


1Department of Dermatology and Venereology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, 2Region Västra Götaland, Sahlgrenska University Hospital, Department of Dermatology and Venereology, Gothenburg, Sweden, and 3Clinical Pharmacology and Pharmacy, Department of Public Health, University of Southern Denmark, Odense, Denmark
An association between methotrexate use and risk of cutaneous squamous cell carcinoma has been reported in patients with rheumatoid and psoriatic arthritis. A nested case-control study was performed to investigate if methotrexate use among patients with psoriasis was associated with increased risk of cutaneous squamous cell carcinoma. Data were obtained from Swedish registers and included 623 patients with psoriasis and a first cutaneous squamous cell carcinoma from 2010 to 2016. Ten randomly selected patients with psoriasis were matched on age and sex to each case. Among cases, 160 (26%) were ever-users of methotrexate. The corresponding number among the controls was 1,370 (22%), yielding an unadjusted odds ratio (OR) of 1.23 (95% confidence interval (95% CI) 1.02–1.49); p = 0.034. After adjusting for use of other immunosuppressive drugs the association was close to unity (OR 1.09; 95% CI 0.89–1.34); p = 0.39. The slightly increased risk of cutaneous squamous cell carcinoma associated with methotrexate-exposure in patients with psoriasis does not seem to be associated with methotrexate, but rather with disease severity, other anti-psoriatic treatments, and ultraviolet exposure.
Key words: adverse effects; epidemiology; methotrexate; pharmacology; psoriasis; squamous cell carcinoma.
Accepted Dec 14, 2020; Epub ahead of print Dec 15, 2020
Acta Derm Venereol 2021; 101: adv00365.
doi: 10.2340/00015555-3725
Corr: Sam Polesie, Department of Dermatology and Venereology, Institute of Clinical Sciences, Sahlgrenska Academy, University of Gothenburg, Gröna stråket 16, SE-413 45 Gothenburg, Sweden. Email: sam.polesie@vgregion.se
Squamous cell carcinoma is the second most common type of skin cancer. This study investigated whether use of methotrexate was linked to increased risk of such cancer, using a database of Swedish patients with psoriasis. Among these, patients who developed squamous cell carcinoma were identified and their use of methotrexate compared with cancer-free patients. Patients with squamous cell carcinoma were more likely to be users of methotrexate compared with cancer-free psoriasis controls. However, when the use of other immunosuppressive drugs was taken into account, use of methotrexate was no longer linked to an increased risk of squamous cell carcinoma.
Immunosuppressive drugs increase the risk of skin cancer, particularly keratinocyte carcinoma (1). Methotrexate (MTX) is an old immunosuppressive and anti-inflammatory drug that has frequently been used for several immune-mediated diseases, including psoriasis, since its introduction more than 70 years ago (2). Use of MTX has been linked with a higher risk of cutaneous squamous cell carcinoma (cSCC) and basal cell carcinoma (BCC) among patients with rheumatoid arthritis (RA) and psoriatic arthritis (PsoA) (3). In a cohort of American patients with RA, use of MTX over one year was associated with an enhanced risk of a second non-melanoma skin cancer (NMSC) (4). In another investigation conducted within a cohort of patients with psoriasis, MTX treatment was linked with an increased risk of BCC but not cSCC (5). In Swedish investigations, hospitalized patients with psoriasis were more likely to develop NMSC including cSCC, compared with the general population (6, 7). In a meta-analysis the relative risk (RR) for cSCC among individuals with psoriasis compared with population-based controls and cohorts was 2.15 (95% confidence interval (95% CI) 1.32–3.50) (8). In a recent systematic review and meta-analysis patients with psoriasis had an increased risk of keratinocyte carcinoma compared with population controls (RR 2.28, 95% CI 1.73–3.01). This association was not observed in patients with PsoA (RR 1.22, 95% CI 0.89–1.66) (9).
