


1Department of Dermatology, Venereology and Allergology, Helios St Elisabeth Hospital Oberhausen, University Witten/Herdecke, Josefstr. 3, DE-46045 Oberhausen, 2Institute of Virology, National Reference Center for Papilloma- and Polyomaviruses, University of Cologne, Cologne, and 3Institute of Pathology, Mülheim an der Ruhr, Germany. E-mail: alexander.kreuter@helios-kliniken.de
Accepted Jan 26, 2021; Epub ahead of print Feb 1, 2021
Acta Derm Venereol 2021; 101: adv00358.
doi: 10.2340/00015555-3756
Penile carcinoma is a rare tumour, accounting for less than 1% of male cancers. Approximately 50% of penile cancers and 80% of their precursor lesions (penile intraepithelial neoplasia) are associated with high-risk human papillomavirus (HPV) infections, predominantly with HPV16 (1). HPV-independent penile cancers develop in the background of chronic inflammatory genital diseases, such as lichen sclerosus or lichen planus. Immunohistochemical overexpression of p16ink4a and low p53 staining in HPV-positive lesions are markers of viral transformation, whereas p53 expression combined with p16ink4a negativity identifies non-HPV-induced cancers (2). We report here a case of penile carcinoma associated with HPV68 in a patient who received long-term (photo)chemotherapy for treatment of psoriasis. HPV68 is a relatively rare HPV-type that has been classified as “probably carcinogenic” and accounts for only 0.1% of cases of cervical cancer (3).
A 75-year-old Turkish man, with a history of psoriasis for more than 50 years, presented with an indurated plaque on the glans penis. He had been circumcised in childhood for cultural reasons. The current penile lesion had developed within the previous 2 months and was slowly enlarging. The patient was a non-smoker and had no history of genital trauma, anogenital infections including sexually transmitted diseases, no genital affection of psoriasis, and no previous arsenic or radiation therapy. However, his psoriasis had been treated in the past with psoralen and ultraviolet A (PUVA) photochemotherapy (cumulative PUVA dose 1,500 J/cm2) and narrowband (NB)-UVB phototherapy (cumulative dose 200 J/cm2) combined with oral low-dose methotrexate (15 mg per week) for more than 5 years. He reported that most of the phototherapy sessions were performed without protection of the genital area. In the last 5 years, several epithelial skin cancers including 3 squamous cell carcinomas (SCC), 4 basal cell carcinomas, 6 Bowen’s disease lesions, and numerous actinic keratoses were surgically excised from various non-genital UV-exposed body sites, including the head, trunk and extremities. His further medical history was unremarkable, HIV testing was negative, and lymphocyte subpopulations were within normal range. After histopathological confirmation of a highly-differentiated penile SCC with a tumour thickness of 2.2 mm and lymphangiosis carcinomatosa with D2-40-positive lymphatic vessels, a partial amputation of the glans penis was performed.
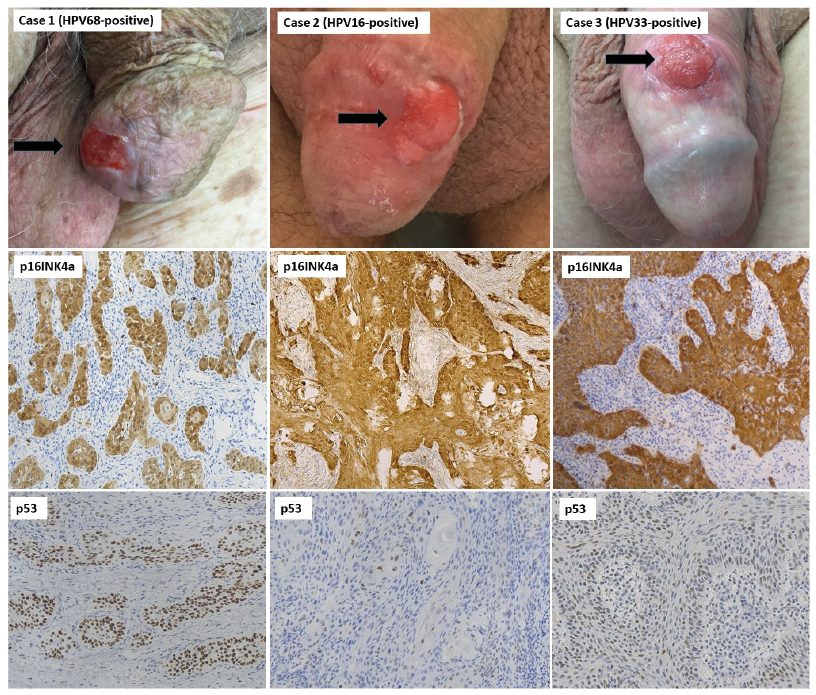
HPV analyses using alpha-group-specific PCR and reverse line blot hybridization revealed a mono-infection with HPV68 (INNO-LiPA HPV Gentotyping Extra II, Fujirebio, Ghent, Belgium). In situ hybridization showed nuclear HPV68-DNA positivity within the tumour cells. As expected, immunohistochemical analyses demonstrated overexpression of p16ink4a, and interestingly, also strong nuclear accumulation of p53 in virtually all tumour cells (Fig. 1, case 1). In contrast, 2 penile cancers from non-PUVA treated patients, induced by HPV16 and HPV33, respectively, were found to be p16ink4a-positive and showed only a p53 wild-type pattern (Fig. 1, cases 2 and 3). Two further patients with carcinomas that developed in association with chronic inflammatory skin diseases, a vulvar carcinoma in a woman with genital lichen sclerosus, and a carcinoma of the tongue in a patient with oral lichen planus, demonstrated negative p16ink4a-staining, but strong positivity for p53 (Fig. S1).
