


1Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Münster, Germany, 2Department of Clinical Sciences Lund, Dermatology and Venereology, Lund University, Lund Sweden and Skåne University Hospital, Lund, Sweden, 3Department of Dermatology, Oslo University Hospital, University of Oslo, Oslo, Norway, 4Department of Social Medicine, Occupational and Environmental Dermatology, University of Heidelberg, Germany, 5Fondazione Policlinico Universitario A. Gemelli IRCCS, Dipartimento di Scienze Mediche e Chirurgiche, UOC Dermatologia, Università Cattolica del Sacro Cuore, Rome, Italy, 6Department of Dermatology, University Hospital of Brest, Brest, France, 7Department of Dermatology, Ayd?n Adnan Menderes University, Ayd?n, Turkey, 8Moscow Scientific and Practical Center of Dermatovenereology and Cosmetology, Moscow, Russia, 9Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, 10Department of Dermatology, University of Rzeszów, 11Department of Dermatology, School of Medicine, University of Information Technology and Management, Rzeszów, Poland, 12Department of Dermatology, Medical University of Graz, Graz, Austria,13Department of Dermatology and Allergy, Charité – Universitätsmedizin Berlin, Berlin, Germany, 14Department of Dermatology, Kantonsspital Aarau, Aarau, Switzerland, 15Department of Dermatology, Sant Pau Hospital, Barcelona, Spain, 16Department of Dermatology, University Hospital and Faculty of Medicine, University of Coimbra, Coimbra, Portugal, 17Institute of Medical Informatics, University of Münster, Münster, and 18Competence Center for Healthcare Research in Dermatology (CVderm), Institute for Healthcare Research in Dermatology and Nursing (IVDP), University Hospital of Hamburg-Eppendorf, Hamburg, Germany
#Shared first-authorship.
*EPP Consensus Conference Participants 2017: Florence Dalgard, Malmö, Sweden; Jesper Elberling, Copenhagen, Denmark; Caroline Forner, Münster, Germany; Uwe Gieler, Giessen, Germany; Tabi A. Leslie, London, UK; Claudia Riepe, Münster, Germany; Gudrun Schneider, Münster, Germany; Hartmut Ständer, Bad Bentheim and Dortmund, Germany
Chronic nodular prurigo is characterized by recalcitrant itch. Patient perspectives on therapeutic goals, satisfaction with therapy and efficacy of therapeutic regimens for this condition are unknown. This questionnaire study examined these issues in 406 patients with chronic nodular prurigo from 15 European dermatological centres. Improvements in itch, skin lesions and sleep were the most important goals. Emollients, topical corticosteroids and antihistamines were the most frequently used treatments, while a minority of patients were prescribed potent medications, such as systemic immunosuppressants and gabapentinoids. Most patients were not satisfied with their previous therapy (56.8%), while 9.8% did not receive any therapy despite having active disease. A substantial number of respondents (28.7%) considered none of the therapeutic options effective. Although chronic nodular prurigo is a severe disease, most patients were not treated with potent systemic drugs, which may contribute to the high levels of dissatisfaction and disbelief in available therapies. Specific guidelines for chronic nodular prurigo and the development of novel therapies are necessary to improve care.
Key words: nodular prurigo; chronic nodular prurigo; patient-reported outcome; itch; pruritus; therapy.
Accepted Dec 14, 2020; Epub ahead of print Dec 15, 2020
Acta Derm Venereol 2021; 101: adv00403.
doi: 10.2340/00015555-3726
Corr: Manuel P. Pereira, Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: manuelpedro.pereira@ukmuenster.de
Chronic prurigo is a highly impairing itchy skin disease, which is difficult to treat. This questionnaire study of 406 patients with active disease at 15 centres across 12 European countries revealed that improvements in itch, skin lesions and sleep are the most important goals for patients. Most patients were not satisfied with their therapy. Almost 10% of patients surveyed did not receive any treatment despite having active disease, while only a minority received potent medication to treat their chronic prurigo. In general, patients with chronic prurigo considered that they were not adequately treated and experienced high levels of dissatisfaction with their therapy.
