


1Department of Dermatology and 7Center for Clinical Trials Regensburg, University Hospital Regensburg, Regensburg, 2Department of Dermatology and Allergology, Klinikum Vest Academic Teaching Hospital, Recklinghausen, 3Faculty of Health, University Witten/Herdecke, Witten, 4Hautzentrum Köln, Köln, 5Department of Dermatology, University Hospital Düsseldorf, Düsseldorf, and 6Prager & Partner, Hamburg, Germany
Actinic keratoses are a chronic condition in ultraviolet-damaged skin, with a risk of progressing to invasive skin cancer. The aim of this study was to investigate the preventive potential of field-directed repetitive daylight photodynamic therapy for actinic keratoses. A randomized trial was performed, including 58 patients with ≥5 actinic keratoses on photodamaged facial skin, who received either 5 full-face sessions of daylight photodynamic therapy within a period of 2 years or lesion-directed cryosurgery. Primary outcome was the mean cumulative number of new actinic keratoses developed between visits 2 and 6 (visit 6 being a follow-up). This outcome was lower after daylight photodynamic therapy (7.7) compared with cryosurgery (10.2), but the difference did not reach significance (–2.5, 95% confidence interval –6.2 to 1.2; p=0.18). Several signs of photoageing (fine lines, pigmentation, roughness, erythema, sebaceous gland hyperplasia) were significantly reduced after daylight photodynamic therapy, but not after cryosurgery. Significantly less pain and fewer side-effects were reported during daylight photodynamic therapy than during cryosurgery. This study found that repetitive daylight photodynamic therapy had photo-rejuvenating effects. However, the prevention of actinic keratoses by this therapy could not be proven in a statistically reliable manner.
Key words: actinic keratoses; daylight photodynamic therapy; methyl aminolevulinate; photo-rejuvenation; skin cancer prevention; skin ageing.
Accepted Dec 7, 2020; Epub ahead of print Dec 14, 2020
Acta Derm Venereol 2021; 101: adv00355.
doi: 10.2340/00015555-3717
Corr: Sigrid Karrer, Department of Dermatology, University Hospital Regensburg, Franz-Josef-Strauss-Allee 11, DE-93053 Regensburg, Germany, E-mail: sigrid.karrer@ukr.de
Actinic keratoses are a chronic-progressive condition in ultraviolet-damaged skin, with the risk of progression to invasive skin cancer. Effective therapies are available, but the best treatment would be prophylaxis. This trial was based on the hypothesis that daylight photodynamic therapy, applied to the whole face on a regular basis, might prevent the development of new actinic keratoses, by treating not only visible lesions, but also subclinical lesions in sun-damaged skin. Repetitive daylight photodynamic therapy was found to be superior to cryosurgery in preventing the development of new actinic keratoses, although this trend was not statistically significant. Photodynamic therapy was found to improve several signs of photoageing and was better tolerated than cryosurgery.
Actinic keratoses (AKs), a chronic-progressive condition in ultraviolet (UV)-damaged skin, is one of the most frequently diagnosed skin conditions in dermatological practice (1). Although AKs are a precursor of squamous cell carcinoma (SCC), no firm prognosis can be made about the probability of an AK progressing to SCC. The photodamaged area around AKs represents a cancerized field, and is hence referred to as “field cancerization” (2). For patients with multiple AKs, guidelines recommend the treatment of not only single AKs, but also of subclinical lesions present in the field-cancerized area (1, 3). Field-directed therapies include photodynamic therapy (PDT), peeling, dermabrasion, ablative laser therapy, and topical treatments, such as application of imiquimod, diclofenac-sodium 3% in hyaluronic acid 2.5% gel, or 5-fluorouracil (1). These therapies also have the potential to address subclinical damage, to reduce the appearance of new AKs, and potentially reduce the risk of development of SCC. Controlled clinical trials addressing this issue, however, are scarce.
Conventional PDT (C-PDT) with red light is known for its high efficacy and good aesthetic results, but pain during illumination makes it difficult to treat larger skin areas in a single session (4). Daylight PDT (DL-PDT), using natural sunlight instead of red light, is as efficacious as C-PDT, but is associated with less discomfort and pain (5–7). Since relapses are likely, even after effective therapy for AKs, preventive strategies are needed to decrease the number of new AKs and the risk of subsequent development of skin cancer. To date, the only known primary prevention strategy for AKs is avoidance of UV-light exposure and regular application of sunscreen (8).
The current study is based on the hypothesis that field-directed DL-PDT with methyl aminolevulinate (MAL), used on a regular basis, may prevent the development of new AKs, by targeting not only clinically evident AKs, but also subclinical lesions in sun-damaged skin. The primary aim of this clinical trial was therefore to investigate the prophylactic effect of repetitive DL-PDT on the development of new AKs compared with a lesion-directed therapy (cryosurgery) that does not target the photodamaged surrounding skin.
