


1Department of Cardiology, 2Department of Dermatology and Allergy and 4Department of Clinical Physiology and Nuclear Medicine, Herlev and Gentofte Hospital, DK-2900 Hellerup, 3Department of Clinical Medicine, University of Copenhagen, 5Department of Clinical Physiology and Nuclear Medicine, Bispebjerg and Frederiksberg Hospital, Copenhagen, 6Department of Medicine, Division of Clinical Immunology, Icahn School of Medicine at Mount Sinai, New York, NY, USA and 7Department of Genetics and Genomic Sciences, Icahn School of Medicine at Mount Sinai, New York, NY, USA. E-mail: lilian.hannah.kaiser@regionh.dk
Accepted Jan 21, 2021; Epub ahead of print Jan 25, 2021
Acta Derm Venereol 2021; 101: adv00406.
doi: 10.2340/00015555-3752
Psoriasis is associated with increased risk of cardiovascular disease (CVD) and shares inflammatory mechanisms with atherosclerosis, the main contributor to CVD (1). Studies with 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT) have shown that patients with psoriasis have increased aortic vascular inflammation, an independent predictor of future CVD (2, 3). In addition, psoriasis severity has been associated with aortic inflammation independent of traditional cardiovascular risk factors, including hypercholesterolaemia (4). Statins are lipid-lowering drugs used for prevention of CVD and these agents decrease vascular inflammation in patients at increased risk of CVD (5). However, whether statins are linked with reduced vascular inflammation in patients with psoriasis is not known.
After informed consent, a total of 83 consecutive adult patients with plaque psoriasis with or without atherosclerotic CVD (myocardial infarction, stroke and/or peripheral artery disease) were recruited at our centre for a multiscale study of the association between CVD and psoriasis (regional ethics committee project ID H-17003458). All patients received intravenous 18F-FDG (3.5 MBq/kg) 120 min prior to whole-body 18F-FDG-PET/CT. Unenhanced low-dose CT images were used for anatomical correlation and 3-mm axial PET slices were manually placed around the external contour of the aorta to outline region of interests (ROIs) and were analysed using MIM 6.9.2 software (MIM Software Inc., Cleveland, OH, USA). The superior vena cava (VCS) was used to correct for background blood activity and vascular inflammation was quantitated in accord with established methods (5, 6). In brief, in each aortic segment a ROI was placed that encompassed both the aortic lumen and wall. The maximal standardized uptake value (SUVmax) of each slice of the ROI was divided by the SUVmean of the VCS to achieve the maximal target-to-background ratio (TBRmax). Moreover, the mean TBRmax was calculated from TBRmax values from all slices of each aortic segment. Most-diseased segments (MDSs) were found by detecting slices with the highest FDG uptakes and averages of TBRmax values were calculated for the adjacent 1.5 cm segments surrounding these slices. For statistical analyses, Welch 2-sample t-test, χ2 test, exact Wilcoxon-Mann-Whitney test, and multivariable regression models adjusted for sex, age and systemic antipsoriatic treatment were used, as appropriate. All analyses were performed with RStudio version 1.2.5033.
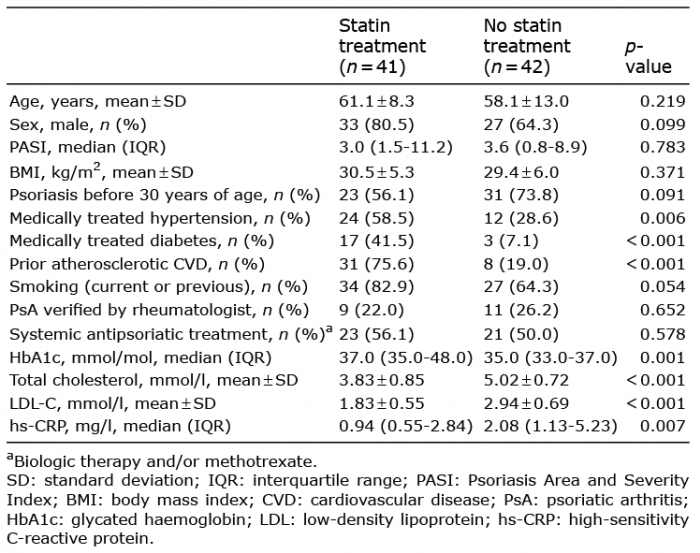
Characteristics of patients with psoriasis with or without statin therapy are shown in Table I. Mean age and Psoriasis Area Severity Index were not different between the 2 groups. As expected, patients who received statins were more likely to have a history of atherosclerotic CVD (75.6 vs 19.0%; p < 0.001), and to receive treatment for hypertension and diabetes. Also, levels of total cholesterol, low-density lipoprotein cholesterol, and the inflammatory biomarker high-sensitivity C-reactive protein (hs-CRP) were lower in the statin group, while glycated haemoglobin (HbA1c) levels were higher. In unadjusted analyses, vascular inflammation measured by FDG uptake (TBRmax and MDS) was nominally lower in the entire aorta and all individual aortic segments in patients treated with statins compared with those without statins, although these unadjusted results were not significant (Table II). After adjustment for age and sex, however, TBRmax was significantly lower in the ascending aorta and the aortic arch, and MDS was lower in the aortic arch, which was also apparent after adding adjustment for systemic antipsoriatic treatment in the model (Table II).
