


1Central Laboratory of Pathology, Nice University Hospital, 30, Avenue Voie Romaine- CS 51069, FR-06001 Nice, Cedex 1, France, 2Nail’s Dermatology Office, Cannes, France, 3Laboratory of Solid Tumors Genetics, Institute for Research on Cancer and Aging of Nice (IRCAN) CNRS UMR 7284/INSERM U1081, Université Côte d’Azur, Nice University Hospital, Nice, France. E-mail: xst.perrin@bbox.fr
#These authors contributed equally to this work.
Accepted Dec 14, 2020; Epub ahead of print Dec 15, 2020
Acta Derm Venereol 2021; 101: adv00388.
doi: 10.2340/00015555-3727
Superficial CD34+ fibroblastic tumour (SCFT) is an uncommon low-grade mesenchymal tumour of intermediate (borderline) malignancy. It occurs in middle-aged adults, with a slight male predilection, most frequently on the lower limbs, particularly the thighs (1–8). To the best of our knowledge, there has been no report of this tumour occurring in the subungual or periungual region. We report here the first case of SCFT of subungual region of the finger with a misleading clinical feature. Immunohistochemical features and RNA sequencing analysis using a panel dedicated to sarcomas ruled out more aggressive neoplasms, such dermatofibrosarcoma protuberans (DFSP).
A 63-year-old man presented with a one-year history of onychodystrophy of the ulnar aspect of his third left finger. Examination revealed that the nail plate was slightly and radially lifted by a tumour. This tumour was identifiable distally as a filiform keratotic, protruding structure with a longitudinal area of yellow discolouration extending most of the length of the adjacent nail plate. The yellow nail plate was medially limited by deep pits as tread marks in the snow arranged in a longitudinal line (Fig. 1a). The longitudinal xanthonychia mimicked onychomatricoma. However, on closer examination, the nail plate was thin, with lateral destruction contrasting with the thick nail plate typically seen in onychomatricoma. No pain was associated with the lesion. The radiological findings did not detect any bony abnormality or connection with the tumour. The combination of focal distal nail plate destruction and acquired fibrokeratoma-like feature led us to suspect Bowen’s disease. Histopathological examination of the biopsy revealed features of pleomorphic fibroma. However, the high proliferation index (Ki67) up to 20% was considered suggestive of an aggressive form of CD34 pleomorphic fibroma.
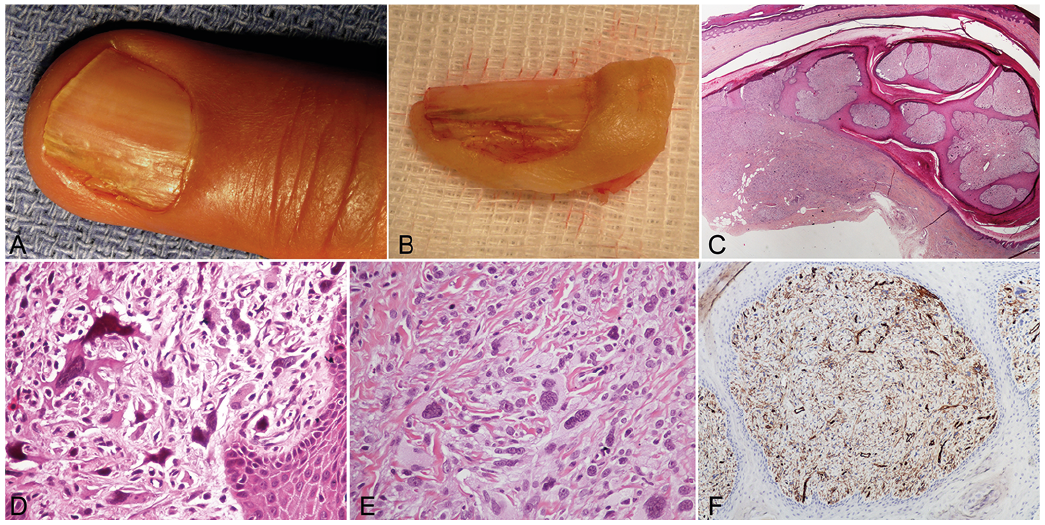
Fig. 1. (A) Fibrokeratoma-like features with longitudinal xanthonychia. (B) Macroscopic examination showing the multibranched fibrokeratoma feature. (C) Scanning power of the transverse section of the matrical region, under the dorsal portion of the proximal nail fold, showing the polypoid feature with multiple fibroepithelial digitations. Note the infiltrative growth of the tumour (asterisk), and partial epidermal metaplasia of the matrix epithelium at the level of the tumour. The medial and peripheral part of the lesion with a thin nail plate is indicated by an arrow (original magnification (OM) ×20). (D) Higher magnification of the enlarged hyperchromatic bizarre-appearing nuclei (OM ×400). (E) Xanthomatous cells interspersed between cells with granular cytoplasm (OM ×400). (F) Diffuse CD34 expression of both the spindle and epithelioid cells (OM ×100).