Study design
This investigator-initiated trial was designed as a prospective, randomized controlled multicentre (5 study sites in Germany) 2-armed clinical study comparing 2 treatments. The intervention treatment was MAL application followed by DL-PDT, and the control treatment was cryosurgery, as a standard lesion-directed therapy for AKs. The study participants selected for this study were patients who presented routinely for therapy of their AKs in the Department of Dermatology in hospitals or in private dermatological practices. Patients were randomly allocated to one of the 2 treatment arms according to a 1:1 blockwise randomization scheme, with study site as the stratification factor. The randomization list was generated by the Center for Clinical Studies at University Hospital Regensburg, using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Sequential numbered randomization envelopes including the patient’s study arm assignment were created and stored at each centre. The envelope with the lowest consecutive number was opened by the investigator after a patient had provided signed consent.
Ethical considerations and study registration
The study was conducted in accordance with the German Drug Law (§ 67 Abs. 1 and 3 Arzneimittelgesetz, AMG plus § 12 Abs. 1 GCP-V), international Good Clinical Practice (ICH-GCP Guideline CPMP/ICH/135/95) guidelines, and the Declaration of Helsinki. (59th WMA General Assembly, Seoul, October 2008). The study was approved by the ethics committee of the University of Regensburg (reference 15-112-0068) and the German Federal Institute for Drugs and Medical Devices (BfArM, reference 61-3910-4040415). The study was prospectively registered at EU Clinical Trials Register (EudraCT Number: 2014-005121-13) and at clinicaltrials.gov (ClinicalTrials.gov Identifier: NCT02736760). A published version of the study protocol, based on the SPIRIT recommendations, is available (https://www.spirit-statement.org/) (9).
Inclusion and exclusion criteria
Inclusion criteria were: clinical diagnosis of AKs; a minimum of 5 non-hyperkeratotic, non-pigmented AKs in the face (Olsen grading I or II); Glogau Photodamage Classification Type II (moderate) to IV (severe); Fitzpatrick skin type I–IV; age ≥ 40 years; a negative pregnancy test and use of a highly efficient contraceptive method by women of child-bearing age; and written informed consent.
Exclusion criteria were: known intolerance or allergy to MAL or to any other ingredient of Metvix 160 mg/g cream or Actinica lotion (organic sunscreen, both Galderma Laboratorium GmbH, Düsseldorf, Germany); photosensitivity; diagnosis of porphyria, hyperkeratotic or pigmented AKs in the face; malignant skin tumours in the face or on the scalp requiring treatment; clinically relevant suppression of the immune system; pregnancy or lactation; medical history of PDT in the face during the 6 months preceding study treatment; rejuvenating treatment of the face during the 3 months preceding study treatment; or planned aesthetic treatments in the face in the subsequent 24 months; other topical treatments of AKs in the face in the 4 weeks preceding study treatment; or systemic treatment with retinoids; and suspected lack of compliance (e.g. dementia).
Study procedures
After the screening visit, patients were scheduled for 6 visits within 24 months (see study flow chart, Table SI). Visits 1–3 took place 3 months apart, and the intervals were extended to 6 months after visit 3. Treatments were carried out during visits 1–5, and the final visit (visit 6) was a follow-up visit. At the screening visit, patients were randomly allocated to either the intervention group (DL-PDT) or the control group (cryosurgery). The first patient entered the study on 3 April 2016, and the last patient finished the study on 7 May 2018.
Intervention group: application of methyl aminolevulinate followed by illumination with daylight
Patients received 5 full-face treatments with DL-PDT. First, sunscreen without mineral filters (Actinica lotion, Galderma Laboratorium GmbH, Düsseldorf, Germany), was applied to the entire face and other parts of the body that would be exposed to daylight. After an absorption time of at least 15 min, the surface of the AKs was gently prepared with a curette or a scalpel to remove scales and crusts and to roughen the surface of the lesion. A thin layer of MAL cream (Metvix 160 mg/g cream, Galderma Laboratorium GmbH, Düsseldorf, Germany) was then applied uniformly onto the entire face, including the hairless forehead, but sparing the eyelids, lips and ears. Approximately one tube (2 g) of MAL cream was required to cover the entire face. Within 30 min after MAL application, the skin areas were exposed to daylight for 2 h. Thereafter, patients washed off the MAL cream with clear water. DL-PDT could only be carried out from March to October, in non-rainy weather, and at an outdoor temperature of at least 10°C.
Control group: cryosurgery
In the control group, a single freeze-thaw cryosurgery cycle was conducted at visit 1, using an open spraying procedure with liquid nitrogen for each AK lesion. Freeze time started after formation of an ice ball and lasted 5–10 s per lesion. Cryosurgery was also conducted at visits 2–5 in the case of non-cleared or newly developed AKs.
Outcome assessment
The primary aim of this trial was to investigate the preventive properties of repetitive, field-directed DL-PDT. Hence, the primary outcome was the cumulative number of new AKs developed after visit 1 that were documented between visits 2 and 6. To assess each lesion objectively, the exact location of each AK in the face was marked on plastic sheets. On these sheets, reference points (nose, eyebrows, lips, wrinkles, and moles) were also marked, to ensure that the location of the lesion would be correctly identified at the next visit. The diameter and Olsen grade of each lesion were also documented. At visits 2–6, only newly developed AKs were marked on a new plastic sheet. Missing values of the primary outcome were imputed if the number of newly developed AKs was assessed at least once. Two different types of missing values had to be distinguished: intermittent missing values and measurement dropouts. Intermittent missing values are values missing in longitudinal data. Imputation of intermittent missing values is not necessary because newly developed AKs would automatically be counted in the subsequent visit. In the case of measurement dropouts, the following imputation method was used: the number of newly developed AKs of completed visits was averaged and then multiplied by the number of missing visits. Finally, this computed value was summed with the actual number of newly developed AKs. This conservative imputation method avoids overestimation of the therapeutic effect.
At visits 2–6, the clearance of treated AKs was documented. Clearance was achieved if a lesion was neither visible nor palpable. For each patient, the clearance rate over the course of the study was calculated (total number of cleared lesions/total number of observed lesions) and expressed as a single percentage value (0–100%). At each visit, patients were also examined regarding the appearance of any new malignant skin tumour in the face. Photo-documentation was conducted in a standardized manner at each visit.
Photodamage parameters were evaluated at each visit and included fine lines, mottled pigmentation, skin colour, tactile roughness, telangiectasias, deep wrinkles, facial erythema, and sebaceous gland hyperplasia. The global score for photoageing was also documented. Each photodamage variable was recorded on a 5-point scale (0–4, where higher points indicate higher damage, modified according to the scale by Dover et al. (10) and Zane et al. (11)) (see Table SII). All investigators had been trained in evaluating photodamage parameters, to ensure comparable ratings.
Patient and investigator satisfaction with the cosmetic outcome were evaluated from visit 2 onwards according to the following scale: 1 = very satisfied, 2 = satisfied, 3 = moderately satisfied, and 4 = not satisfied. These satisfaction scorings were averaged across visits 2–6. Patients marked the level of pain experienced during the treatment procedure on a visual analogue scale (VAS, 0 = no pain to 10 = insufferable pain) immediately after the treatment. The investigator rated erythema and oedema after each treatment on a 5-point-scale: 0 (none), 1 (mild), 2 (moderate), 3 (severe) and 4 (very severe). Pain, erythema, and oedema scorings were averaged for visits 2–6. From the second visit onwards, patients were asked if they had experienced any side-effects or adverse events (AEs).
Skin-related quality of life was assessed with the Dermatology Life Quality Index (DLQI) during the screening visit and at visit 6. The DLQI was used to measure how much a patient’s life had been affected by the skin problem during the previous week. The DLQI was calculated by summing up the score of each question, resulting in a maximum of 30 and a minimum of 0 points. The higher the score, the higher the impairment of quality of life (0–1 = no effect at all, 2–5 = small effect, 6–10 = moderate effect, 11–20 = very large effect, 21–30 = extremely large effect on patient’s life) (12).
Statistical considerations
Sample size. The sample size calculation was based on the primary outcome parameter (the cumulative number of new AKs documented between visits 2 and 6). Clinical experience suggests a mean cumulative number of 10 new AKs in the DL-PDT group vs 14 in the cryosurgery group, with a standard deviation (SD) of 5 in both groups. To detect a mean ±SD difference of 4 ± 5 with a power of 80% at a 2-sided alpha significance level of 0.05, a sample size of 26 patients per group is required. To compensate for a loss-to-follow-up rate of 10%, 29 patients per group are needed. Thus, the total number of patients enrolled in this trial was set at 58 patients.
Populations to be analysed. The intention-to-treat (ITT) population consisted of all patients receiving at least one treatment with at least one documented primary outcome. According to the ITT principle, all patients were analysed as belonging to their randomized treatment, regardless of whether treatment was refused or discontinued, or whether other protocol deviations occurred.
The per-protocol (PP) population consisted of the ITT population with no major protocol violations. Major and minor protocol deviations were identified by medically trained staff before database lock. The safety population to account for AEs and serious AEs consisted of all patients who had received at least one treatment.
Statistical analysis
Primary outcome (the cumulative number of newly developed AKs and documented AKs between visits 2 and 6) was compared between the 2 treatment groups using an analysis of covariance (ANCOVA) with treatment (DL-PDT vs cryosurgery) as a fixed factor and the initial number of AKs at baseline as well as the study centre as covariates. Adjusted means and associated 95% confidence intervals (95% CI) were reported. The primary outcome analysis was carried out on the ITT and PP populations and was 2-sided at the significance level of 0.05.