In the Cardiovascular Inflammation Reduction Trial (CIRT) the role of MTX treatment for prevention of a new cardiovascular event in patients with stable atherosclerosis was assessed (10). The trial included 4,786 North American patients (81.2% men, median age 65.7 years) randomized to receive either low-dose MTX (n = 2,391) or placebo (n = 2,395). Patients randomized to MTX treatment did not have a lower risk of a subsequent cardiovascular event. However, when the proportion of adverse events in both groups was compared, a significantly increased risk of skin cancer was observed among patients randomized to MTX treatment. For cSCC, 33 cases (1.4%) were reported among the MTX exposed and 10 cases (0.4%) in the placebo group, yielding a hazard ratio (HR) of 3.31 (95% CI 1.63–6.71) (11). Notably, this difference was observed within a median follow-up period of 23 months. Nevertheless, patients with any immune-mediated disease, which is the actual label for MTX, were not included, since any chronic inflammatory condition was listed as an exclusion criterion. Expanding our knowledge of potential side-effects for old pharmaceuticals is important, particularly those used by millions of patients worldwide, such as MTX. Therefore, the aim of this Swedish nested case-control investigation was to further analyse the association between MTX use among patients with psoriasis and cSCC.
Cohort
The specific Swedish psoriasis cohort definition and detailed information about the registries used have been described previously (12). Briefly, the cohort consists of 81,738 patients with psoriasis. To allow for an adequate exposure assessment window (the drug prescription registry was initiated in July 2005), patients with an incident cSCC (including cutaneous squamous cell carcinoma in situ (cSCCis)) during the period 2010 to 2016 were selected (cases). Prior to the date of the cSCC diagnosis, the cases needed to be cancer-free with the exception of BCC. All cSCC were identified through combining International Classification of Diseases, Tenth Revision (ICD-10) and the morphology codes for International Classification of Diseases for Oncology, third edition (ICD-O/3). The exact definitions are available in the supplementary material (Table SI).
The date of the cSCC diagnosis was used as the matching date for the controls (index date). Eligible controls needed to be alive and cancer-free on the index date and were matched for age (same birth year) and sex. Risk set sampling was used as the matching strategy (13). All patients needed to reside continuously in Sweden from July 2005 to the index date. Patients with any International Classification of Diseases (ICD) code indicating a previous organ transplant surgery and/or HIV were discarded if the diagnosis antedated the index date. Ethical approval was obtained from the Swedish Ethical Review Authority (approval number 2020-01839).
Exposure
Exposure to MTX was based on filled prescriptions recorded in the Swedish Prescription Registry. The main exposure of interest was defined as ever-use of MTX, while cumulative doses were analysed in supplementary analyses to assess dose response. Exposure to MTX was assessed from data availability (July 2005) until the index date. Accumulated MTX doses to the index date (in g) were obtained.
Covariates
The Charlson Comorbidity Index was obtained for all patients to adjust for comorbidity at large (14). Furthermore, conditions that are considered prior to MTX prescription and other formal indications for MTX were obtained. Specifically, alcohol-associated conditions, diabetes, liver diseases, renal diseases, peptic and duodenal ulcers, smoking-associated conditions, actinic keratosis, Crohn’s disease, RA and PsoA were included as covariates (Table SI).
Primary analysis
In the main analysis, association between ever-use of MTX and cSCC was examined with conditional logistic regression models, adjusting for relevant comorbidities and immunosuppressive drugs.
Secondary analyses
(i) The filled MTX doses used before the index date were summarized and per oral and subcutaneous doses, as well as totally accumulated doses, were assessed as a continuous variable. Moreover, totally accumulated MTX doses were analysed separately as a categorical variable.
(ii) Analyses of the association between cSCC and ever-use of ciclosporin, acitretin, azathioprine, tumour necrosis factor α inhibitors (TNFis) and interleukin pathway-inhibitors (ILis).
(iii) Mortality analyses, investigating overall mortality between cases and controls and MTX-exposed and MTX-unexposed within the case group.
Sensitivity analysis
Three sensitivity analyses were conducted. First, to examine the potential for reverse causation or protopathic bias, different lag periods (period before the index date that is disregarded with respect to filled MTX prescriptions) were introduced. In the second analysis, the case group only included patients with an invasive cSCC and their respective controls. In the final sensitivity analysis, the study inclusion criteria for cases and controls were changed. In this analysis prevalent cancers (other than cSCC or cSCCis) were permitted prior to the index date. For the 2 last sensitivity analyses, the primary and all secondary analyses were repeated.