Macroscopically, the multibranched fibrokeratoma-like feature of this tumour was clearly observed after partial avulsion of the nail plate (Fig. 1b). Microscopically, the tumour grew in both a superficial circumscribed and an infiltrative fashion (Fig. 1c). It was composed of moderately to, sometimes highly, cellular fascicles and sheets of spindled to epithelioid cells with an abundant fibrillary, glassy or granular cytoplasm (Fig. 1d, e). Proximally, the polypoid submatrical tumour was associated with epithelial collarette forming, while, distally, the tumour presented several fibroepithelial digitations (Fig. 1c). The morphological hallmark of the tumour was the presence of enlarged hyperchromatic bizarre-appearing cells, some of which harboured intranuclear pseudo-inclusion or giant macronucleoli (Fig. 1d). Xanthomatous changes were identified in rare foci (Fig. 1e). Mast cells were abundant without a mixed inflammatory cell infiltrate. Despite the striking nuclear pleomorphism, there was a low mitotic rate (< 1 mitosis per 50 high-powered fields (HPFs)). The Ki67 index was low in most sections (<5%) with a few sections with higher areas, of up to 20%. No necrosis, or myxoid area or hyalinized blood vessels or hemosiderin deposition was observed. Careful sampling did not identify univacuolated or multivacuolated lipoblasts.
Tumour cells displayed strong positivity for CD34 (Fig. 1f), a focal staining for CD10, but they were negative for CD99,bcl2, MUC4, Smooth muscle actin, desmin, myogenin, STAT6, ALK1, S100 protein, melan A, Hmb45, SOX10, pancytokeratin and CD31. INI 1 expression was retained. The tumour contained rare isolated cells or clustered cells with immunoreactivity for p63 and EMA. Of note, p16 and p53 were diffusely and focally expressed, respectively. RNA-sequencing analysis, using a panel dedicated to sarcoma ( RNA seq), notably ruled out dermatofibrosarcoma protuberans (DFSP), fibrosarcoma arising in DFSP, solitary fibrous tumour and synovialosarcoma. Array-comparative genomic hybridization (aCGH) analysis revealed a complex genomic quantitative profile, including losses of RB1 gene (13q) and TP53 (17p) and amplifications of the 18p and 19p regions. Notably, no MDM2 amplification was observed; therefore we could to rule out a dedifferentiated liposarcoma.
The overall findings were consistent with a diagnosis of SCFT. The tumour was incompletely excised by “en bloc” excision of the nail unit. Distal amputation was mandatory. No evidence of recurrence was observed in 10 years of follow-up.
Fibrokeratoma-like Bowen’s disease is a classical clinical variant of subungual Bowen’s disease. This is the first report of a case of subungual SCFT as a fibrokeratoma-like Bowen’s disease. This misleading presentation was replicated on histological grounds, as the biopsy showed a feature of pleomorphic fibroma with a discordant high proliferation index (Ki67). SCFT is a novel entity of the cutaneous CD34+ spindle cell mesenchymal tumour family. SCFT is characterized by a striking pleomorphism, a distinctive abundant granular or glassy cytoplasm, very low mitotic activity, diffuse CD34 immunoreactivity, and rare foci of xanthomized cells (1–8). The biological behaviour of SCFT, based on fewer than 50 documented cases (1–8), is generally regarded as a low-grade mesenchymal neoplasm of intermediate malignancy. Follow-up information, available in 38 cases, revealed a very low local recurrence rate, < 1%, and only one patient developed regional lymph node metastasis.
The current study is the first to provide a comprehensive molecular analysis of SCFT. Importantly, the complexity of the quantitative genomic profile emphasizes its potential malignant behaviour. SCFT must be distinguished from other mesenchymal neoplasm with pleomorphism and CD34 positivity. A diagnosis of DFSP that has undergone sarcomatous differentiation was ruled out by RNA sequencing. A diffuse expression of CD34 has rarely been described in synovialosarcoma (9), and minute synovial sarcoma of the hand is not uncommon (10) . In the current case, RNA sequencing eliminates this diagnosis. Dedifferentiated solitary tumour exhibits a specific positivity for STAT6 (11). The retained expression of SMARCB1/INI1 rules out the classical and proximal type of epithelioid sarcoma. Both atypical fibroxanthoma and pleomorphic dermal sarcoma predominantly affect the sun-damaged skin of the head and neck in elderly people, have brisk and atypical mitotic activity, and lack CD34 expression (1, 3).
Differential diagnosis also may include myxoinflammatory fibroblastic sarcoma and superficial acral fibromyxoma, both of which have an acral predilection and CD34 immunoreactivity (1, 3). However, no myxoid stroma was observed in the tumour in the current case. In addition, myxoinflammatory fibroblastic sarcoma is characterized by a prominent inflammatory infiltrate and a specific TGFBR3-MGEA5 fusion, which is absent in the tumour in the current case. Conversely, superficial acral fibromyxoma is cytologically benign. Pleomorphic hyalinizing angiectasic tumour, which is morphologically and genetically related to myxoinflammatory fibroblastic sarcoma, has distinctive features, such as thick-walled ectatic with prominent perivascular hyalinization. Such features were lacking in the current case.
As cellular angiofibroma has recently been described in a subungual location (12), the differential diagnosis for SCFT includes cellular angiofibroma with a sarcomatous component (13). This last tumour was ruled out by its prominent distinctive benign component with striking hyalinized vessels.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize