


Department of Dermatology, University of Montpellier and INSERM U1058 “Pathogenesis and control of emerging and chronic infections”, Montpellier, France
Low-dose methotrexate is widely used in mycosis fungoides and Sézary syndrome, but few studies have evaluated this treatment. The aim of this study was to evaluate the benefit/risk ratio of this regimen on skin lesions. A retrospective survey of a series of patients treated for mycosis fungoides or Sézary syndrome with low-dose methotrexate and followed for at least one year in a tertiary referral centre was performed. From a total of 48 patients, complete response and partial response were achieved in 10 (21%) and 25 (52%) patients, respectively, with no significant difference in response rates between mycosis fungoides and Sézary syndrome. Of the responders, 20 out of 35 (57%) relapsed after a median time of 11 months. Forty-four of the total of 48 patients discontinued methotrexate, mainly due to primary or secondary failure and/or limiting toxicity (9 patients). Overall, the benefit/risk ratio of low-dose methotrexate in mycosis fungoides and Sézary syndrome appears favorable and this treatment remains a valid option in mycosis fungoides/Sézary syndrome. However, its activity is limited in duration and significant toxicity may occur in some patients.
Key words: mycosis fungoides; Sézary syndrome; methotrexate; benefit/risk.
Accepted Dec 8, 2020; Epub ahead of print Dec 14, 2020
Acta Derm Venereol 2021; 101: adv00384.
doi: 10.2340/00015555-3719
Corr: Olivier Dereure, Department of Dermatology and INSERM U1058, University of Montpellier, Hôpital Saint-Eloi, 80 avenue Augustin Fliche, FR-34295 Montpellier 5, France. E-mail: o-dereure@chu-montpellier.fr
Most current therapeutic recommendations include methotrexate as a treatment option for early mycosis fungoides, which is the most frequent primary cutaneous lymphoma. However, there are relatively scarce data regarding the clinical efficacy and benefit/risk ratio of methotrexate. We report here our clinical experience of the use of methotrexate in management of mycosis fungoides and Sézary syndrome, with a emphasis on treatment outcome and benefit/risk ratio. A response was obtained in most patients, with a minority of complete responses, but most of the responding patients relapsed after a relatively short time. Limiting toxicity was observed in 19% of patients. Overall, the benefit/risk ratio of methotrexate in mycosis fungoides and Sézary syndrome appears favorable and this treatment remains a valid option in these conditions. However, its activity is limited in duration and significant toxicity may occur in some patients.
Mycosis fungoides (MF) and Sezary syndrome (SS) encompass the majority of primary cutaneous T-cell lymphomas (CTCL), and their practical management along with therapeutic guidelines are updated on a regular basis. A number of therapies are currently available for this group of diseases, organized as different lines of treatment, largely according to clinical stage. Among them, low-dose methotrexate (MTX) is clearly identified as a standard treatment, especially in early MF, and is widely used in daily clinical practice (1, 2). However, only a few retrospective studies have evaluated the benefit/risk ratio of MTX in MF or SS, either as monotherapy or as part of combination therapy, in a significant number of patients (3–15), while no prospective study has been performed to support its use in these two major subsets of CTCL. A monocentre retrospective study was conducted in a tertiary referral centre to further appraise the benefit/risk ratio of low-dose MTX on skin lesions in a series of patients with MF or SS in a real-life setting.
Patient selection and baseline data
All patients over 18 years of age with confirmed MF or SS treated between 2005 and 2017 with low-dose MTX, in monotherapy or in combination for at least one month and followed for at least one year after MTX introduction were included in the study. Identification of patients was based on a computerized epidemiological database through a specific coding (PMSI) for MF or SS. Patients fulfilling the inclusion criteria were identified in a second step. Detailed data from selected patients were then retrospectively collected using electronic medical records from local medical software and anonymized before analysis. The diagnosis was established in all cases on usual clinical and histological grounds and validated by a national expertise network (French Task Force for Primary Cutaneous Lymphoma). Patients were staged upon treatment initiation using the standard tumour-node-metastasis-blood (TNMB) classification system. The study was approved by the local institutional review Board for Ethical Issues of University hospital of Montpellier (file number 2018_IRB-MTP_11-01).
