


1Department of Health Sciences, Section of Dermatology, 2Department of Experimental and Clinical Medicine, Section of Gastroenterology, University of Florence, Florence, and 3Gastroenterology Unit, San Giuseppe Hospital, Azienda USL Toscana Centro, Empoli, Italy
Granular deposits of IgA represent the specific cutaneous marker of dermatitis herpetiformis. The prevalence of IgA deposits in the skin of patients with coeliac disease without dermatitis herpetiformis remains unknown. In this prospective case-control study, skin biopsies from newly diagnosed coeliac patients without dermatitis herpetiformis were analysed by direct immunofluorescence. Controls included healthy volunteers and patients with both bowel symptoms and skin eruptions unrelated to coeliac disease. Clinical data and serum level of anti-tissue transglutaminase and anti-epidermal transglutaminase IgA antibodies were collected from patients and controls. Granular deposits of IgA or IgA1 in the skin were found in 29 out of 45 patients with coeliac disease (64.4%), and in none of the included controls (specificity 100%; sensitivity 64.4%). Positive direct immunofluorescence correlated significantly with an increased serum level of anti-epidermal transglutaminase IgA antibodies (p < 0.005). This study shows that granular deposits of IgA represent a low sensitive, but highly specific, cutaneous marker of coeliac disease independent of dermatitis herpetiformis.
Key words: general dermatology; direct immunofluorescence; coeliac disease; gastroenterology; dermatitis herpetiformis; immunoglobulin A; granular deposit; epidermal transglutaminase.
Accepted Jan 5, 2021; Epub ahead of print Jan 11, 2021
Acta Derm Venereol 2021; 101: adv00382.
doi: 10.2340/00015555-3742
Corr: Roberto Maglie, Department of Health Sciences, Section of Dermatology, University of Florence, Viale Michelangiolo 41, IT-50125 Florence, Italy. E-mail: robertomaglie.med@libero.it
Dermatitis herpetiformis, the specific cutaneous manifestation of coeliac disease, is characterized by granular deposits of IgA along the dermal–epidermal junction. These deposits are thought to be relevant for the pathology of dermatitis herpetiformis by promoting fibrinogen activation and recruitment of neutrophils in the skin. This study shows that approximately two-thirds of patients with a new diagnosis of coeliac disease, but without a history of dermatitis herpetiformis, have granular deposits of IgA in the skin, resembling those observed in patients with dermatitis herpetiformis. This suggests that granular deposits of IgA in the skin represent a specific cutaneous marker of coeliac disease, independent of dermatitis herpetiformis.
Coeliac disease (CD) is a chronic immune-mediated enteropathy related to a permanent intolerance to gluten (1). Dermatitis herpetiformis (DH) is the specific cutaneous manifestation of CD (2, 3). Patients with CD and those with DH both carry the same predisposing HLA DQ2/DQ8 haplotypes and show circulating IgA autoantibodies against tissue transglutaminase (TG2); both diseases significantly improve with a gluten-free diet (GFD); finally, most patients with DH show evidence of CD-related histological changes on duodenal biopsy (4).
In DH skin, IgA targeting epidermal-transglutaminase (TG3) forms granular aggregates with TG3, which deposit at the tips of the dermal papillae (5). Detection of granular deposits of IgA at the dermal–epidermal junction (DEJ) by direct immunofluorescence (DIF) represents the gold standard for diagnosis of DH (6). In patients with DH, DIF is sufficient for diagnosing CD without the need for duodenal biopsies (6). However, despite the high performance of serological tests, including anti-TG2 IgA antibodies and anti-endomysial IgA antibodies, for identifying patients with CD, current guidelines still recommend performing duodenal biopsies to reach an accurate diagnosis of CD in adult patients without DH (1). In more detail, a recently published large international study demonstrated that a 10-fold increase in IgA anti-TG2 antibody levels has a strong predictive value in identifying adult patients with CD-associated histological changes at duodenal biopsy. The sensitivity of this serological assay for patients with low clinical suspicion of CD, but with a Marsh 3 grade at duodenal biopsy, was, however, approximately 50% (7). Because duodenal biopsy is an invasive and time-consuming procedure, there is an unmet need for alternative diagnostic methods.