Chronic nodular prurigo (CNPG; also known as prurigo nodularis) is the most prevalent subtype of chronic prurigo and is characterized by the development of severely pruritic hyperkeratotic nodules, a consequence of chronic itch and prolonged scratching (1). Treatment of CNPG is complex, and the disease is often refractory to available drugs (2). Recommendations for management of CNPG are discussed in national and international guidelines for pruritus and in a newly developed guideline specific for CNPG (3, 4). A stepwise approach should be adopted in the treatment of CNPG. If possible, the underlying diseases leading to chronic itch should be treated, although in most cases this does not lead to an improvement in CNPG (5). Topical corticosteroids and calcineurin-inhibitors, as well as ultraviolet (UV) therapy, have shown antipruritic efficacy in clinical studies (6–8). Recommended systemic options include gabapentinoids, antidepressants, immunosuppressants (cyclosporine A, methotrexate) and opioid modulators; however, clinical trials on these substances are lacking (3, 4). Monoclonal antibodies are promising novel agents (9–11), which may constitute a therapeutic option for CNPG in the near future. In a recent survey, European itch specialists revealed that the drugs they most often prescribe for CNPG include antihistamines, antidepressants, gabapentinoids and immunosuppressants, while there is a need for development of novel targeted therapies (12). Data on patient perspectives on available therapeutic options and their efficacy are lacking. Therefore, a prospective multicentre patient-oriented questionnaire-based study was performed, aiming to assess the perception of patients with CNPG on therapeutic goals, previously used therapies, overall satisfaction with therapy, efficacy of available therapeutic regimens and out-of-pocket costs.
The methods and population of this prospective, cross-sectional, cohort study are described in our initial publication related to the European Prurigo Project (EPP) (13). In brief, after signing the informed consent, patients with CNPG aged 18 years or older reporting having itch and nodular prurigo lesions in the previous week were asked to complete a questionnaire, either on paper or electronically. Patients were recruited at dermatological tertiary centres across Europe. Data were pseudonymized and collected centrally at a database in Münster (14).
In this study, 15 European centres from 5 regions, i.e. Germany (Münster, Berlin, Heidelberg), Northern Europe (Norway – Oslo, Sweden – Lund), Central Europe (Austria – Graz, France – Brest, Switzerland – Aarau), Eastern Europe (Poland – Rzeszow, Poland – Wroclaw, Russia – Moscow), and Southern Europe (Italy – Rome, Portugal – Coimbra, Spain – Barcelona, Turkey – Ayd?n) participated. The ethics committees corresponding to the participating centres approved the study (main ethics committee: Medical Faculty of the University of Münster, 2017-168-f-S), which was performed according to the Declaration of Helsinki. The study is registered at the German registry of clinical trials (DRKS00012876, registration date: 09.08.2017).
Assessments
This part of the study analysed the answers to question numbers 27–37 of the patient questionnaire (Appendix S1). The questions related to the most important therapeutic goals (questions 35–37) (15), the overall number of drugs used, and the number of drugs used specifically for treatment of CNPG (questions 27 and 28), previous therapies for CNPG (questions 29 and 30), overall satisfaction with therapy (question 31), best and worst therapeutic regimens (questions 32 and 33), and out-of-pocket costs (question 34).
Statistical analysis
All data were analysed descriptively (shown as absolute and percentage values for categorical data; median (interquartile range; IQR) for continuous data). For group comparisons of continuous variables (number of drugs taken by patients between different European regions), the Mann–Whitney U test was applied. The χ2 test was used for group comparisons of categorical variables (e.g. frequency of therapies used between very satisfied patients and the remaining cohort). Two-sided significance was set at p < 0.05. As there were missing values, the number of observations is given for each item for transparency. For comparisons between European regions, the countries were divided by regions according to a historical classification, as previously performed (13). Germany was regarded as a region on its own, due to its larger sample size and because 3 recruiting centres were located in Germany. All analyses were performed with SPSS v. 25.0 for Windows (IBM Corporation, Armonk, NY, USA).