Table I. Characteristics of study patients with or without statin treatment
Table II. Vascular inflammation in patients with or without statin treatment
This study found that statin therapy was associated with decreased vascular inflammation in patients with psoriasis. Notably, most (75.6%) patients in the statin group had prior atherosclerotic CVD and in patients with psoriasis, favourable effects of statins on atherosclerotic plaque inflammation therefore do not appear to be mitigated by the presence of established CVD. In this regard, post hoc analyses from both primary and secondary prevention trials have indicated that statins improve CVD outcomes in patients with psoriasis irrespective of established vascular disease, and psoriasis is perceived as a CVD risk-enhancing factor in assessment of patients for cholesterol-lowering treatment (7, 8). In addition to their lipid-lowering effects, statins display pleiotropic anti-inflammatory actions and reduce hs-CRP levels, as also suggested by the data from the current study, but the role of lipid-independent mechanisms in statin-induced vascular effects remains to be determined (9).
Limitations of this study include that it was not a randomized trial, a control group of individuals without psoriasis was not included, some individuals declined study participation and this self-election may have introduced bias. In addition, there are technical limitations of 18F-FDG-PET/CT. The FDG uptake in inflammatory cells is influenced by, for example, fasting state, blood glucose and insulin levels, as well as the injected 18F-FDG dose. Moreover, imaging protocols and PET/CT scanner properties play a role. In the current study conditions were standardized by measuring blood glucose levels (all were below 11.1 mmol/l (10)), using weight-adjusted 18F-FDG dosing, and observing a fixed time interval between 18F-FDG injection and scanning. This study used TBR in attempt to compensate for individual differences in 18F-FDG excretion rates by correcting for background blood activity. In addition, reduction in vascular inflammation in the statin group was not significant in the unadjusted analyses in the aortic segments. However, significant differences were not least observed when adjusted for age, sex and systemic antipsoriatic treatment in the ascending aorta, where 18F-FDG-PET/CT measurements have shown good reproducibility and where vascular inflammation is predictive of future CVD independent of traditional risk factors (3, 5, 11).
In conclusion, the results of this study suggest that statins may be linked with reduced vascular inflammation in patients with psoriasis, and the results may support the case for use of statins in patients with psoriasis who are at increased risk of CVD.
Joel Dudley, PhD, and Brian Kidd, PhD, are acknowledged for support.
Funding: HK, AKH, XW, CB and PRH were supported by the LEO Foundation (grant no. LF16115).
Conflicts of interest: PRH is a recipient of a Borregaard Clinical Scientist Fellowship from the NOVO Nordisk Foundation and chairs a clinical academic group supported by the Greater Region of Copenhagen. CB is a consultant for Onegevity Health. LS has been a paid speaker for AbbVie, Eli Lilly and LEO Pharma, and has been a consultant or served on Advisory Boards with AbbVie, Janssen Cilag, Novartis, Eli Lilly, LEO Pharma, UCB, Admirall and Sanofi. She has served as an investigator for AbbVie, Janssen Cilag, Boehringer Ingelheim, AstraZenica, Eli Lilly, Novartis, Regeneron and LEO Pharma and received research and educational grant from Pfizer, AbbVie, Novartis, Sanofi, Janssen Cilag and Leo Pharma.


 Click to show fullsize
Click to show fullsize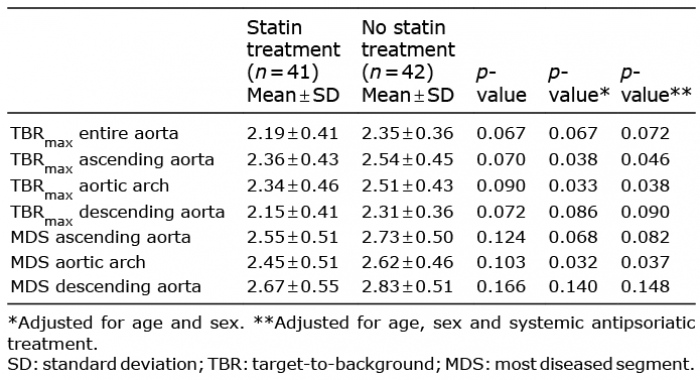 Click to show fullsize
Click to show fullsize