Secondary outcomes were longitudinally assessed at visits 1–6, and thus contained occasional missing values (protocol violation). Therefore, it was decided to conduct secondary analyses using the PP population. All secondary analyses were exploratory and no adjustments for multiple testing were applied. The percentage of clearance of AKs was assessed via a linear mixed model (fixed factors = treatment and Olsen grade; random factor = patients). Student’s t-tests for independent samples were used for the treatment comparison regarding scores for pain, erythema, swelling and satisfaction with the cosmetic outcome. The results of parametric and non-parametric tests were comparable. The course of the 9 photodamage parameters and quality of life within each treatment group were assessed with the Wilcoxon and Friedman tests, and between-treatment comparisons for each assessment time-point were conducted with the Mann–Whitney U test. Baseline characteristics and safety variables were analysed descriptively. Statistical analyses were performed with SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Study population
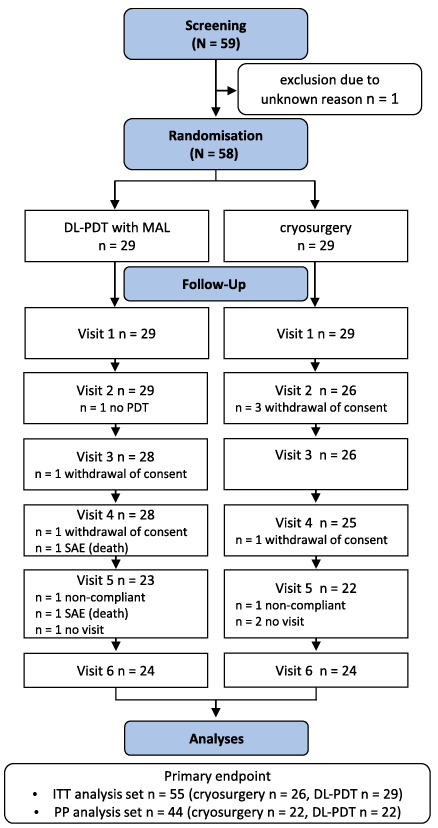
Of the 58 patients enrolled in this study, 29 were randomized to receive DL-PDT and 29 to receive cryosurgery (see Fig. 1 for the Consort flow diagram). Patients’ demographics and baseline characteristics are shown in Table I; all patients demographics (age, sex) and baseline characteristics (Fitzpatrick type, Glogau classification, number of AKs at baseline, diameter of AKs) were equally distributed across the two treatment groups.
Fig. 1. Consort flow diagram. N: number of patients; DL-PDT: daylight-photodynamic therapy; MAL: methyl aminolevulinate; PDT: photodynamic therapy; SAE: serious adverse event; ITT: intention-to-treat; PP: per-protocol.
Table I. Demographics and baseline characteristics of both treatment groups
Treatment-related parameters
In the DL-PDT group, the mean incubation time with MAL cream prior to sunlight exposure was 12.6 ± 10.5 min (range 1–30 min). Mean duration of sunlight exposure was 120 ± 0.5 min (range 117–125 min). Mean temperature during sunlight exposure was 17.0 ± 5.1°C (range 10.0–30.0°C). The weather conditions during sunlight exposure were sunny in 43.3% of all sessions, partly cloudy in 42.5%, and cloudy in 14.2%. During 7 (5.2%) PDT sessions, daylight exposure was briefly interrupted for 3–5 min.
In the cryosurgery group, mean freezing duration per lesion after formation of an ice ball (392 AKs treated during visits 1–5) was 6.3 ± 1.8 s (range 5–10 s).
Primary outcome: prophylactic effect
The prophylactic effect was assessed by the cumulative number of newly developed AKS documented between visits 2 and 6. According to the ITT analysis (n = 55), fewer new AKs developed in the DL-PDT group (unadjusted mean ± SD 8.2 ± 7.0; adjusted mean 7.7, 95% CI 5.5/10.3) than in the cryosurgery group (unadjusted mean ± SD 10.1 ± 6.3; adjusted mean 10.2, 95% CI 7.5/12.9). The adjusted mean difference of –2.5 (95% CI –6.2/1.2) was not statistically significant, F(1.55) = 1.824, p = 0.183 (Fig. 2). Analysis of the PP population (n = 44) confirmed this finding, F(1.44)=0.378, p = 0.542 (Table II).
Fig. 2. Adjusted means and 95% confidence intervals (95% CI) of the cumulative number of newly developed actinic keratoses (AKs) documented during visits 2–6 in the intention-to-treat (ITT)-population (n = 55). The difference between DL-PDT and cryosurgery was not significant, p = 0.183. DL-PDT: daylight photodynamic therapy.
Table II. Comparison between daylight photodynamic therapy (DL-PDT) and cryosurgery (per-protocol population: PP-population)
Secondary outcomes
Clearance of actinic keratoses. The linear mixed model yielded no significant difference in the mean rate of clearance between patients treated with DL-PDT (63.5%, 95% CI 52.6%/74.5%) and those treated with cryosurgery (52.4%, 95% CI 41.3%/63.5%), p = 0.154 (Table III). The mean percentage of clearance differed among the Olsen grades (Olsen grade I: mean 74.7% (95% CI 65.9%/83.5%), Olsen grade II: mean 64.0% (95% CI 55.5%/72.5%), Olsen grade III: mean 35.2% (95% CI 16.9%/53.5%), p = 0.001). The mean percentage of clearance was significantly lower in Olsen grade III AKs than in Olsen grade I AKs (p < 0.001) and Olsen grade II AKs (p = 0.005). The interaction between Olsen grade and treatment was significant, p = 0.045 (Table III). Within Olsen grade I (p = 0.533) and II (p = 0.594), the treatment groups did not significantly differ in the mean percentage of clearance of AKs (Table III). However, Olsen grade III AKs responded significantly better to DL-PDT than to cryosurgery (p = 0.021).