Fig. 1. Clinical presentation and immunohistochemical analyses for p16ink4a and p53 of 3 penile carcinoma cases. Case 1: HPV68-associated penile carcinoma with both p16ink4a and p53-overexpression (original magnification ×100). Case 2: HPV16-associated penile carcinoma. Case 3: HPV33-associated penile carcinoma. Cases 2 and 3 demonstrate strong p16ink4a-expression, but a p53 wild-type staining pattern (original magnification ×100). Black arrows indicate the respective penile carcinomas.
Like NB-UVB, PUVA photochemotherapy is a highly effective and well-tolerated therapy for psoriasis. However, PUVA is both mutagenic and immunosuppressive, which increases the risk for developing cutaneous SCCs up to 80-fold compared with the normal population (4). Psoriasis patients treated with PUVA have a 95.7 times increased risk of developing invasive penile cancer compared with the general population (5).
Halec et al. assessed the expression pattern of p16ink4a and p53 in HPV68-positive cervical cancer tissues by immunohistochemistry, and demonstrated viral carcinogenicity (p16ink4a high, p53 low) (6). The E6 oncoprotein of HPV68 degrades p53 as efficiently as E6 of established oncogenic genotypes, such as HPV16 or HPV18 (7). In the literature, only a few cases of penile SCC associated with HPV68 mono-infection have been described (1, 8). Barzon et al. (8) have published a case with p16ink4a- and nuclear p53-positive staining. Unfortunately, it is not reported whether this patient was regularly exposed to UV radiation (8). The strong p16ink4a-positivity of the present penile carcinoma together with the accumulation of nuclear p53, that has not been degraded by HPV68-E6, points towards the presence of mutant p53 generated by PUVA-induced p53 gene mutations (4). It is possible that this multifactorial oncogenesis may explain the relatively fast and aggressive tumour development within 2 months in the current case. Synergistic effects of oncogenic risk factors in HPV-associated carcinogenesis have been reported previously, e.g. interaction of HPV with other viruses, tobacco use in HPV16-associated oropharyngeal squamous cell carcinoma, and UV-light and beta-HPV in epithelial skin cancer (9–11). To the best of our knowledge, this is the first report of a possible pathogenetic role of PUVA and HPV in penile carcinoma.
In conclusion, these findings are suggestive of a dual-track pathway of carcinogenesis, with HPV68-driven oncogenesis augmented by the mutagenic effects of UV light. One could speculate that the presence of a further mutagen (here UV light) may enhance the carcinogenicity of probable high-risk HPV-types, such as HPV68. Clinical examination of psoriasis patients with a history of long-term phototherapy should always include the anogenital region, especially if PUVA has been performed without appropriate genital protection.
The authors thank Monika Junk, Anke Bartröver, Tanja Kleinecke, Silke Bolz, and Stefanie Fittkau for excellent technical assistance.
HPV analyses were funded by the German National Reference Center for Papilloma- and Polyomaviruses (German Federal Ministry of Health, grant number 1369-401). M.H. was funded by Deutsche Krebshilfe (grant number 70112727).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize