the 37% rate of ixekizumab discontinuation at one year was higher than reported in a Japanese cohort (27%) after a median of 318.5 days (23), and the rate of drug survival in the current study was similar to the 57% drug persistence rate at one year reported by Blauvelt et al. (24). Thus, in their recent study of 62 ixekizumab-treated psoriatic patients in Denmark, Egeberg et al. (15) reported an 83% drug survival at 6 months in the bio-experienced patients compared with 100% (as extracted from the Kaplan–Meier curve) in the bio-naïve patients, supporting a negative effect of previous bio-experience on drug performance. After 12 months, drug survival decreased to approximately 76% in the bio-experienced patients. The effect of intra-class IL-17 inhibitor switch on drug survival was not evaluated, since only 2 patients were switched directly from secukinumab to ixekizumab (15).
The current evaluation of the direct effect of the intra-anti-IL-17 switch revealed no difference between the anti-IL-17-exposed and anti-IL-17-naïve groups (Fig. 2). In addition, there was no pattern of a steep incline in drug discontinuation after the loading dose; rather, drug failures were spread throughout the study period. A similar finding was previously reported for secukinumab (13).
Lunder et al. (22) showed that drug survival had a class effect. The current findings are in partial agreement, even though both anti-IL-17 agents were prescribed mostly as first- or second-line treatment in their cohort, whereas in ours, they were the 4th or 5th line of treatment. It was observed that, even after primary failure of secukinumab, most patients were initially responsive to ixekizumab and only later did the drug exhibit loss of efficacy (Fig. 1). However, mean drug survival of ixekizumab was limited to 16–17 months, regardless of previous anti-IL-17 exposure (Fig. 2).
Previous IL-17 exposure had little effect on PASI improvement rates (Table II). The current short-term efficacy results are mostly in accordance with the recent systematic review and meta-analysis of Loft et al. (25) assessing the efficacy of treatment with a second IL-17 inhibitor in patients with psoriasis. The authors concluded that there was no further decrease in efficacy of a second IL-17 inhibitor after intra-class switch compared with real-world studies. However, their analysis was limited by the scarcity of reports on long-term efficacy and the lack of information on response to a previous IL-17 inhibitor. They explained the favourable response of ixekizumab following secukinumab by its better affinity to IL-17A cytokine (25).
The current study was limited by the retrospective design and rather small comparative anti-IL-17- naïve group, which might have led to an underestimation of the between-group differences in drug survival and efficacy. In addition, because of the late introduction of ixekizumab to Israel, the duration of follow-up of the anti-IL-17-naïve patients was short, which may have biased the survival analysis in this group.
In conclusion, the main novelty of this study is the investigation of ixekizumab survival and efficacy in a cohort composed solely of bio-experienced patients. The results showed that, despite promising sustainability of ixekizumab, previous treatment with multiple lines of biologic agents are a major obstacle to its survival. The reduction in ixekizumab survival is comparable to most recent real-life studies. Secukinumab-to-ixekizumab switch may yield an initial favourable primary response. It does not seem to significantly undermine the efficacy of ixekizumab, and it does not have a further negative effect on the already decreased ixekizumab survival.
Conflicts of interest: LP has served as an investigator for Abbvie, Coherus, Novartis, Janssen Biotech, Eli Lilly and as an advisor, consultant and/or invited lecturer for Abbvie, Janssen Biotech, Novartis Pharmaceuticals Corporation, Pfizer Inc., Dexcel Pharma, and Eli Lilly.