The pathology of DH is based on fibrinogen activation and neutrophil recruitment by enzymatically active IgA/TG3 aggregates in the skin. However, it remains unclear why IgA/TG3 deposits persist for years in the skin of patients with DH despite the absence of active lesions (8). In addition, deposits of IgA in skin, resembling those in DH, have been shown to occur in patients with CD but without DH (9, 10). The main aims of this study were to investigate the frequency of IgA deposits in the skin of patients with CD but without DH, and to evaluate whether DIF of the skin may be employed as a tool for diagnosing CD independent of the occurrence of DH.
Patients
Patients with a new diagnosis of CD referred to the Gastroenterology Unit of the Department of Experimental and Clinical Biomedical Sciences, University of Florence and the Gastroenterology Unit of San Giuseppe Hospital, Empoli, USL Toscana Centro, Italy, were consecutively enrolled from November 2015 to April 2018.
Inclusion criteria were: age ≥ 18 years; diagnosis of CD confirmed by typical histopathology findings at duodenal biopsy according to the Marsh classification modified by Oberhuber (11); patients still on a gluten-containing diet or on a GFD started ≤ 30 days before inclusion into the study.
Exclusion criteria were: age < 18 years; GFD started >30 days before inclusion; treatment with systemic or topical steroids and/or immunosuppressive drugs during the 12 weeks before inclusion; presence of active skin lesions and/or skin symptoms, including itch; history of photosensitivity or connective tissue diseases; positive testing for antinuclear antibodies or anti-extractable nuclear antigen antibodies; denied consent.
At the time of inclusion in the study, clinical data, results of duodenal biopsy, and the serum level of anti-TG2 antibodies were recorded. Moreover, a 3-mm punch biopsy for DIF, from normal-appearing skin on the buttocks or elbows, and a serum sample for immunoenzymatic analysis of anti-TG3 antibodies were collected from each patient.
As a control, biopsy samples from apparently normal skin taken from the same sites (buttocks or elbows) were collected from 50 healthy volunteers (control group 1) matched for age and sex. In these cases, CD was excluded by anti-TG2 antibody testing. Finally, perilesional skin samples from 10 patients (control group 2) with gastrointestinal symptoms and skin eruptions unrelated to CD (7 patients with eczematous eruptions and 3 patients with psoriasis) were analysed by DIF. In such patients, CD was excluded by anti-TG2 antibody testing and duodenal biopsy.
Direct immunofluorescence
DIF was performed investigating the presence of IgA, IgA1, IgG, IgM and C3 deposits. IgA2 were not examined because previous studies demonstrated that IgA1 represents the predominant IgA subclass found in skin deposits of DH (12, 13). After collection, skin biopsies were immediately frozen at –80°C and then prepared as 5-μm thick slides, which were stained with fluorescein-conjugated antibodies against human IgA, IgA1, IgG, IgM and C3 (DAKO, Copenhagen, Denmark).
The slides were observed with Nikon C2 confocal microscope by 2 blinded independent observers (EA, RM). Morphology (i.e. granular or linear) and localization (i.e. at the DEJ) of the deposits were recorded for each slide. As for DH, DIF was considered positive if granular deposits of IgA and/or IgA1 were found along the DEJ or at the dermal papillae.
Immunoenzymatic analysis
Enzyme-linked immunoassay (ELISA) for anti-TG3 antibodies were performed according to manufacturer instructions (Immunodiagnostik, Bensheim, Germany), as described previously (14). Anti-TG3 antibodies were considered positive when their level was ≥ 22 UI/ml, borderline for values > 16 and < 22 UI/ml, and negative for values ≤ 16 UI/ml. Anti-TG2 IgA antibodies were measured by commercially available ELISA kit (Eu-TG2 IgA, Eurospital, Trieste, Italy), according to the manufacturer’s instructions. Anti-TG2 IgA antibodies were considered positive when their level was ≥ 16 UI/ml, borderline for values > 9 and < 16 UI/ml, and negative for values <9 UI/ml.