Table III. Comparison of complete clearance of actinic keratoses (AKs) between daylight photodynamic therapy (DL-PDT) and cryosurgery according to the Olsen grade (per-protocol population)
Cosmetic result. Within the DL-PDT group, 6 out of the 9 parameters of photoageing were significantly reduced between visits 1 and 6: fine lines (p < 0.001), mottled pigmentation (p = 0.007), tactile roughness (p < 0.001), skin colour (p = 0.016), facial erythema (p < 0.001), and sebaceous gland hyperplasia (p = 0.017) (Fig. 3 a–i). No significant improvement was found in the global photoageing score (p = 0.173), telangiectasias (p = 0.082), or deep wrinkles (p = 0.595).
Fig. 3. Course of (a–i) skin ageing parameters and (j) skin-related quality of life in the per-protocol (PP)-population. Blue line: daylight photodynamic therapy; red line: cryosurgery.
In contrast, patients in the cryosurgery group showed no significant changes in any of the 9 signs of photoageing between visits 1 and 6 (p > 0.050). Between-group comparisons showed that patients in the DL-PDT group had significantly fewer mottled pigmentations (p = 0.032) and facial erythema (p = 0.037) at visit 6 than patients in the cryosurgery group. No further significant differences were found between the groups at baseline or at visits 2–5.
Patient and investigator satisfaction with the cosmetic result. Mean patient satisfaction with the cosmetic result (visits 2–6) did not differ significantly between treatment groups, p = 0.627 (Table II). Mean investigator satisfaction with the cosmetic results (visits 2–6) was higher for DL-PDT than for cryosurgery, p = 0.027 (Table II).
Quality of life (Dermatology Life Quality Index). In both treatment groups, skin-related quality of life improved significantly over time, DL-PDT: p = 0.020, cryosurgery: p = 0.020 (Fig. 3j). At the screening visit, quality of life was slightly impaired in both groups, but no impairment was reported at visit 6. There was no significant difference between groups at the screening visit (p = 0.119) or at visit 6 (p = 0.367).
Pain and local reactions. Patients receiving DL-PDT reported significantly less pain (p < 0.001, mean VAS 0.9 after DL-PDT vs 3.2 after cryosurgery), and showed less swelling (p = 0.001) and less pronounced erythema (p < 0.001) after treatment than patients receiving cryosurgery (Table II).
Some local reactions were reported in the DL-PDT group during visit 1 only. One patient reported some burning in the entire face, one patient reported crusting, and one patient felt slight pruritus on the nose.
Safety. Overall, 56 AEs occurred in 24 patients: 23 in the DL-PDT group and 33 in the cryosurgery group. Of the total AEs, 31 were mild, 23 moderate, and 2 severe. In only one case of pruritus was the AE related to the study treatment (DL-PDT); all other AEs were unrelated to the study procedure.
Eight serious AEs (SAEs) occurred in 8 patients, but none of the SAEs were related to the study procedure. Six of these patients had received DL-PDT and 2 had received cryosurgery. All SAEs led to hospitalization; 5 were moderate, one life-threatening, and 2 fatal. The life-threatening SAE (lacunar stroke) occurred in the cryosurgery group. Both fatal SAEs occurred in the DL-PDT group; one patient died of myocardial infarction, and the cause of death in the other patient was unknown.
Two patients developed a malignant skin tumour in the face during the study period. One patient in the DL-PDT group developed a basal cell carcinoma (BCC), which was diagnosed at visit 3, and one patient in the cryosurgery group developed a SCC, which was diagnosed at visit 6. Both tumours were treated surgically.
Prevention and early management of AKs in field-cancerized and photodamaged skin may have profound implications for prevention of skin cancer. Although one of the most important claims of field-directed DL-PDT is the treatment of cells with cancerogenic potential in subclinical areas of photodamaged skin, this has not been sufficiently proven in controlled clinical trials. Therefore, this study investigated the preventive potential of repetitive DL-PDT with MAL in patients with photodamage and multiple AKs on the face, using the mean number of newly developed AKs as the primary endpoint. Cryosurgery was chosen as control instead of a placebo treatment, since it would have been unethical to leave AKs untreated for the study duration of 2 years, due to their precancerous potential. Since cryosurgery only targets single lesions, no preventive effect in field-cancerized areas of the surrounding skin can be expected.