Post hoc analysis
To examine the impact of potential confounding by UV exposure, a post hoc analysis restricted to individuals without a history of actinic keratosis was conducted. To this end, an updated risk set sampling was used, in which only cases and controls without a previous history of actinic keratosis before the index date were included, and the primary and secondary analyses were repeated in this population.
Statistical analysis
Conditional logistic regression models were used, with cSCC as the dependent variable and MTX as the independent variable. Cox proportional hazards regression models were adjusted for age group (≤ 40, > 40–≤ 50, > 50–≤ 60, > 60–≤ 70 and > 70 years) and sex. Kaplan–Meier survival plots were performed as mortality analyses. In all models, drugs and comorbidities refers to registered events before index date. Fisher’s exact test and Wilcoxon’s rank sum test were used for comparing proportions and 2-sample tests, respectively. All tests were 2-sided and p < 0.05 was considered as statistically significant. All data were analysed using R version 3.5.3 (https://www.r-project.org/).
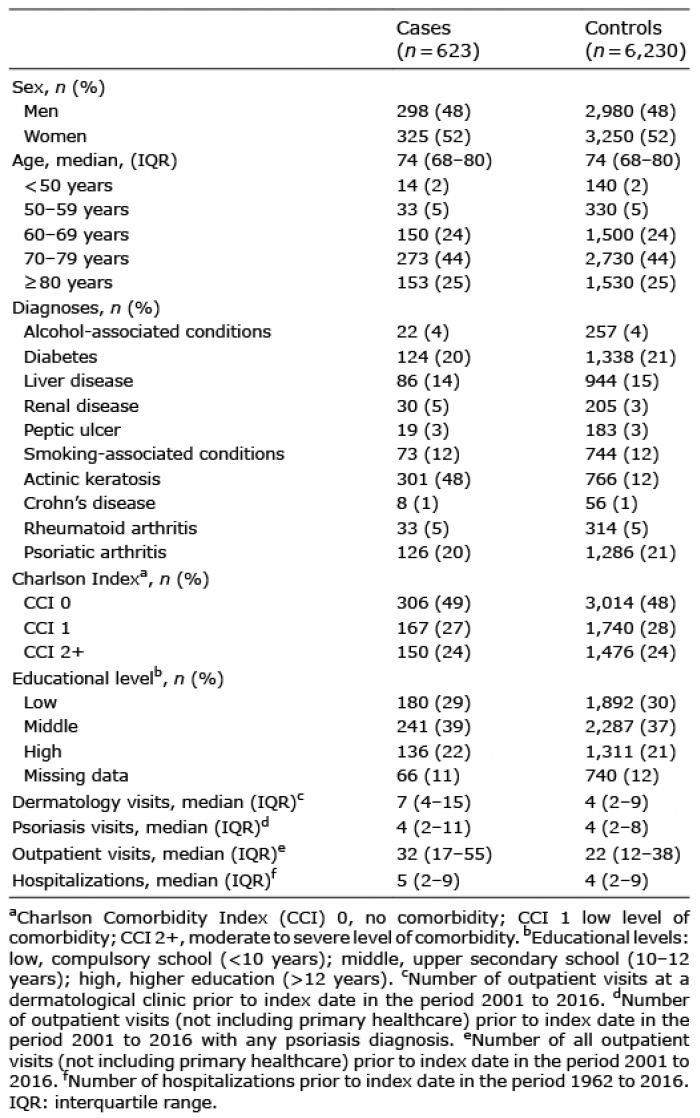
In total, 623 patients with psoriasis (52.2% women) with a first cSCC, including cSCCis (n = 314) were identified (cases) during 2010 to 2016. A total of 6,230 patients with psoriasis were sampled as controls (Fig. S1). The majority (95.0%) were born in any of the Nordic countries. Except for renal diseases and actinic keratosis, which were more prevalent in the case group (p = 0.050 and p < 0.0001), comorbid conditions were distributed similarly among cases and controls. The cases had more visits to a dermatology clinic (p < 0.0001), visits related to psoriasis (p = 0.0007) and outpatient visits (p < 0.0001) compared with controls (Table I). The median time (interquartile range (IQR)) from the first available diagnosis of psoriasis to the index date among the cases was 7.7 years (3.7–10.7 years). The corresponding time for the controls was 7.4 years (3.8–10.5 years; p = 0.43).