Confocal microscopy
Co-localization studies for investigating IgA, TG2 and TG3 expression in the skin of patients with CD were performed, as described previously (11). Approximately 10-μm serial sections of fresh-frozen skin biopsies were fixed with ice-cold acetone, then blocked with 0.25% casein in Tris-buffered saline (TBS; 0.88% NaCl, ThermoFisher, 0.24% tris(hydroxymethyl) aminomethane, and distilled water). FITC-labelled antibodies against human IgA (DAKO) and unlabelled polyclonal rabbit anti-human TG2 (Zedira, Darmstadt, Germany) or anti-human TG3 antibodies (Zedira) at 1:500 were prepared in TBS containing 1% foetal calf serum (FCS) and incubated on sections for 1 h at room temperature.
Secondary goat antibodies against rabbit IgG AlexaFluor 568 (Molecular Probes, Eugene, OR, USA) at 1:200 were prepared and incubated on sections for 1 h. Sections were visualized with a Nikon C2 confocal microscope.
Statistical analysis
Categorical variables were presented as numbers with percentages. The differences across selected variables were assessed by means of Pearson’s χ2 test (or Fisher’s exact test, where required). All tests were considered statistically significant at p < 0.05. The sensitivity and specificity (95% confidence interval; CI) of the finding of granular deposits of IgA in the skin for diagnosis of CD were assessed. Analyses were performed with SPSS v.20.0 (IBM Corp., Armonk, NY, US).
Patients
A final total of 45 patients (16 males; 29 females; median age 40, range 18–80 years) met the inclusion criteria and were included in the study.
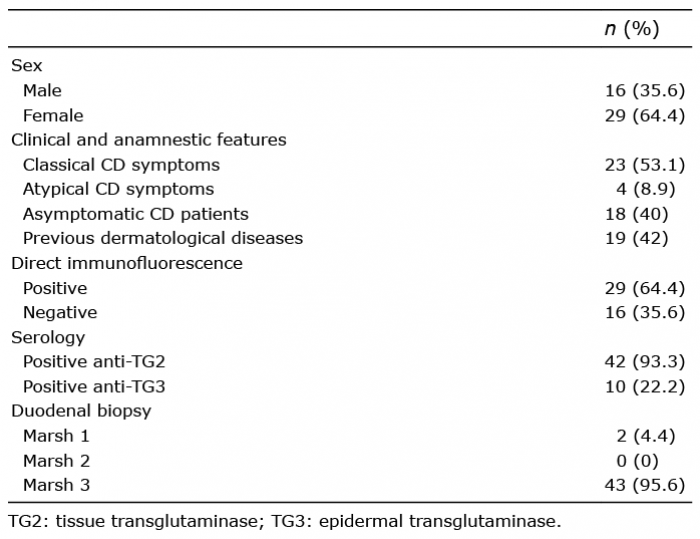
All the relevant patient data are reported in Table I. Briefly, 23 patients (53.1%) showed symptoms of classical CD, including diarrhoea, bloating, and weight loss; 4 patients (8.9%) had an atypical presentation of CD, showing constipation and/or abdominal pain in the absence of signs of malabsorption; finally, 18 patients (40%) had a subclinical presentation of CD or did not show any symptoms.
Table I. Clinical features and laboratory results of the 45 patients with coeliac disease (CD) included in the study
Eleven patients (24.4%) had systemic associated diseases, the most frequent being autoimmune thyroiditis (4 patients, 8.9%). Other associated diseases included Down syndrome, hypertension, colorectal and breast cancer, Parkinson’s disease, and asthma.