The following baseline characteristics were retrieved from all patients’ files: sex, age, clinical stage at treatment introduction, initial dosage of MTX, therapeutic line, absence/presence of an associated treatment (excluding topical treatments). In addition, patients with MF were divided into 2 histological subsets according to the absence (“classical” MF; cMF) or presence (“annexotropic” MF; aMF) of a histological annexotropism
Survey endpoints
The primary endpoint was the best overall response (BOR) of skin lesions, as clinically evaluated by caring physicians. Clinical response was evaluated using the modified Severity Weighted-assessment Tool (mSWAT) scoring (16) change for patients treated after 2008 and complete response (CR), partial response (PR) and absence of response (NR) were defined as 99–100%, 50–99%, and less than 50% score improvement compared to baseline, respectively, following the internationally consensual definition of clinical end-points and response criteria in MF and SS as reported by Olsen et al. (16). For patients treated before 2008, initial skin response was rated as complete (total or almost total clearance of lesions), partial (clearance of the majority of lesions, but not total disappearance) or unsatisfying, considered as a failure (no response at all or minor response), using a pragmatic response assessment. Secondary endpoints included BOR duration, relapse rate, and time to relapse in initially responding patients, overall duration of treatment, status of MTX at patient’s visit (ongoing treatment vs discontinued) and treatment-related safety data based on the Common Terminology Criteria for Adverse Events (adverse events and serious adverse events resulting, or not, in temporary or permanent discontinuation of treatment). Relapse was defined as the return of skin lesions to baseline pattern regarding extension and clinical subset. Actuarial Kaplan–Meier relapse-free survival curves were built for responding patients, based on overall and disease subset-specific data. Evaluation of the response of non-cutaneous targets (mainly lymph nodes or blood, if applicable) was beyond the primary scope of this retrospective study, which focused on skin response.
Statistical analysis
Initial MTX dosage, response rate, BOR, relapse and time to relapse, status of MTX at last patient’s visit and safety data were compared between a number of predefined clinical subsets (MF vs SS; MF Ia vs Ib; patients experiencing CR vs PR) and between the 2 main histological categories (annexotropic vs non-annexotropic) using Mann–Whitney test, when appropriate, for quantitative data, and Fisher’s exact test for categorical data. As mentioned above, actuarial relapse-free survival curves were built for initially responding patients and compared using the log-rank test between the predefined different disease subsets.
Patients’ baseline characteristics
A total of 48 patients (M/F ratio 33/15; median age at treatment introduction 62 years, age range 22–88 years, Q1–Q3 55–71.5 years) fulfilling the inclusion criteria were included: 28 early MF (15 Ia and 13 Ib), 2 advanced MF (IIb), and 18 SS. Regarding histological subtypes of MF, 19 and 11 patients were identified as cMF and aMF, respectively. Diagnosis was validated by the national expertise network for Primary Cutaneous Lymphoma (Groupe Français d’Etude des Lymphomes Cutanés) in all cases. MTX was first introduced after 2008 in a large majority of patients (42/48, 12.5%) who were evaluated by mSWAT and for whom the therapeutic response was rated according to international criteria (16).
Methotrexate regimen
Low-dose MTX was initially used as systemic monotherapy in 45/48 patients and associated upfront with bexarotene in 3 patients with SS, but topical steroids were intermittently used in parallel in most patients. MTX was implemented as a first-line systemic treatment in half of the patients (24/48), and administered either orally (37/48 patients) or subcutaneously (11/48 patients). Initial weekly dosage of MTX was 10 and 25 mg, with a median initial dosage of 15 mg for MF and 17.5 mg for SS. The treatment was administered on a continuous basis in 41/48 patients (27/30 MF and 14/18 SS) or intermittently in 7 patients, due to limiting side-effects (mainly cytolysis), in a stop-and-resume strategy.