Study population
A total of 509 patients were invited to participate in the study, between March 2017 and June 2019. Of these, 406 (251 females (61.8%), 155 males (38.2%); median age 63 years (interquartile range (IQR) 51–71 years)) reported having itch and pruriginous lesions in the previous 7 days and were therefore qualified to complete the whole questionnaire (Germany n = 137; Northern Europe n = 69; Central Europe n = 57; Eastern Europe n = 76; Southern Europe n = 67). Detailed information on the study population, including demographics and comorbidities, is given in the previous publication on the European cross-sectional study (13).
Therapeutic goals
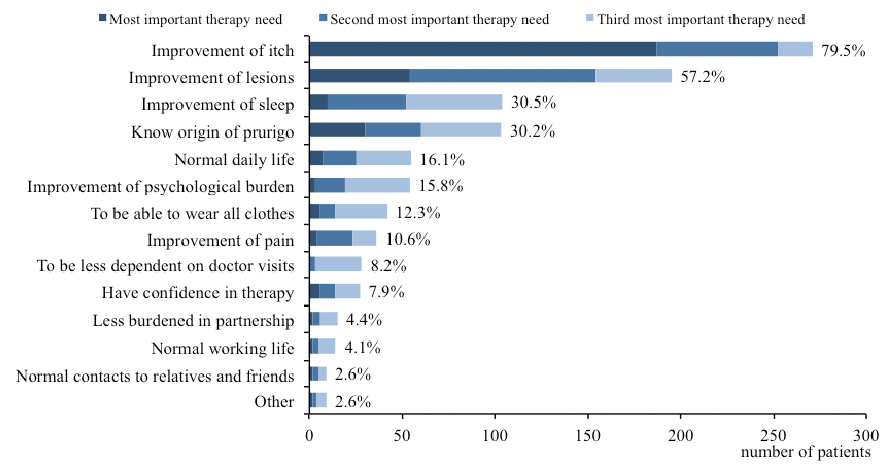
Asked for the 3 most important therapeutic goals, improvement in itch was mentioned most frequently (79.5%, 271/341), followed by improvement in skin lesions (57.2%, 195/341) and improvement in sleep (30.5%, 104/341). All reported therapeutic goals are shown in Fig. 1.
Fig. 1. Most important therapeutic goals. First, second and third most important therapeutic goals from the patients’ point-of view. In total, 341 out of 406 patients indicated at least one therapeutic goal. For each goal, the percentage of patients considering it as a top 3 goal is shown.
Previous therapies
Emollients, topical corticosteroids and antihistamines were the therapeutic regimens applied most often. All other therapies were used to a lower extent (Table I). The median total number [IQR] of drugs used by patients was 4 [2; 6], n = 379, while 1 of 4 drugs taken by the patients was used to treat CNPG (1 [0; 2], n = 375). Patients from Central Europe took a lower amount of drugs for CNPG compared with patients from Northern Europe (p = 0.012), Eastern Europe (p = 0.007) and Southern Europe (p = 0.005).
Table I. Previous treatment regimens
Satisfaction with therapy
Overall, more than half of the patients were not satisfied with the therapy they had received in the previous 6 months (not satisfied or rather not satisfied: 56.8%, 225/396), while 9.8% (39/396) did not receive any therapy in the previous 6 months, despite having active disease. Only 33.3% of patients were satisfied or very satisfied with the therapy. The highest proportion of patients who were not satisfied or rather not satisfied with the therapy was recorded in Southern Europe (73.1%) and the lowest in Northern Europe (46.2%; Fig. 2).
Fig. 2. Patient satisfaction with therapy in the previous 6 months (n = 396).
When asked about the most effective therapies (n = 352), a substantial proportion of patients considered that none of the options were effective (28.7%). Topical steroids and emollients were regarded both as the most (13.6% and 10.5%, respectively) and least effective (10.0% and 28.1%, respectively) therapy. Systemic immunosuppressants were frequently considered as the most effective therapy (12.5%). When considering only the patients who previously used them, 46.3% (44/95) reported this drug class as the most effective. All other options were chosen by less than 10% of respondents. Antihistamines (11.7%) next to UV therapy (11.1%) were often reported as the least effective therapy (Table II).
Table II. Most and least effective treatments
Out-of-pocket costs
Overall, the majority of patients (59%, 236/400) estimated up to €500 or more out-of-pocket costs owing to CNPG treatments in the previous 6 months (including personal purchases, prescribed drugs and travel costs to the physician). The distribution of out-of-pocket costs overall and across regions is shown in Fig. 3.
Fig. 3. Patients’ estimate of out-of-pocket costs (in Euro) related to chronic nodular prurigo in the previous 6 months (n = 400).
CNPG is a severe condition, in which itch plays a central role. Patients experience itch of high intensity, often accompanied by painful sensory symptoms, such as burning and stinging. Affected individuals consider itch to be the most burdensome aspect of the disease, followed by the presence of skin lesions (13). As a result of the itch and skin lesions, patients with CNPG are burdened with substantial impairment in their quality of life, sleep loss (13), high incidence of depression and other psychiatric comorbidities (16), and potentially higher risk of suicide (17). Owing to the severity of the disease, effective treatment is of great importance for those affected. The current study showed, as expected, that treatment of itch is by far the most important priority for patients with CNPG, followed by improvement in skin lesions and sleep quality, which is in line with the clinical profile of the disease (13). A homogenous profile regarding therapeutic goals was observed across European regions. Interestingly, understanding the origin of CNPG was also mentioned by a substantial number of patients. Itch associated with CNPG can be of dermatological, systemic, neurological, psychiatric/psychosomatic, multifactorial or unknown origin (1, 18). However, once established, CNPG is a distinct disease, and diagnosis and therapy of the triggering condition does not lead to improvement in the majority of patients. The treatment goals of patients with CNPG should be taken into account by attending physicians in the management of these patients.
Owing to the lack of approved therapies, only a minority of patients across all regions in Europe reported treatment with potent medications. Systemic drugs with anti-inflammatory effects or those with a central anti-pruritic action were seldom used. Only a few patients had been prescribed biologics (nemolizumab (n = 1), omalizumab (n = 1), ustekinumab (n = 1); Table I). Even though randomized controlled trials are still lacking, case series have shown beneficial effects of systemic immunosuppressive drugs (cyclosporine (19, 20), methotrexate (21, 22)), gabapentinoids (23) and μ-opioid receptor antagonists (24, 25). In a recently consented guideline on the treatment of chronic prurigo, systemic medications are recommended to patients with CNPG refractory to commonly used treatments, such as emollients, topical steroids, antihistamines and phototherapy (26) (Table I), provided contraindications are excluded. These findings suggest that a substantial proportion of patients were not offered potent systemic medication, and this omission results in low levels of satisfaction with therapy and documents the high unmet need (Fig. 2). In line with this, 9.8% of patients from the current cohort did not receive any therapy in the 6 months prior to completing the survey, despite having active disease, pointing to insufficient care. The proportion of patients not receiving any treatment was highest in Northern Europe (20.0%) and lowest in Southern (1.5%) and Eastern Europe (4.1%), suggesting possible disparities across Europe regarding the healthcare systems. The current study also observed discrepancies in the use of emollients across Europe, with the highest percentage of patients using emollients in Germany (92.0%) and lowest in Eastern Europe (65.8%). It is possible that the high costs of emollients for the patients limit their use in some countries.