Nineteen patients (42.2%) referred a previous history of cutaneous or oral diseases, including atopic dermatitis (7 patients; 15.6%), psoriasis (4 patients; 8.9%), lichen planus, hidradenitis suppurativa, urticaria, vitiligo, oral aphthosis, rosacea, and skin xerosis.
Direct immunofluorescence
Overall, DIF showed granular IgA and/or IgA1 deposits along the DEJ or at the tips of the dermal papillae in 29 out of 45 patients (64.4%) (Fig. 1A–C). Among the positive patients, 27 out of 29 (93.1%) had IgA deposits, while 16 (55.2%) had IgA1 deposits. Fourteen out of 29 (48.3%) had both IgA and IgA1 deposition, 13 (44.8%) had only IgA deposition and 2 (6.9%) had only IgA1 deposition.
Fig. 1. (a–c) Granular deposits of IgA in the skin of patients with coeliac disease without dermatitis herpetiformis revealed by direct immunofluorescence; (d) absence of IgA deposition in the skin of a healthy control.
Some of the patients with IgA and/or IgA1 on DIF showed other immune deposits at the DEJ. In particular, one patient out of 29 (3.4%) showed granular deposits of IgG, 11 (37.9%) showed granular deposits of IgM, and 19 (65.5%) showed granular deposits of C3. Among the 16 patients without IgA or IgA1 deposits, who were thus considered as having a negative result, 2 had granular deposits of IgM at the DEJ.
Interestingly, none of the skin specimens from the 50 healthy controls (control group 1) nor from the 10 patients with gastrointestinal symptoms and inflammatory skin diseases (control group 2) had IgA and/or IgA1 deposits at the DEJ (Fig. 1D). Other DIF findings in the control group 1 included 4 cases (8%) with granular IgM deposits and 5 (10%) with granular C3 deposits. Likewise, in the control group 2, 4 cases (40%) had granular C3 deposits along the DEJ, 2 (20%) had perivascular IgM and C3 deposits, and 2 (20%) had IgM florescent bodies at the DEJ.
Overall, the presence of IgA and/or IgA1 deposits in the healthy skin showed a 64.4% (95% CI 50.4–78.4) sensitivity and a 100% (95% CI 97.2–100) specificity for the diagnosis of CD. The positive predictive value (PPV) of the test was 100%, while the negative predictive value (NPV) was 75.8%.
Serology of anti-TG2 and TG3 antibodies
Serum levels of anti-TG2 antibodies were above the cut-off level in 42 out of 45 patients (93.3%); 2 patients (4.4%) had a borderline result, while one patient (2.2%) was negative (Table I). Interestingly, one patient with a borderline result had a positive DIF, while the other patient and the patient with normal anti-TG2 levels also tested negative on DIF.
Serum levels of anti-TG3 IgA antibodies were above the cut-off level in 10 out of 45 patients (22.2%), 4 patients had borderline results (8.9%), while the remaining 31 were negative (68.9%) (Table I). Interestingly, all the patients with positive results at anti-TG3 IgA autoantibody testing, and 3 out of 4 patients with a borderline result, showed a positive DIF, while only one patient was negative. Moreover, all the controls tested negative for anti-TG3 antibodies, except by 2 in the control group 1.
Correlation of direct immunofluorescence results with clinical features, serology and anamnestic records
Of the 29 patients with a positive DIF, 15 had a previous history of muco-cutaneous diseases, while 14 did not. Correlation between a positive DIF and history of dermatological diseases in the past was close to, but did not reach, statistical significance (p = 0.08) (Table II). Of the 29 patients with a positive DIF, 13 (44.8%) had higher or borderline serum levels of anti-TG3 antibodies, while none of the 16 patients with negative DIF were positive at anti-TG3 testing and only one showed borderline values. The presence of anti-TG3 IgA autoantibodies correlated positively with the presence of granular deposits of IgA in the skin of patients with CD on DIF (p < 0.005) (Table II). DIF did not correlate with the presence of CD-associated symptoms nor with the Marsh degree at duodenal biopsy (Table II).