Initial response to low-dose methotrexate
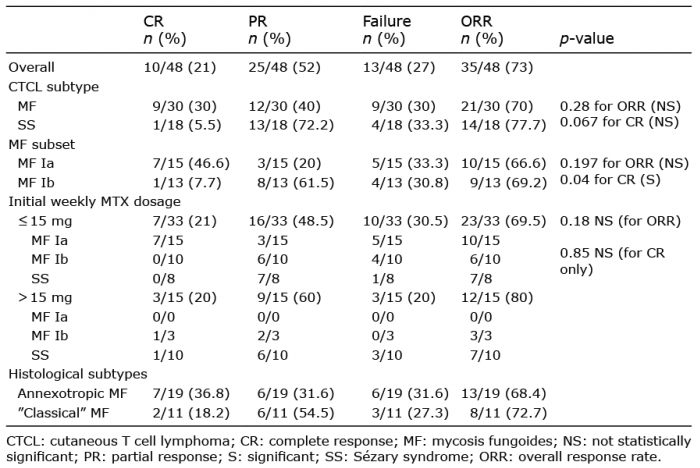
Overall, an initial clinical response was obtained in 35/48 patients (73%), while no significant benefit was observed in 13/48 patients (27%). BOR was identified as CR in 10/48 patients (21%) and PR in 25/48 patients (52%) after a median treatment duration of 3.5 months. Overall response rate (ORR) was not significantly different between MF and SS (70% (21/30) vs 77.7% (14/18), respectively, p = 0.28), but CR was more frequently obtained in MF (CR 30%/PR 40%) than in SS (CR 5.5%/PR 72.2%), with a trend toward significance (p = 0.067). Initial ORR was very close in cMF and aMF (68.4% vs 72.7%), but CR was more often obtained in cMF (36.8%) than in aMF (CR 18.2%). ORR was 66.6% in MF Ia patients vs 69.2% in MF Ib (p = 0.197 not significant (NS)), but CR was observed much more frequently in MF Ia (46.6% vs 7.7%; p = 0.04, significant). No comparison was performed between early and advanced MF, due to the small size of the latter subset (2 patients; one CR and one PR) precluding relevant statistical analysis. ORR was similar in patients treated before and after 2008, who were not evaluated by the same procedure (3/6 and 32/42 responding patients, respectively). Eventually, initial MTX weekly dosage did not seem to significantly influence initial ORR (69.5% (23/33) vs 80% (12/15) with weekly dosage ≤ 15 mg and > 15mg, respectively; p = 0.18 NS) nor achievement of CR (7/33 vs 4/15 respectively; p = 0.85 NS).
The corresponding response data are summarized in Table I.
Table I. Best overall response to methotrexate (MTX) treatment
Relapses and treatment outcome
At least one relapse occurred in 20/35 initially responding patients (57%) after a median time of 11 months after treatment implementation (range 6–72 months; Q1–Q3 8.5–16,75 months) with a corresponding overall median BOR duration of 8 months (range 2–36 months; Q1–Q3 5.25–12 months) (Fig. 1A). In 7 patients relapse persisted despite weekly dosage increase. As a consequence, MTX was permanently discontinued in 19/20 relapsing patients. Treatment was maintained in one patient, with increased MTX dosage in combination with bexarotene, with secondary achievement of PR after initial CR.
Fig. 1. (A) Overall relapse-free survival of responding patients over time (dotted lines: 95% confidence interval). (B) Disease-specific relapse-free survival of responding patients (blue line: patients with mycosis fungoides; red line: patients with Sézary syndrome). (C) Relapse-free survival of responding patients according to quality of initial response (blue line: patients with complete response; red line: patients with partial response). (D) Relapse-free survival of responding patients: influence of initial weekly methotrexate dosage (blue line: ≤15 mg; red line: >15 mg).