The low awareness and experience with CNPG among physicians, the lack of approved therapies and shortage in recommending off-label therapies in CNPG are relevant factors contributing to the use of less effective therapies and, consequently, the subpar care of CNPG patients. Other factors influencing patient satisfaction, such as the patient-doctor relationship and attention to quality of life (26), were not analysed in this study and should be addressed in the near future.
High levels of disbelief were detected in patients with CNPG regarding the efficacy of available treatment options. When asked about the most effective treatment regimen, almost one-third of patients considered none of the options to be effective (Table I). Of the total patient population, 12.5% regarded systemic immunosuppressive drugs as the most effective agents. Considering that only 23.4% of the current patient cohort had ever received immunosuppressive agents to treat CNPG, this represents a relatively large proportion of patients. In contrast, antihistamines (5.4%) and emollients (10.5%) were only seldom indicated as the most effective therapy, especially when taking into account that these are often-used therapies (55.2% and 84.7%, respectively). Interestingly, emollients were considered both as the most and least effective therapy by a substantial number of patients (10.5% and 28.1%, respectively). While emollients may provide relief when applied to itchy skin, the effect is usually of short duration, which would explain the conflicting observations in this study.
Novel agents, such as biologics (dupilumab and nemolizumab), as well as opioid receptor modulators (nalbuphine) and neurokinin-1 receptor antagonists (aprepitant) were reported as the most effective therapies by a few patients. To date, these drugs are only available in clinical trials or at expert centres in off-label regimens, but may constitute effective therapies for resistant CNPG cases in the future. A recent 12-week randomized placebo-controlled, double-blind, phase 2 trial investigating the efficacy of nemolizumab in CNPG showed promising results (9), while case series suggest a good anti-pruritic effect of dupilumab (11, 27, 28). Clinical trials investigating these substances in patients with CNPG are needed in order to confirm their efficacy and safety.
Thalidomide was also referred to by one patient as the most effective therapy. Although case series indicate a beneficial effect of thalidomide in CNPG (29–31), its use should be considered only in exceptional cases by physicians with experience with this drug, due to the high risk of developing irreversible adverse reactions, such as peripheral neuropathy.
Some patients with CNPG mentioned a vast array of non-pharmacological treatments (e.g. homeopathy, acupuncture, diet, therapeutic baths, climate therapy, salt water; Table II) as the most effective therapy, reflecting their disbelief in conventional medical therapeutic options.
Twenty-one patients reported being very satisfied with the therapy they had received in the previous 6 months. Very satisfied patients showed, as expected, lower itch intensities (NRS: p < 0.001; verbal rating scale: p = 0.001, (13)) and impairment in quality of life (5 pruritus life quality: p < 0.001, (13)) compared with the remaining patients receiving a therapy in the previous 6 months. Of note, very satisfied patients were treated more often with “other therapies” in the previous 6 months compared with the remaining cohort (p = 0.021). Nemolizumab (n = 2), fosaprepitant (n = 1) and apremilast (n = 1) were mentioned as the most effective drugs by very satisfied patients, suggesting that novel innovative drugs may improve care in CNPG. In addition, very satisfied patients more frequently reported having had psychotherapy in the past (p = 0.005), indicating the importance of psychological care in this condition. Other factors, such as age, sex, geographical distribution or presence of atopic conditions, did not differ when comparing very satisfied patients with the remaining cohort receiving a therapy.
An additional burden for patients is the relatively high out-of-pocket costs related to CNPG. The vast majority of patients reported out-of-pocket costs below 500€ across the European regions in the previous 6 months (82.5–89.3%), while a larger percentage of patients from Eastern Europe (65.3%) and Northern Europe (46.2%) reported costs below 100€. Across Europe, only a small minority of patients mentioned spending over 500€ in the previous 6 months. However, these results should be interpreted with caution, since the current study did not control for disease severity, general cost of living, discrepancies in health insurance systems or other costs (e.g. absenteeism), socioeconomic status and divergent currencies across European countries.