Table II. Association between demographic, clinical and serological characteristics of patients with direct immunofluorescence (DIF) results
Confocal microscopy
Intense double staining for both IgA and TG3 was found at the dermal papillae in 8 out of 10 patients with CD (Fig. 2). Interestingly, IgA and TG3 co-localized at the DEJ, at the dermal papillae (Fig. 3a–c). In the remaining 2 patients, while IgA staining was evident at the dermal papillae (Fig. 3d), TG3 staining was of weak intensity (Fig. 3e) and no significant co-localization between TG3 and IgA was detected (Fig. 3f). All the patients with CD were negative at TG2 staining. By contrast, none of the controls showed IgA, TG3 or TG2 staining at the DEJ or in the dermis. Physiological staining of TG3 of the stratum granulosum was found in the skin both of patients with CD and of controls.
Fig. 2. Double staining of IgA and epidermal transglutaminase (TG3) showing IgA/TG3 co-localization in the skin of a patient with coeliac disease, revealed by direct immunofluorescence (DIF). Green staining identifies IgA deposition; red staining identifies TG3 (note that positive staining of the uppermost epidermis results from physiological expression of TG3 in keratinocytes); yellow staining corresponds to IgA/TG3 co-localization.
Fig. 3. (a) Granular IgA (green staining) and (b) epidermal transglutaminase (TG3) (red staining) deposits at the dermal-papillae in the skin of a patient with coeliac disease (CD); (c) at double staining (yellow colour), IgA and TG3 clearly co-localize at the dermal papillae. (d) Granular IgA deposits (green staining) in the skin of another patient with CD; (e) in this case TG3 staining (red) was found to be of weak intensity and (f) IgA/TG3 co-localization was not documented.
In this case-control study, DIF could identify granular deposits of IgA, resembling DH, in the skin of two-thirds of patients with CD who had no previous history of DH nor active skin eruptions. Besides IgA, granular deposits of other immune-reactants, including IgM, C3 and IgG, were also observed, but with a lower frequency than IgA. Other studies have also reported similar findings in patients with DH, with granular IgM and C3 occurring with higher frequency than IgG (15–17). The pathological meaning of these immune-reactants in the pathogenesis of DH, as well as in the skin of patients with CD, remains elusive. Remarkably, granular deposits of IgG, IgM and C3 were also observed in some healthy controls. Among the healthy control group 2 (patients with a skin eruption associated with gastrointestinal manifestations unrelated to CD), 40% of the patients (all with eczematous eruptions) had granular deposition of C3 on DIF, in the absence of other immune-reactants. The pathological meaning of granular C3 deposits in the skin in the absence of immunoglobulin deposits is far less clear to date. DH-like or bullous pemphigoid-like skin eruptions with granular deposits of C3 on DIF have been described by Hashimoto et al., and regarded as granular C3 dermatosis (18). In that work, the author did not identify a link between the skin eruption and CD (18). Besides these immune-reactants, none of the controls showed granular deposits of IgA on DIF. Collectively, these findings suggest that IgA deposits represent a specific cutaneous finding of CD. This study expands and strengthens previous observations made by 2 separate studies: Cannistraci et al. reported granular deposits of IgA in the healthy skin of 9 patients with CD (8); thereafter, one study by our group reported granular deposits of IgA in the perilesional skin of 6 patients with CD with inflammatory skin diseases other than DH (9). Limitations of these studies included the low number of cases analysed and the absence of controls (19). The current study addressed both of these limitations, including a large series of patients and a similar number of controls. Indeed, the current study found that DIF was 100% specific, but showed 64% sensitivity for the diagnosis of CD. This value was consistently lower than that of serological tests and duodenal biopsies. Collectively, these findings suggest that DIF is less useful for diagnosing CD compared with the already existing tools. Furthermore, the current study was unable to identify specific correlations in the patient cohort between DIF positivity and clinical, serological or anamnestic findings, except for a high level of serum anti-TG3 IgA antibodies.