Relapses were more frequently observed in patients with SS compared with those with MF, although the difference was not significant (52.4% (11/21) vs 64.3% (9/14) respectively; p = 0.73 NS) and the median time to relapse similar in both conditions (11 months) (Fig. 1B). Conversely, relapses were significantly more frequent in patients with MF Ib compared with Ia (100% vs 20% respectively; p = 0.0007) while a trend toward a significantly lower relapse rate was observed after CR compared with PR (3/10 (30%) vs 17/25 (68%); p = 0.06), along with a significantly longer median time to relapse after CR compared with PR (56 vs 11 months, respectively; p-value (log-rank test) = 0.035) (Fig. 1C). Initial weekly dosage of MTX did not significantly influence relapse rate (65% (15/23) vs 41.5% (5/12) with weekly dosage ≤ 15 mg and >15 mg, respectively; p = 0.16) or median time to relapse (12 vs 15 months; p-value (log-rank test) 0.88) (Fig. 1D).
The overall median total duration of MTX treatment was 10 months (range 1–96 months; Q1–Q3 6.5–24 months) and 18 months for responding patients (range 6–96 months; Q1–Q3 9.5–36.5 months) with no significant difference between MF (18 months) and SS (17.5 months) in this latter subset. Four out of 48 patients were still being treated with MTX at last patient’s visit (3 patients in CR and one patient in PR after CR concomitantly treated with bexarotene). Conversely, MTX was permanently discontinued in the other 44 patients, for various and sometimes combined reasons: protracted CR with no relapse after discontinuation (n = 5), adverse events with no relapse after discontinuation (n = 5), confirmed primary failure after at least 3 months of treatment (n = 11), early limiting toxicity (n = 2), secondary failure with or without limiting side-effects (n = 19) and other reasons (n = 2).
Data related to response and treatment outcome are summarized in Table II.
Table II. Relapse rates and time to relapse after initial response to methotrexate (MTX)
Safety
Side-effects, mainly biological ones, of any type and severity were observed in 19/48 patients (39.5%), including 10 grade 1/2 and 9 protracted or severe grade 2/grade 3 adverse events: abnormal liver tests (5 patients), general status degradation (4 patients), asthaenia/cytopaenia (4 patients), interstitial pneumopathy (2 patients), neurological symptoms (1 patient) and early acute pancytopaenia (1 patient). In addition, a MTX-induced primary cutaneous diffuse large B-cell lymphoma was diagnosed in 2 patients with SS. As mentioned above, side-effects led to transient discontinuation of treatment for one or several short period(s) in 7/35 initially responding patients, mostly due to mild and fluctuating liver toxicity. Conversely, protracted or serious side-effects resulted in permanent discontinuation of MTX in 9/48 (18.75%) patients, including 2 with early limiting adverse events (general status degradation and possible central neurological toxicity).
Low-dose MTX has long been used in CTCL therapeutic strategies and is a recommended treatment in updated guidelines, even though specific market-access labelling is absent in most countries for this indication (1, 2). However, to date, only a small number of retrospective evaluations have been conducted to assess the benefit/risk ratio of low-dose MTX as a systemic monotherapy in MF and SS. The usefulness of MTX in CTCL was first mentioned in 1964, when Wright et al. (3) successfully treated MF with single daily doses with better results compared with other immunosuppressive agents, such as chlorambucil. Other reports from retrospective series published in subsequent years confirmed the activity of the molecule in monotherapy in this setting (4–6), with response rates as high as 82%, the best result obtained among 8 commonly used chemotherapeutic agents (5). In 1989, Zackheim & Epstein (7) reported a retrospective series of 17 patients with SS treated with low-dose MTX (10–50 mg weekly) with an ORR of 76%, including 41% of CR, along with encouraging safety data (6% of limiting toxicity). Responses were protracted, with 71% of patients still in PR or CR for at least 3 years and 35% for at least 5 years. A few years later the same authors further reported similar favourable results on a retrospective series of 29 patients with erythrodermic CTCL, with an ORR of 58%, a majority of CR (41%) (8) and a median “freedom from treatment failure” of 31 months. Median overall survival was 8.4 years. Tolerance was also good, with only 2 patients experiencing side-effects resulting in treatment discontinuation. Another cohort of 69 patch/plaques and tumour-stage patients with