Study limitations
One limitation of this study is that patients with CNPG were recruited at specialized tertiary units, such as university hospitals or large community hospitals. This may impact the current findings, since these tertiary units probably treat the most severe cases of CNPG. On the other hand, patients being treated in dermatological offices or by primary care physicians may less often be prescribed more potent medications, such as systemic immunosuppressants or biologics, and have less access to novel substances being tested in clinical trials. Another limitation is that the patient questionnaire used was not validated. Moreover, data was obtained by self-report and was not validated through medical records.
Conclusion
This large multicentre study, performed in 12 European countries, documents the low use of potent systemic drugs and high level of dissatisfaction and disbelief in available treatments in CNPG. A greater awareness of CNPG and the development of guidelines specifically for CNPG are essential in order to improve its management, while novel therapies, such as biologics and opioid modulators, may be decisive to improve care in the future.
The authors thank B. Pfleiderer, MD, for assistance in the study preparation.
This study was supported by the European Academy of Dermatology and Venereology (EADV, No. 2016-012 to MP). Galderma S.A, Kiniksa Pharmaceuticals and Menlo Therapeutics provided support for the study.
Conflicts of interest. MPP is an investigator for Trevi Therapeutics; a consultant for Galderma; and has received speaker honoraria/travel fees from Galderma, Menlo Therapeutics, Novartis and Trevi Therapeutics. CZ has received speaker honoraria/travel fees from Beiersdorf and Dermasence. EW is an investigator for Menlo Therapeutics, Trevi Therapeutics, Kiniksa Pharmaceuticals and a member of the advisory board