Although the association was not statistically significant, a high number of patients with positive DIF referred a previous history of dermatological diseases, in particular atopic dermatitis. The hypothesis that these patients might have had DH in the past and that DH was misdiagnosed as another kind of dermatosis, such as atopic dermatitis, can be excluded by the fact that remission of DH occurs only rarely without a long-term GFD (20, 21). Conversely, it is known that CD is significantly associated with skin disorders other than DH, including atopic dermatitis and psoriasis (22, 23). In particular patients with CD display a higher risk of skin diseases compared with the general population, with risks for eczema and psoriasis being the highest, followed by urticaria, vitiligo, acne, and alopecia areata (24). A recent study also found a significant association between DH, CD and atopic dermatitis during infancy (25). It is thus possible that chronic inflammation in the skin during childhood may lead to epidermal damage and exposure to TG3; production of IgA against TG3 could subsequently occur during the immune reaction to TG2 in the gut of patients with CD due to an epitope-spreading phenomenon.
The significance of granular deposits of IgA in the skin of patients with CD remains unclear. Dermal deposition of IgA is thought to be the primary disease-promoting mechanism of DH (4). TG3 is regarded as the main autoantigen of DH, since both IgA and TG3 were shown to co-localize in dermal aggregates of DH skin (5). Current evidence suggests that production of anti-TG3 IgA in DH begin in the gut, and then IgA circulates as immune complexes with TG3 and forms dermal aggregates in the skin (26, 27). The current study shows that these mechanisms may be not specific only for DH, but generally occur in patients with CD. Accordingly, the current study showed that in 8 out of 10 patients, IgA clearly co-localized with TG3 (but not with TG2). The hypothesis that IgA in the skin of patients with CD recognized TG3 as an antigen is further corroborated by the observed correlation between skin deposits of IgA and elevated levels of anti-TG3 IgA autoantibodies in patient sera. The results of the current study are in line with previous observations by Cannistraci et al. regarding IgA/TG3 co-localization in the skin of patients with CD, and contrast with those of our previous study regarding IgA/TG3 co-localization in the perilesional skin of patients with CD with non-DH inflammatory dermatoses (8, 9).
An important question is whether IgA aggregates identify patients with CD who are at risk of developing DH if they continue on a gluten-containing diet. Previous research suggests that development of DH is a matter of time, since it generally affects adults more than children (28,29); furthermore, early identification of CD due to a wide prescription of serological tests has led to a significant decrease in incidence of DH in recent years (30). However, the fact that the skin of patients with CD harbours the same immunopathological marker of DH suggests that, besides time, other factors may be required for DH to occur. The identification of these triggering factors would be a remarkable advance in the understanding of the pathophysiology of DH.
Limitations
The main limitation of this study is the lack of histological slides of previous dermatological diseases of patients with CD. Major strengths include the prospective and multicentric design, and the large number of patients and controls.
Conclusion
This study represents the largest case series investigating the rate of IgA deposits in the skin of patients with CD. Based on its observed low sensitivity, DIF may not play a prominent role in the diagnostic algorithm for CD. However, although further analyses are required to confirm these results, this study addresses granular deposits of IgA as an independent and highly specific cutaneous marker of CD.
The project was funded by a grant from the Italian Ministry of Health and from Regione Toscana (GR-2011-02346877).