Table I. Demographic data
When investigating all filled MTX prescriptions among cases and controls, 45%, 31%, 9%, 6% and 9% were prescribed by dermatologists, rheumatologists, internists, general practitioners and other physicians, respectively. Fig. S2 illustrates the summarized MTX doses for MTX-exposed cases and controls. The time from first to last filled prescription of MTX was 3.0 years for both groups combined and did not differ significantly between the groups. The median time (IQR) from a first prescription of MTX to the index date was 5.8 years (3.2–8.2) for the cases and 5.5 years (2.9–7.8) for the MTX-exposed controls (p = 0.28).
Primary analysis
Among the cases and controls, 160 patients (26%) and 1,370 (22%) had filled any MTX prescription. A univariate conditional logistic regression model, using ever exposure of MTX, yielded an OR of 1.23 (95% CI 1.02–1.49; p = 0.034) for ever use of MTX associated with cSCC. When adjusting for TNFis and immunosuppressants other than MTX, the confidence intervals overlapped 1; however, the point estimates were similar to the above result. In univariate analyses for the covariates associated with cSCC, actinic keratosis was strongly associated with cSCC (OR 7.77, 95% CI 6.43–9.41; p < 0.0001) (Fig. 1). In a complementary analysis, the effect on the OR for MTX associated with cSCC after adjusting for each covariate separately are shown (Table II).
Fig. 1. Odds ratios. 95% CI: 95% confidence interval; cSCC: cutaneous squamous cell carcinoma including squamous cell carcinoma in situ; MTX: methotrexate; OR: odds ratio; PsoA: psoriatic arthritis; TNFi: tumour necrosis factor α inhibitor.
Table II. Confounding analysis
Secondary analyses
(i) A trend for an increased risk of cSCC with increasing doses of accumulated MTX was observed. When modelling dose as a continuous variable, the risk of cSCC increased significantly with per oral and total dose of MTX (Table III).
Table III. Methotrexate (MTX) doses among cases and controls and dose-response analysis
(ii) Filled immunosuppressive drugs other than MTX, azathioprine and TNFis were more frequent among cases compared with controls. The distribution of ever-use of drugs and drug classes are shown in Table IV.
Table IV. Ever-use of drugs and drug classes among cases and controls
(iii) There were no differences in mortality rates between cases and controls (adjusted HR 1.0, (95% CI 0.7–1.2); p = 0.71). When MTX-exposed and MTX-unexposed cases were compared no difference in mortality was observed (Fig. S3).
Sensitivity analyses
Altering the lag periods had no impact for the main analysis (Table SII). When the case group was restricted to those patients with invasive cSCC (n = 309) and their respective controls (n = 3,090) previous associations were preserved (Tables SIII and SIV). In the final sensitivity analysis, the case and control group included patients who also could have had previous malignancies (other than cSCC or cSCCis) prior to index date. For this separate investigation, a new risk set sampling was performed and this analysis included 878 cases (47.5% men) and 8,780 controls. The results of the primary and secondary analyses echoed in this separate investigation (Tables SV and SVI).
Post hoc analysis
In the post hoc analysis including patients without a history of actinic keratosis, 28.6% (92 of 322) and 22.5% (726 of 3,220) of cases and controls had any MTX use, which yielded a crude OR of 1.38 (95% CI 1.07–1.78; p = 0.014). The results of the primary and secondary analyses were preserved in this analysis (Tables SVII and SVIII).
This Swedish nested case-control study, demonstrated an association between use of MTX among patients with psoriasis and cSCC. Moreover, a trend for a dose-response association was seen. However, the association was no longer significant when adjusting for ever-use of TNFis or immunosuppressants other than MTX.