meetings for Menlo and Trevi. SG has received consulting support from companies, including Menlo Therapeutics. LM is a consultant for Galderma, Menlo, Trevi, Sanofi, and was investigator for Galderma, Trevi, Sanofi. EB is an investigator for Biogen, Galderma, and is a consultant and/or member of the advisory board for Janssen, Lilly, Celgene, Novartis, Pfizer, and received financial support from Sanofi, Abbvie. AL is a consultant for Galderma and Novartis; and has received speaker honoraria/travel fees from Galderma, Bayer, LEO, Pierre Fabre. SB has received speaker honoraria/travel fees from LEO. JCS is an investigator for AbbVie, Amgen, Janssen, Menlo Therapeutics, Merck, Novartis, Regeneron, Trevi, UCB, Galapagos, Pfizer, Helm, InflaRX, Incyte; advisor for AbbVie, Leo Pharma, Novartis, Pierre-Fabre, Menlo Therapeutics, Trevi and speaker for AbbVie, Novartis, Sanofi-Genzyme, Janssen, Leo Pharma, Novartis, SunFarm, Eli Lilly. AR is a consultant or speaker for AbbVie, Bioderma, Celgene, Chema Elektromet, Eli Lilly, Galderma, Janssen, Leo Pharma, Medac, Menlo Therapeutics, Novartis, Pierre-Fabre, Sandoz and Trevi; Principal Investigator or Subinvestigator in clinical trials sponsored by AbbVie, Drug Delivery Solutions Ltd, Galderma, Genentech, Janssen, Kymab Limited, Leo Pharma, Menlo Therapeutics, MetrioPharm, MSD, Novartis, Pfizer and Trevi. FJL is an investigator for DS Biopharma, Eli Lilly, Galderma, Pfizer, Menlo Therapeutics, Trevi Therapeutics. He is a member of the advisory boards and/or has received speaker honoraria/travel fees from AbbVie, Almirall, Celgene, Eli Lilly, Janssen, Leo Pharma, Menlo Therapeutics, Novartis, Pfizer, Trevi Therapeutics. MM has received honoraria as a speaker and/or consultant for Amgen, Aralez, argenx, Bayer, Beiersdorf, Celgene, Galderma, Menlo, Moxie, Novartis, Roche, Sanofi, Shire, Uriach. MS is a