 Click to show fullsize
Click to show fullsize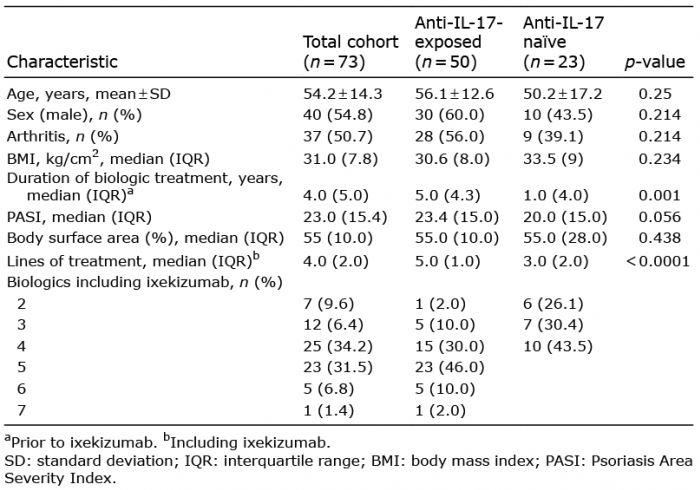 Click to show fullsize
Click to show fullsize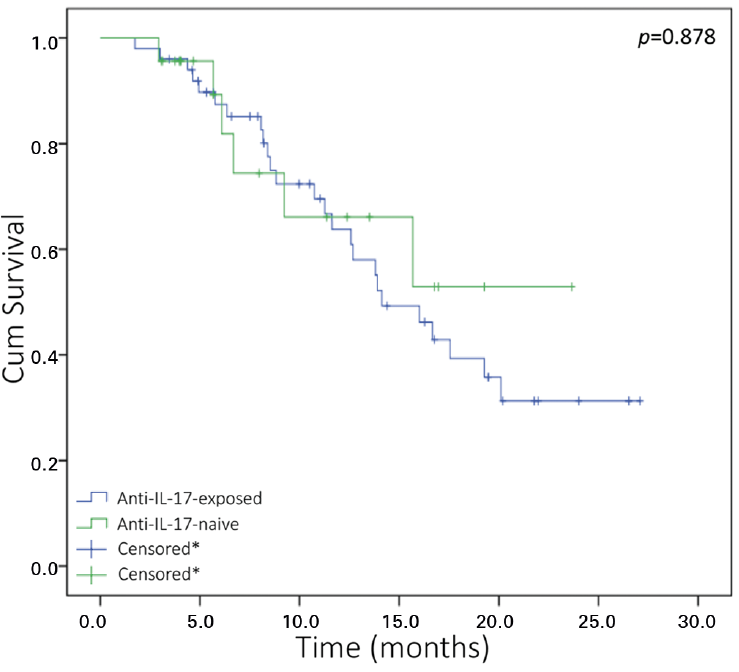 Click to show fullsize
Click to show fullsize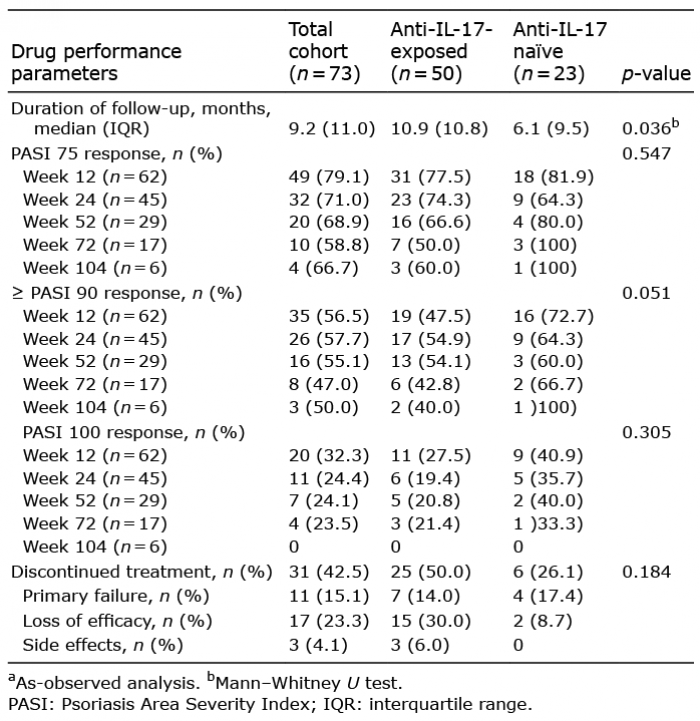 Click to show fullsize
Click to show fullsize