Reviewed and approved by the institutional review board of Area Vasta Centro, Florence; approval SPE 14.167_ASF.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize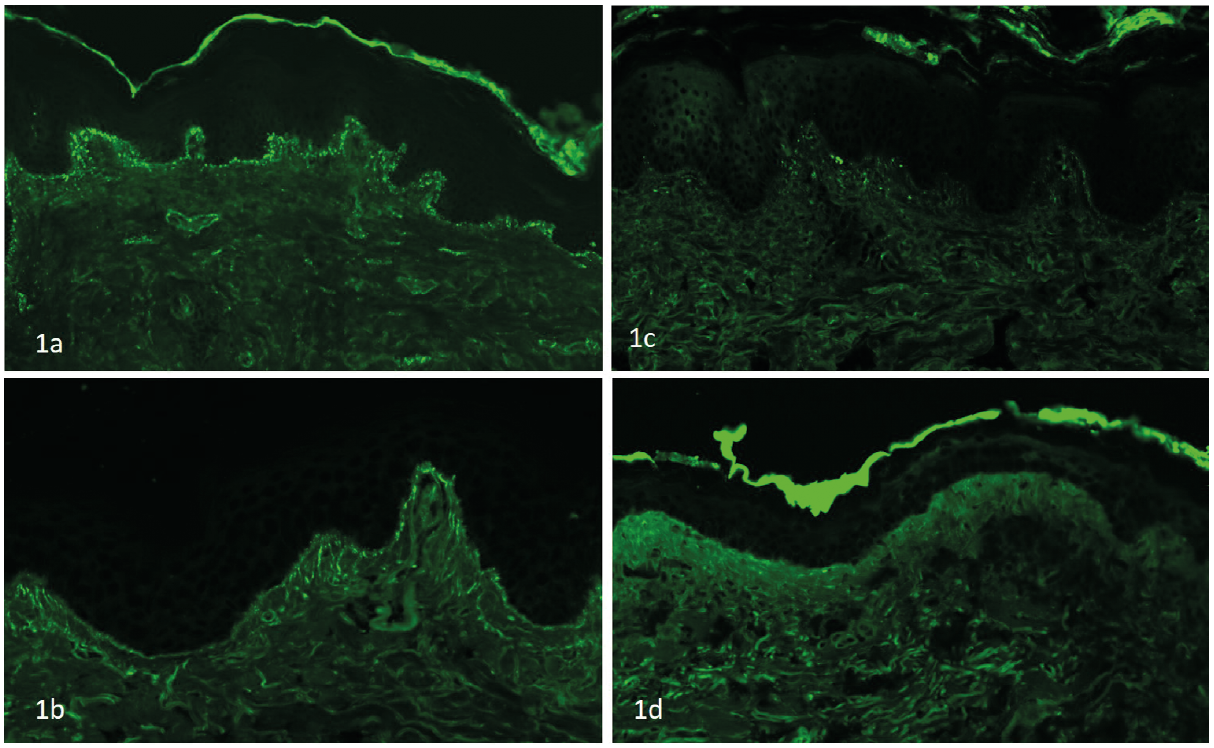 Click to show fullsize