consultant and member of advisory boards of AbbVie, Almirall, Celgene, Eli Lilly, Janssen-Cilag, Menlo, Novartis and Pfizer. He has received speaker honoraria/travel fees from AbbVie and Novartis. ES-B is an investigator, a consultant or gave presentations for Regeneron, Sanofi, Stiefel/GSK, Pierre Fabre, La Roche Posay, Leo Pharma, Novartis, Almirall, Pfizer, Galderma, Lilly, Abbvie. MG has been a consultant and received speaker honoraria for Novartis and Sanofi. MA reports receiving speakers honoraria or grants from, or participated in clinical trials or health services research projects for Abbott/AbbVie, Almirall, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Forward Pharma, Galderma, GSK, Hexal, Janssen, LEO Pharma, Medac, MSD, Novartis, Pfizer, Sandoz, Teva, TK, Trevi, and Xenoport. MD is co-founder of Hippokrates IT. SS is an investigator for Dermasence, Galderma, Kiniksa Pharmaceuticals, Menlo Therapeutics, Trevi Therapeutics, Novartis, Sanofi, and Vanda Pharmaceuticals Inc.; and is a consultant and/or member of the advisory board for Almirall, Bayer, Beiersdorf, Bellus Health, Bionorica, Cara Therapeutics, Celgene, Clexio Biosciences, DS Biopharma, Galderma, Menlo Therapeutics, Novartis, Perrigo, and Trevi Therapeutics. TAL has been a consultant for Menlo and Novartis. HFS is an advisor and/or investigator for Menlo Therapeutics, Abbvie and Novartis. JW, JAH, ES, NNP, AB, MS, TN, VH, SaS, IG, FD, JE, CF, UG, CR and GS have no conflicts of interest.


 Click to show fullsize
Click to show fullsize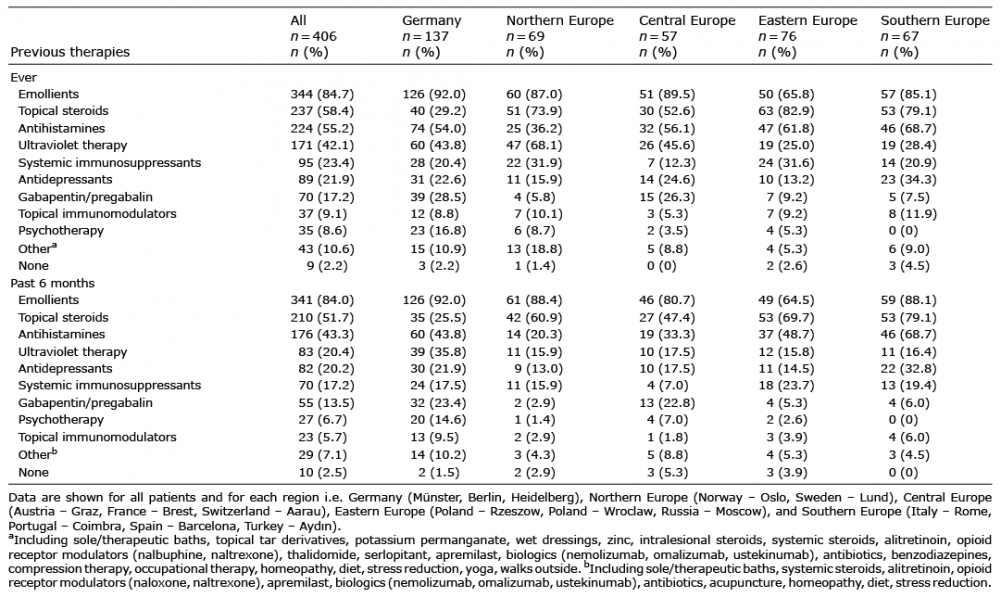 Click to show fullsize
Click to show fullsize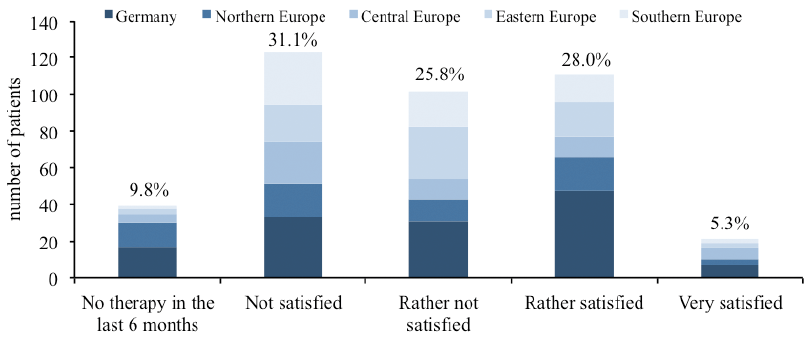 Click to show fullsize
Click to show fullsize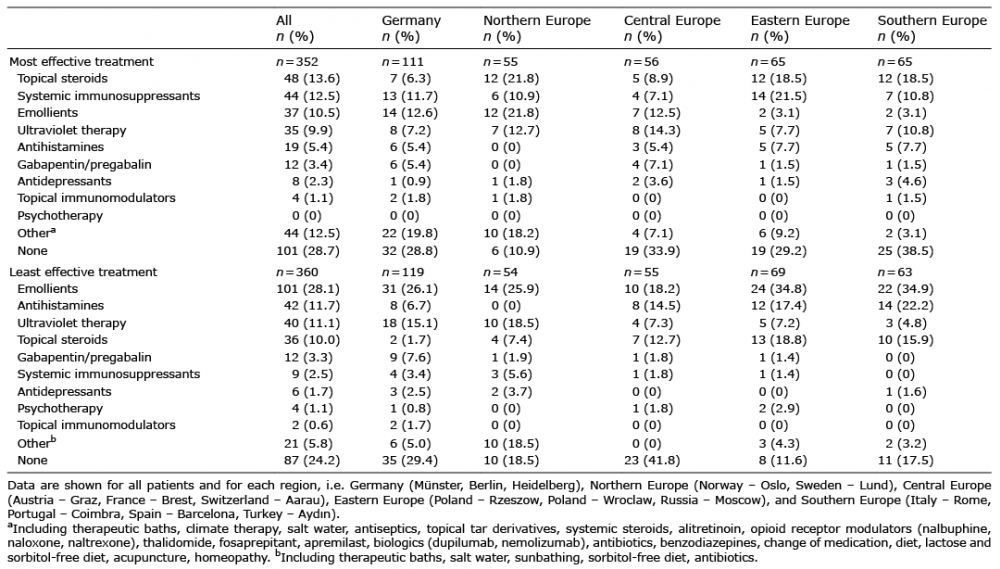 Click to show fullsize
Click to show fullsize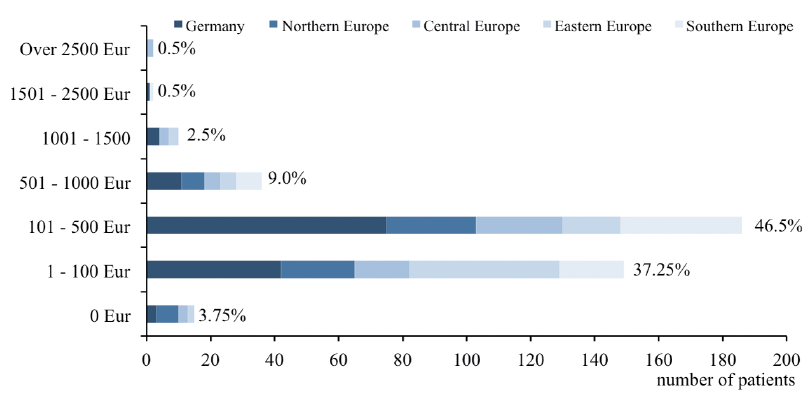 Click to show fullsize
Click to show fullsize