The effectiveness and tolerability of DL-PDT in the treatment of AKs has been proven in several studies. Two phase III studies have shown that DL-PDT with MAL is as efficacious as C-PDT with red light, but was better tolerated, almost painless, and more convenient for patients. Complete remission rates of AKs at week 12 were 70–89% after DL-PDT and 74%–93% after C-PDT (6, 7). DL-PDT also has the advantage that clinic visits can be avoided because no equipment is needed, and patients can treat themselves at home (13). Thus, patient motivation for retreatment is high, and DL-PDT can easily be repeated on a regular basis. However, no studies are available to date on the effect of long-term repetitive DL-PDT on the prevention of AKs. Studies in immunocompromised patients have shown the potential of C-PDT to delay or reduce the development of new AKs when it is used on larger skin areas (14–16). Organ transplant recipients with AKs were treated with 2 cycles of MAL-PDT compared with cryosurgery (15). Significantly fewer new AKs were present 3 months after C-PDT. After 27 months, the difference was no longer significant, suggesting that repeated treatments may be necessary for a prolonged preventive effect. The potential of CPDT with MAL repeated every 6 months in renal transplant recipients is therefore being investigated over a period of 5 years. Interim analysis at the 3-year follow-up has shown a significantly delayed onset of AKs compared with untreated skin (16). Another study investigated the preventive potential of C-PDT with aminolaevulinic acid (ALA) in immunocompetent patients with face and scalp cancerization, showing a significant delay of approximately 6 months in the development of new AKs compared with control sites (17). The efficacy of C-PDT with MAL (2 sessions one week apart) as a preventive strategy in 44 patients with field cancerization was compared with that of topically applied imiquimod 5% (18). The total number of new AKs developed over a 12-month follow-up period did not significantly differ between these 2 field-directed treatment regimens. However, C-PDT with red light resulted in burning, stinging, and pain in all patients, making the procedure not very convenient. This problem can be overcome with DL-PDT, which is almost painless. Therefore, the same study group compared DL-PDT with C-PDT in 26 patients with face and scalp cancerization (19). Two contralateral areas received 2 sessions, one week apart, of either DL-PDT or C-PDT with MAL. At the follow-up visits 3, 6, 9, and 12 months after PDT, the total number of newly developed AKs did not significantly differ between the 2 treatment areas with a time-related gradual decrease in the prophylactic effect. Patients’ preference was clearly in favour of DL-PDT. The authors suggest that the optimal time-point for a further session of DL-PDT, in order to sustain the preventive potency, may be 6 months after the final treatment. Furthermore, periodic use of DL-PDT may result in adequate control of recurrences in patients with field changes.
This study investigated the prophylactic efficacy of repeated DL-PDT with MAL compared with lesion-directed cryosurgery in immunocompetent patients with multiple facial AKs. In the first year, 3-month intervals were chosen between visits 1 and 3 in order to gain good control of the disease, and thereafter the intervals were extended to 6 months. Treatment with DL-PDT had to be conducted between March and October, since DL-PDT could not be used during the winter months (due to low levels of sunlight). At every visit, the entire face was treated with DL-PDT, even if no new AKs were detected. In contrast, cryosurgery was conducted only when new or non-healed AKs were present. After 5 treatment sessions, within 18 months and 6 months of follow-up, the cumulative mean number of new AKs was not significantly different between DL-PDT (7.7) and cryosurgery (10.2). The adjusted mean difference was only 2.5, and thus lower than the expected mean difference of 4. Furthermore, unadjusted means and SDs showed that the SDs of the primary endpoint variable were higher than the expected value of 5 in both groups (observed SD 7.0 for DL-PDT and 6.3 for cryosurgery). Nevertheless, the mean difference expected initially was within the 95% CI of the primary endpoint variable, as observed in the present study. Thus, it can be concluded that the initial assumption regarding the size of the treatment effect was too optimistic and that the trial was underpowered. A further explanation from a methodological standpoint is “chance”, as there is always to possibility that study results are negative despite a true initial assumption about the effect size. A power of 80% implies that 2 out of 10 studies will yield a non-significant result even when true differences are present in the parent population. Thus, the study results may not reflect the true effect of the treatment under investigation.
From a clinical perspective, the concept of prevention requires a long-term study of at least 5 years with continuously repeated sessions of DL-PDT. This should result in a more pronounced prevention effect. A trial with a longer observation period, in combination with a larger sample size, is necessary to determine the hypothesized prevention effect in a statistically reliable manner.
Another possible limitation of this study is that most patients had a relatively mild disease with a mean number of facial AKs at baseline of 7.2 ± 1.9 in the DL-PDT group and 6.4 ± 2.2 in the cryosurgery group. A minimum of 5 AKs in moderately to severely photodamaged facial skin was chosen as an inclusion criteria, since this conforms with the most common definitions of field cancerization (20). However, if patients with more severe damage had participated in this study, it is possible that the preventative activity might have been greater.
An important secondary outcome of this study was the cosmetic effect of repetitive DL-PDT; patients with AKs usually also show signs of photoageing. Therefore, simultaneous treatment of AKs and facial photodamage would be beneficial for affected patients. Several studies have reported rejuvenating effects of C-PDT, resulting in a reduction in fine wrinkles, mottled pigmentation, tactile roughness, skin texture, telangiectasias, facial erythema, and sallowness (5, 21, 22). Immunohistochemical analyses have shown upregulation of collagen production and reduction in elastotic material in the dermis after C-PDT (23–25). These molecular effects, together with the disappearance of Tp53, a marker for epidermal carcinogenesis, may explain why PDT reverses the signs of photoageing (26). To date, clinical studies have provided little evidence that DL-PDT may also reduce facial photodamage (27). The current study investigated, for the first time, the photo-rejuvenating effects of repetitive DL-PDT with MAL. In the DL-PDT group, 6 out of 9 parameters of photoageing significantly improved over time: fine lines, mottled pigmentation, tactile roughness, skin colour, facial erythema, and sebaceous gland hyperplasia. In the cryosurgery group, no signs of photoageing were significantly altered. Patient satisfaction with the cosmetic result was mostly good or very good in both treatment groups, with no significant differences, whereas investigators were significantly more satisfied with the cosmetic results of DL-PDT. Since patients experienced only DL-PDT or cryosurgery, a direct comparison regarding cosmetic results was not possible as it would have been in a split-face study. The fact that photoageing parameters improved significantly, whereas the cancerogenic potential of the cancerization field could not be significantly reduced is not necessarily a contradiction: While PDT destroys cancerogenic cells via reactive oxygen species within tumour cells in the epidermis, photo-rejuvenating effects are caused by other mechanisms of action, such as activation of fibroblasts and induction of cytokines, resulting in collagen remodelling in the dermis (21, 23).