The results from the current study may support the findings in the CIRT, which showed an enhanced risk of cSCC among patients exposed to MTX (10, 11). Even though this randomized and double-blinded prospective trial had optimal design to investigate whether MTX reduced the risk of cardiovascular events, it was not devised to detect differences in adverse events specifically skin cancer. Therefore, it is interesting that the authors were able to detect a significantly higher risk of cSCC among those patients randomized to MTX treatment compared with those randomized to placebo. While the results are important to the scientific community at large, it is essential to underline that no patients with inflammatory diseases were included in the CIRT. This raises the question as to whether the results are generalizable to patients in whom MTX is used clinically (15). Furthermore, the accumulated doses for the case group were not presented in the CIRT and the study mainly included men (81.7%), compared with the current investigation, in which the sex distribution was equal (47.8% men). Moreover, the patients included were younger at inclusion compared with our investigation (median age 65.7 vs 73.7 years). The present study had a median follow-up time of 5.6 years. While this can be considered short, in the CIRT an increased risk of cSCC was observed within a median time of less than 2 years (23 months).
To address the results from the recent systematic review and meta-analysis by Vaengebjerg et al. (9), the current study adjusted for PsoA in the primary analysis. Adjustment for PsoA did not influence the OR of cSCC with respect to MTX. The association between MTX and cSCC was no longer statistically significant when the analysis was adjusted for use of TNFis. Previous studies show conflicting results on the impact of biologic agents on incident cSCC. In a Swedish cohort investigation consisting of patients with RA (n = 12,558), use of TNFis was associated with an increased risk of cSCC (including cSCCis) compared with biologics-naive patients (adjusted HR 1.43, 95% CI 1.22–1.69) (16). In the meta-analysis by Vaengebjerg et al. (9), including 13 investigations, biologic agents did not increase the risk of keratinocyte carcinoma compared with treatment with conventional therapies in patients with psoriasis (RR 0.91, 95% CI 0.64–1.30).
In the case definition for the primary and secondary analyses, the current study included cSCCis. Experienced dermatologists can often identify these lesions clinically and therefore these tumours are not always sent for pathology report. Therefore, it is expected that the number of cSCCis is underestimated in both groups. Moreover, among patients with psoriasis, it may be challenging to distinguish cSCCis from psoriasis plaques. In this context it is also worth mentioning that patients treated with MTX might have clearer skin, which, intrinsically, may facilitate detection of cSCC. Using that line of argument, MTX use per se could result in detection bias and possibly an exaggerated OR. Nonetheless, our results were robust when we only restricted the case group to those with invasive cSCC, which are typically more conspicuous lesions and thus more easily detected both by the patient and physician, regardless of the presence or absence of psoriatic plaques. Allowing any prevalent cancer, other than cSCC, prior to the index date among cases and controls did not impact the results.
This investigation has some limitations. Due to the retrospective design, important risk factors for cSCC including detailed data on sun exposure and UV radiation could not be obtained. Light therapies, including narrow-band UVB (nbUVB) and psoralen plus UVA, both of which have been associated with an enhanced risk of cSCC, in both American and European investigations (17–20), are not included in the Swedish healthcare registries. Nevertheless, in a Swedish cross-sectional investigation, the skin cancer risk of patients with psoriasis treated with nbUVB was not higher than the general population (21). While there is only a limited number of investigations conducted, nbUVB therapy for patients with psoriasis does not seem to increase the risk of cSCC (22–25). Having said that, confounding by UV-radiation, both due to lifestyle factors and light therapy, cannot be excluded. The presence of actinic keratosis is generally considered as an indicator of chronically sun-damaged skin and, hence, cumulative sun exposure. In a recent Swedish cohort investigation including 2,983 patients with actinic keratosis and 14,668 age- and sex-matched patients without such a disease, a HR of 7.7 (95% CI 6.7–8.8) for cSCC was observed (26). In a post hoc analysis, we examined whether the findings persisted after excluding patients with actinic keratosis. The findings from this separate analysis were in line with the primary and secondary analyses, indicating that confounding due to UV exposure may be limited. Of note, since BCC is not included in the Swedish cancer registry, it was not included in our analysis. Therefore, future investigations including both cSCC and BCC are encouraged.