MF, mainly with T2 disease and treated with low-dose MTX (10–50 mg/week; median dose 25 mg/week) was subsequently reported by Zackheim et al. (9), but ORR was lower than in erythrodermic patients with CTCL (34%, including 12% CR and 22% PR, with a higher response rate in early-stage disease compared with tumour stage (response rate 14%)). Median time to treatment failure was 15 months for responding patients. Significant toxicity, resulting in permanent treatment interruption, was reported in 6 (9%) patients. Since then, only 2 other retrospective reports have further investigated the specific activity of MTX in monotherapy in CTCL. In a comparative study of MTX (15–50 mg/week, mean 30 mg) vs interferon-alpha (IFN-α) in 21 stage Ia–IV CTCL (MF either folliculotropic or not and SS), initial ORR was significantly higher with IFN than with MTX (87% vs 47% after a median time of 2 and 3 months, respectively). Erythrodermic patients did not properly respond to MTX, but this subset included only 3 patients (10). MTX-related adverse effects were observed in 9/19 (47%) patients. In a larger cohort of 79 MF of all stages receiving MTX (5–50 mg/week, median 20 mg) final ORR was 75% and rated higher in stage II–IV vs stage I although no data were available regarding CR/PR ratio. Median relapse-free survival was between 4 and 6 months for responding patients; longer in patients receiving a higher dosage of MTX (11). Adverse events were not specified. Eventually, other reports investigated the activity of low-dose MTX combined with other first-line drugs, mainly IFN, retinoids and bexarotene, with ORR and CR as high as 80% and 74%, respectively, and overall minimal or mild toxicity (12–14).
Direct cross-comparisons between previous reports and between these reports and the present series regarding clinical results have low relevance, due to a high degree of discrepancy as to weekly MTX dose, follow-up duration and methodology with a special mention for response definition and evaluation tools, which are unspecified in most reports. The current study, based on 48 patients affected by 2 major subsets of CTCL (MF and SS), is the third largest study to evaluate low-dose MTX activity in this setting after studies by Olek-Hrab et al. (11) (79 patients) and Zackheim et al. (9) (69 patients), but the only one to clearly define the different subsets of clinical response. ORR observed in the current series (73%) is in line with most prior studies reporting an ORR between 50% and 80% regardless of CTCL subset and MTX dosage, with the notable exception of the series of 69 patients with MF reported by Zackheim et al. (9) (34%). In the present study, ORR was similar in non-erythrodermic and erythrodermic patients, with no significant difference between clinical and histological (classical vs annexotropic) subsets in patients with early MF; data reminiscent of the series of Wain et al. (10), in which no difference in ORR was observed between classical (56%) and folliculotropic (66%) MF. Conversely, CR was significantly more frequently achieved in very early stages (Ia) and in non-annexotropic MF, with a trend to a higher CR/PR ratio in MF vs SS; data not specifically highlighted in previous reports. The much higher rate of achievement of total control in very early stages (50% vs 7.7% in stages Ia and Ib, respectively) is probably related to a lower tumoural burden, but might also be partially explained by other therapeutic factors, including an easier and more steady use of topical steroids on limited lesions, even though a sustained response is more likely to be assigned to the systemic treatment.
Relapse rate and time to relapse are also important issues to consider in these chronic and relapsing diseases, but such data are only minimally available in previous reports. In the current series 57% of responding patients relapsed after a median treatment duration of 11 months; data less favourable than in the 2 cohorts of erythrodermic CTCL treated by Zackheim et al. (7, 8), but more consistent with the median time to treatment failure (15 months) observed by the same authors in MF, and very close to the disease progression rate reported by Wain et al. (10) (58%). In addition, the only parameters clearly related to relapse were MF stage (more frequent in stage Ib) and, to a lesser extent, the level of initial response. Eventually, Olek-Hrab et al. (11) reported a median relapse-free survival of 4–6 months in MF; relatively close to data of the current series (median BOR duration 8 months). Overall, it appears that when a clinical response is achieved it is maintained for less than one year in most patients.