Click to show fullsize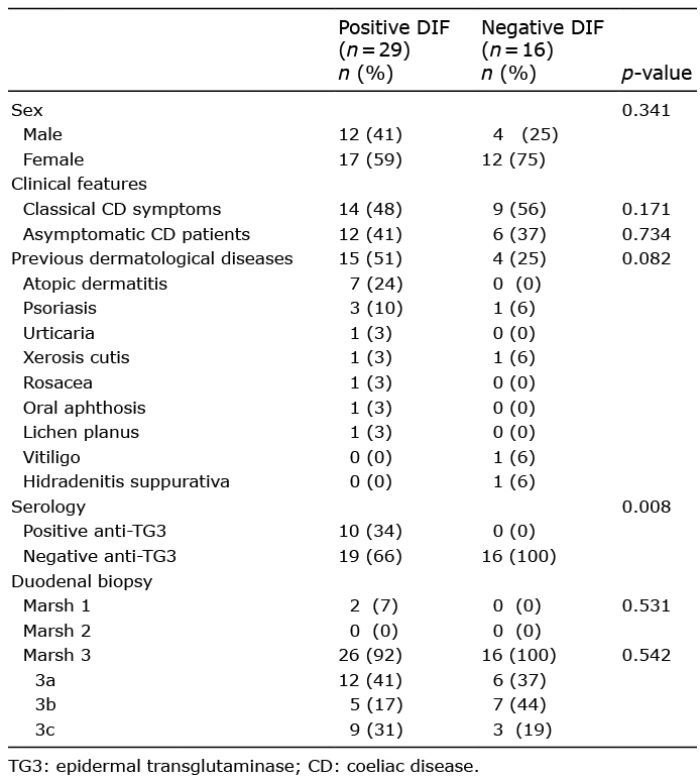 Click to show fullsize
Click to show fullsize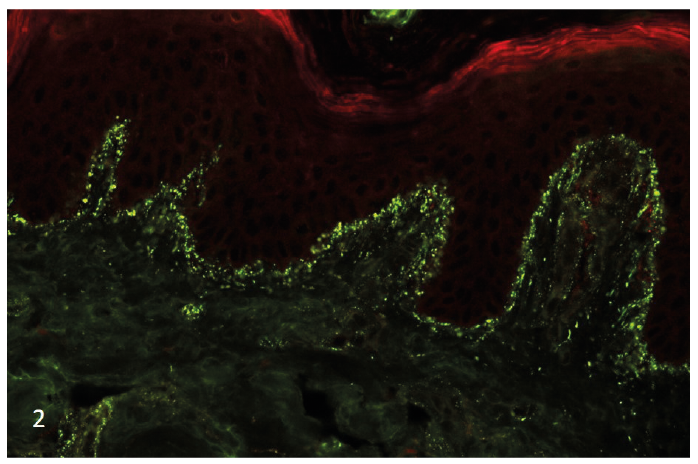 Click to show fullsize
Click to show fullsize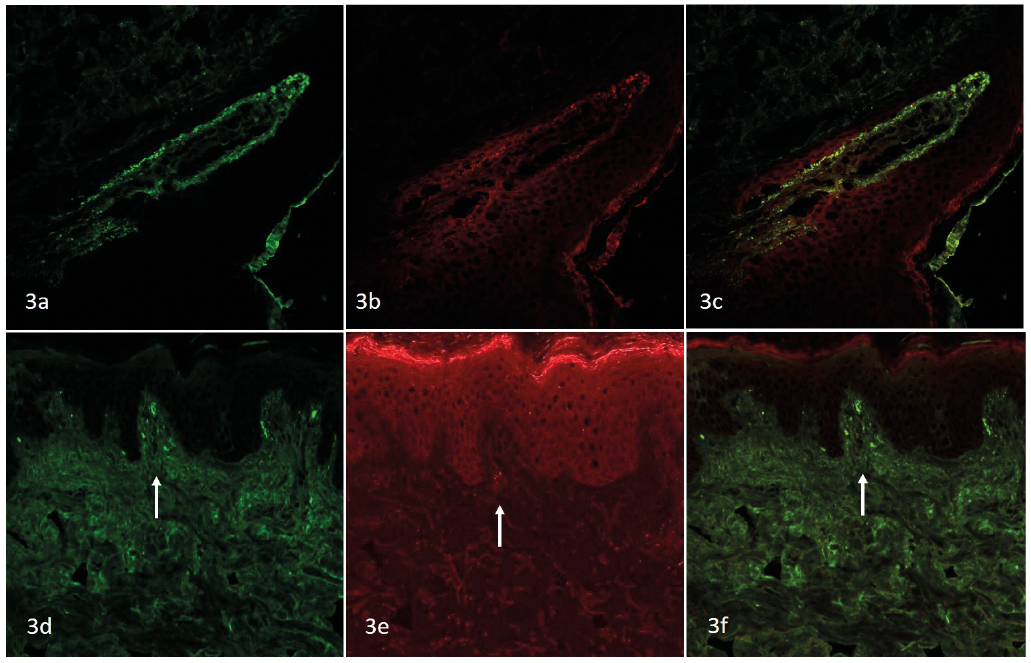 Click to show fullsize
Click to show fullsize