Further secondary outcomes included efficacy and tolerability of the treatment. Overall complete lesion clearance of AKs did not differ significantly between DL-PDT (63.5%) and cryosurgery (52.4%), but was clinically relevant, with a mean difference of 11.2%. Mild and moderate AKs responded better to treatment than thick AKs. However, the total number of thick AKs (Olsen grade III) was very low (n = 4 in each group), since thick AKs were an exclusion criterion at study entry and were treated only when they newly occurred during the study period. Other controlled studies have shown similar efficacy of cryosurgery and C-PDT, but this study is the first direct comparison between cryosurgery and DL-PDT (28, 29). Concerning tolerability of treatment, this study showed significantly lower mean pain scores for DL-PDT (VAS 0.9) than for cryosurgery (VAS 3.2). In addition, DL-PDT was associated with significantly less swelling and fewer erythema than cryosurgery. Regarding these main results, the higher costs of DL-PDT compared with cryosurgery could be justified, based on the fact that DL-PDT was better tolerated and gave better cosmetic results in the treated field, even though it did not result in improved efficacy or significant preventive effects.
Skin-related quality of life was investigated using the DLQI. Both treatment groups reported only slightly impaired quality of life at baseline, which improved over time, with no impairment at visit 6. This improvement might be due to the fact that regular treatments and medical consultations reassure patients regarding the risk of developing invasive skin cancer.
To address the question as to whether repeated DL-PDT may prevent the development of invasive skin cancer, any new tumour in the treatment area was documented. One patient in the DL-PDT group developed a BCC in the face that was diagnosed at visit 3, and one patient in the cryosurgery group developed a SCC that was diagnosed at visit 6. However, the limited sample size and short duration of the study do not allow any conclusions to be drawn from these results. Only one study has investigated the potential of C-PDT, conducted every 4–8 weeks for 2 years, to reduce the incidence of SCC in 12 high-risk solid-organ transplant recipients (SOTRs) (30). The number of SCCs developed after the start of the study was compared with the number of SCCs developed during the year before study initiation. The median reduction in SCCs between the pretreatment counts and the 12- and 24-month post-treatment counts was 79% and 95%, respectively. The authors conclude from these results that cyclic C-PDT may reduce the incidence of SCC in SOTRs.
In conclusion, DL-PDT and cryosurgery did not differ significantly with regard to the cumulative number of newly developed AKs; a too-short observation period and a small sample size may be responsible for this result. Secondary endpoints, such as photoageing and tolerability, indicated superiority of DL-PDT over cryosurgery. A sufficiently powered large-scale trial with a clinically adequate treatment and observation period is needed to further investigate the prophylactic properties of DL-PDT.
The authors thank Monika Schöll for linguistic revision of the manuscript.
This study was financially supported by Galderma Laboratorium GmbH, Düsseldorf, Germany. Metvix 160 mg/g cream and Actinica lotion were provided by Galderma Laboratorium GmbH, Düsseldorf, Germany. Galderma Laboratorium GmbH was neither involved in the design, conduct, and analysis of the study nor in the writing of the manuscript.