In most reports, including the current series, tolerance data appear favourable, with the usual and expected MTX-related side-effects. These adverse effects were described as limiting in 6–9% of patients in previous reports by Zackheim et al. (7–9), and resulted in permanent discontinuation of treatment in approximately 19% of patients in the current series. In other cases, they may lead to transient interruption(s) followed by subsequent resumption(s) of the treatment, with possible dosage modulation, in an on/off strategy. A role of MTX in large cell lymphoma transformation has been considered by some authors, but with no definite evidence and such reports remain scarce (15).
The mechanism of action of low-dose MTX in CTCL is unknown. Direct antiproliferative activity seems unlikely, owing to the low dose of the molecule and to the lack of a high proliferative rate of neoplastic cells in early MF. Conversely, modulation of expression of a number of genes after exposure to MTX has been well documented in CTCL; most notably an increase in Fas/Fas ligand expression, resulting in improved sensitivity of neoplastic cells to apoptosis (17–19). This upregulation, reminiscent of the mechanism of action of histone deacetylase inhibitors, which are another class of drugs active in CTCL, may be related to epigenetic modulation of target genes. Supporting this hypothesis, a reduction of Fas promoter methylation (19) has been documented with MTX exposure, probably an indirect consequence of intracellular MTX detoxification that requires methylation of the molecule. Accordingly, a high level of pre-treatment methylation of the promoter region of some genes involved in CTCL pathomechanisms, through modulation of the response to apoptotic stimuli, might be used in the future as a predictive biomarker of MTX activity in CTCL.
In conclusion, low-dose MTX appears to display a favorable benefit/risk ratio in both early MF and SS, but its activity remains limited in duration, and a significant proportion of patients appear to be primarily resistant, emphasizing the need to develop biomarkers predictive of efficacy. It would be of interest to further research a topical form of the molecule, the development of which has not been pursued following an initial study (20).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize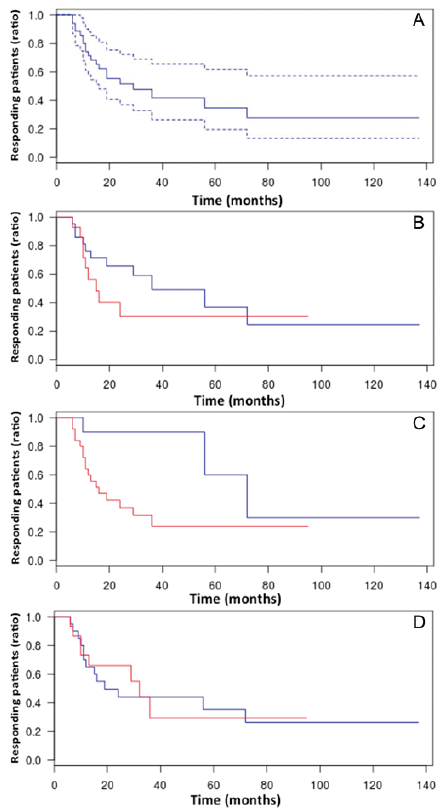 Click to show fullsize
Click to show fullsize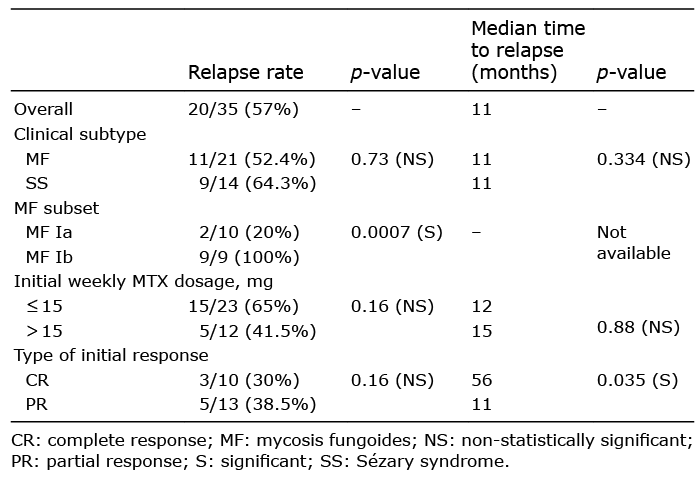 Click to show fullsize
Click to show fullsize