All data in the Swedish registers are prospectively added. Consequently, we acknowledge that other study designs addressing this specific question could have be chosen. An alternative approach would be the active comparator design (i.e. patients with psoriasis who fill prescriptions of MTX could be compared with those who receive another systemic treatment, such as ciclosporin, TNFis or acitretin). This design would allow comparison of different drugs and would position MTX to other drugs with respect to the risk of cSCC. On the other hand, in Sweden, ciclosporin is rarely selected as an anti-psoriatic treatment, and patients dispensed with biological treatments in Sweden most often have a history of MTX use, making it difficult to exclude an additive effect. Finally, since acitretin might lower the risk of cSCC (27, 28), the active comparator design would also have intrinsic weaknesses.
Strengths of this investigation are that it includes cSCCis, which is infrequently included in observational investigations. Since inclusion of in situ carcinomas in national cancer registries is a rare event, it is important to underline that the results were robust when only considering those patients with invasive cSCC as cases. Moreover, the study is conducted within a cohort of patients with psoriasis, which minimizes the risk of confounding by indication. Furthermore, dermatological follow-up for patients with psoriasis includes a total-body examination, meaning that the risk of surveillance bias is diminished. However, even after nesting the cohort in patients with psoriasis, we observed that cases had more visits to a dermatology clinic, visits related to psoriasis and outpatient visits compared with controls. Thus, arguably the cases most likely had higher disease severity and were examined more frequently than controls.
In conclusion, while the results of the current study suggest an increased risk of cSCC associated with use of MTX among patients with psoriasis in a dose-response pattern, it is important to underline that, when the current analysis was adjusted for TNFis or other immunosuppressants, the association was no longer significant. Thus, the key message to practicing dermatologists is that the slightly increased risk of cSCC associated with MTX may be due to confounding by disease severity, other anti-psoriatic treatments, and UV exposure. While a theoretical increase in risk cannot be excluded, it is probably not significant for the dermatologist in everyday clinical practice.
The authors have no conflicts of interest to declare.
 Figure S1 Table SI Figure S2 Figure S3 Table SII Table SIII Table SIV Table SV Table SVI Table SVII Table SVIII
Figure S1 Table SI Figure S2 Figure S3 Table SII Table SIII Table SIV Table SV Table SVI Table SVII Table SVIII

 Click to show fullsize
Click to show fullsize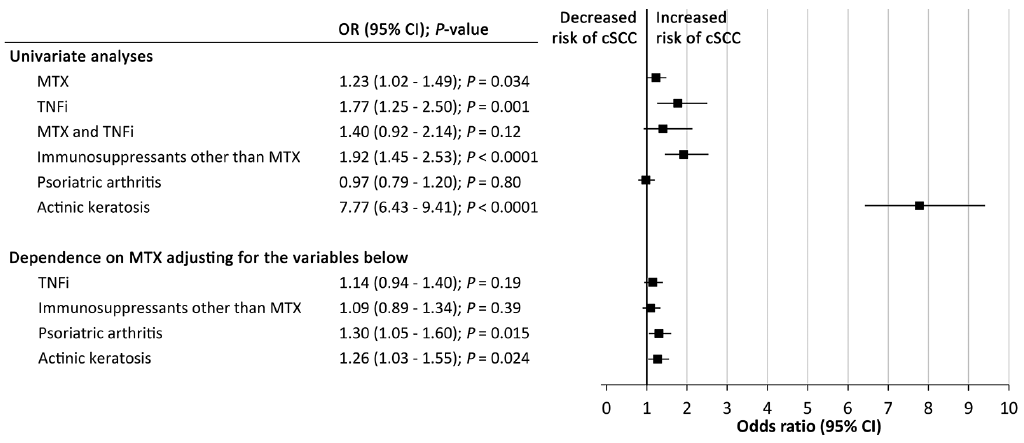 Click to show fullsize
Click to show fullsize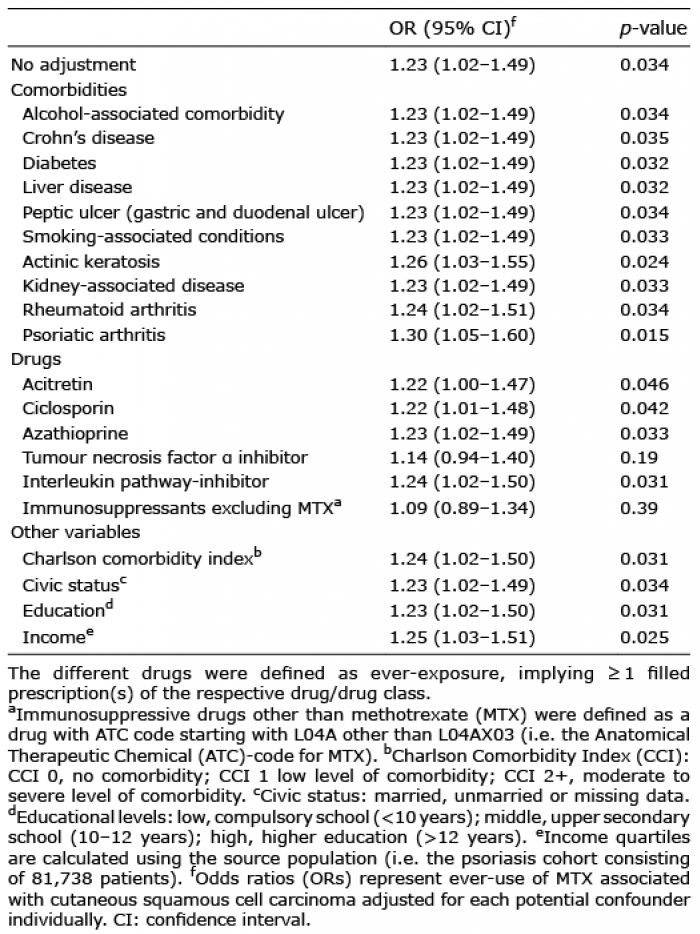 Click to show fullsize
Click to show fullsize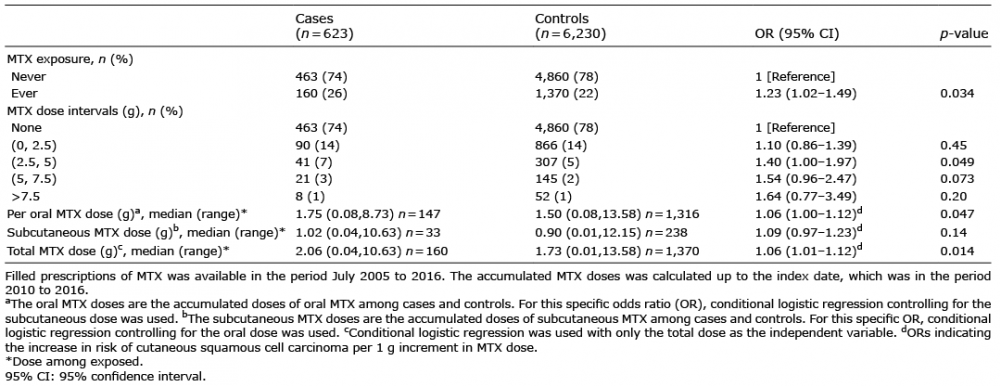 Click to show fullsize
Click to show fullsize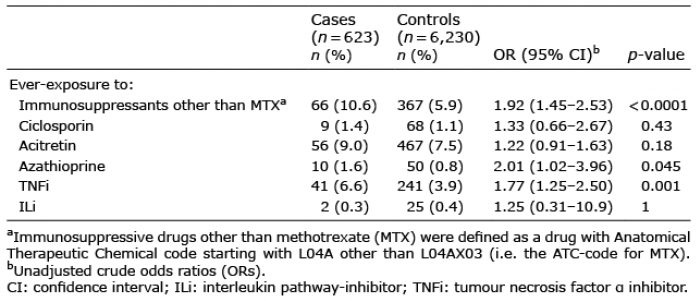 Click to show fullsize
Click to show fullsize