Conflicts of interest. SK was a member of advisory boards for Galderma and has participated in previous clinical trials for Galderma. RMS is a member of advisory boards for Almirall, Beiersdorf, Dr. Wolff-Group, Galderma, Janssen and Leo Pharma. He has received speakers’ honoraria and has participated in clinical trials for the aforementioned companies. PAG was a member of advisory boards for Galderma. He has received speakers’ honoraria and research funding and has participated in clinical trials for Asclepion, Beiersdorf, Biofrontera, Boehringer, FB Dermatology, Galderma, Leo, Lilly, and Merz. MK, KKM and FZ received a grant from Biofrontera. WGP-D, WP and ED have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize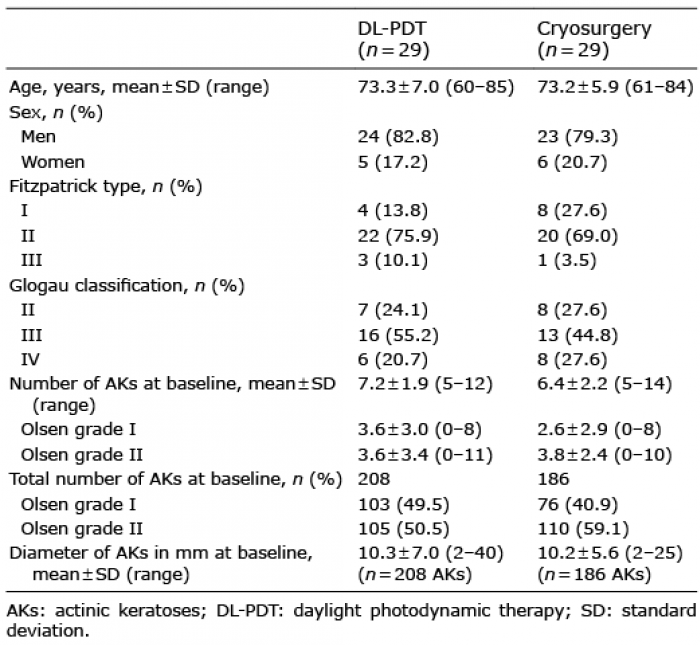 Click to show fullsize
Click to show fullsize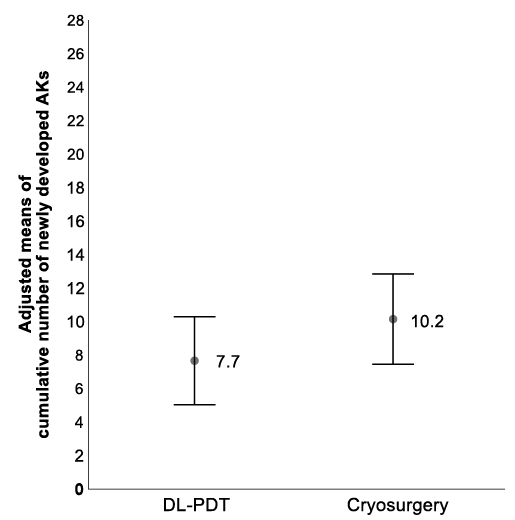 Click to show fullsize
Click to show fullsize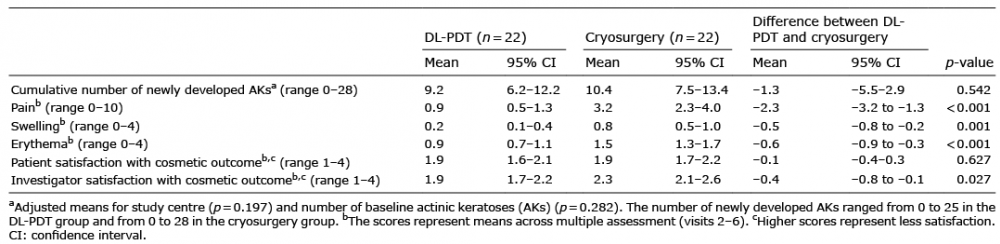 Click to show fullsize
Click to show fullsize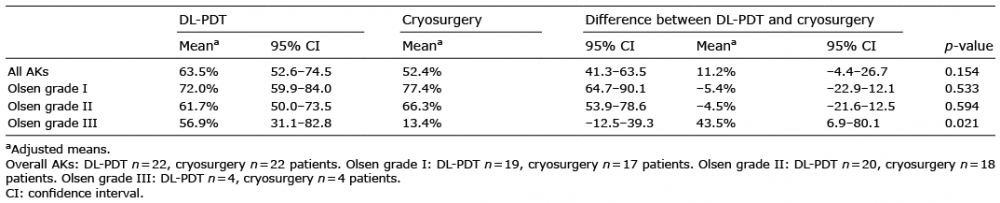 Click to show fullsize
Click to show fullsize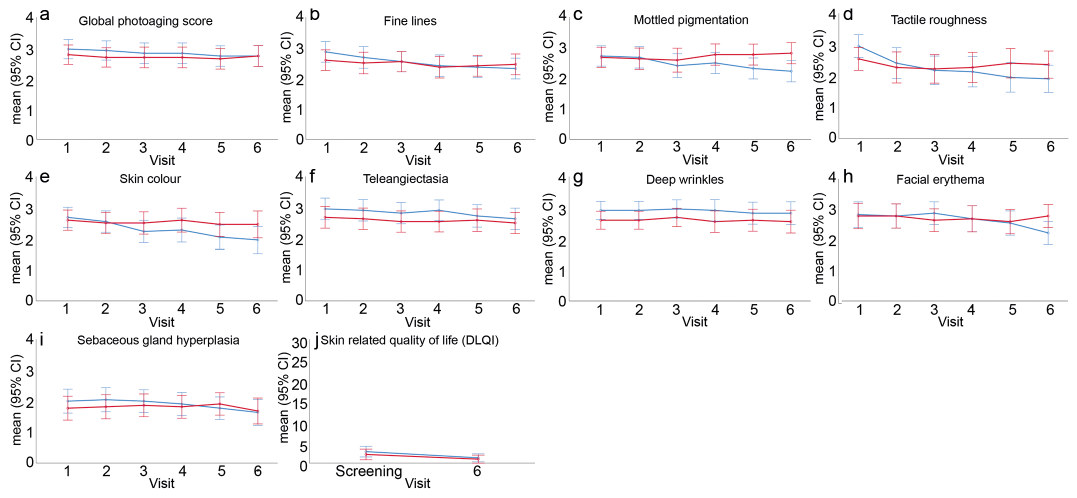 Click to show fullsize
Click to show fullsize