


1Institute of Dermatology, IRCCS Policlinico San Matteo Foundation Pavia, P.le C. Golgi, 2, IT-27100 Pavia, 2Dermatology Unit, Department of Health Sciences, ASST Santi Paolo e Carlo, 3Department of Pathophysiology and Transplantation, University of Milan, and 4Division of Pathology, Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italy. *E-mail: vbrazzelli@libero.it, v.brazzelli@smatteo.pv.it
Accepted Feb 2, 2021; Epub ahead of print Feb 8, 2021
Acta Derm Venereol 2021; 101: adv00398.
doi: 10.2340/00015555-3761
Eruptive pseudoangiomatosis (EPA) is an acute, spontaneously regressing rash, first described by Cherry et al. (1) in 1969. The clinical presentation consists of angioma-like papules, a few millimetres in diameter, frequently surrounded by an anaemic halo (1). Histology of EPA is characterized by dilated blood vessels in the upper dermis with no increase in their number; hence the term “pseudoangiomatosis” (2).
EPA can affect both children and adults (1, 3). The disease course is benign with spontaneous resolution within a few weeks, although recurrences are not uncommon (3). There appears to be a seasonal correlation, with most cases occurring in summer (1, 5, 6). The exact aetiopathogenesis of EPA remains unknown; possible causes include viruses, mosquito bites, flea bites, certain foods, and drugs (4–7).
The aim of the study was to retrospectively evaluate the epidemiological, clinical, and histopathological characteristics of 20 adult patients with EPA, which occurred as small outbreaks in different hospital departments.
A continuous series of 20 patients, who were inpatients in different hospital departments at Foundation IRCCS Policlinico San Matteo Pavia, Italy, were retrospectively studied for other diseases or programmed surgical procedures. All patients were examined by a dermatologist (VB or CV). Diagnoses were confirmed on the basis of clinical presentation and histological findings. Data were collected on age, sex, season in which lesions occurred, comorbidities, lesion location, presence of any prodrome or recurrences. A punch biopsy was performed for histological examination in all patients. Serologies and viral isolations for human herpes virus 6 (HHSV 6), human herpes virus 7 (HHSV 7), parvovirus B19, Epstein-Barr virus (EBV) and cytomegalovirus (CMV) were performed. The study was conducted according to ethical guidelines and the principles of the Declaration Helsinki.
The patients’ clinical characteristics are shown in Table SI. The age of the patients ranged from 37 to 88 years (mean age 66.7 years). A female predominance was observed, with a female-to-male ratio of 3:1. All of the cases occurred during the summer months of July and August.
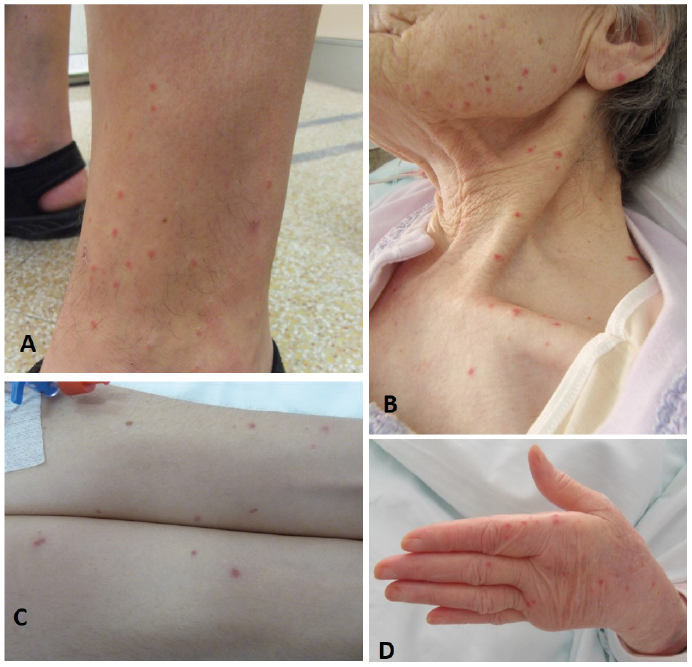
All patients developed typical monomorphic lesions (Fig. 1). Most of the lesions were located on the extremities (75%; Fig. 1A, C, D), followed by the face (45%; Fig. 1B), trunk (15%), neck and décolletage (15%). None of the patients experienced prodromal or any associated systemic symptoms. Spontaneous resolution of the lesions occurred in all patients within 7–20 days.
Fig. 1. Four different patients with small, angioma-like, erythematous lesions on different body sites. The lesions are monomorphous and identical in all 4 patients. (A) Small papular lesions located on the lower extremities surrounded by prominent anaemic halo. (B) Identical papular lesions located on the face, neck, and décolletage. (C) Erythematous-violaceous papules located on the ventral aspect of the forearms. (D) Typical eruptive pseudoangiomatosis lesions located on the dorsal aspect of the hand.
Histology revealed blood vessel dilatation, mainly in the upper dermis, and plump endothelial cells with prominent nuclei (Fig. S1A, B). No epidermal changes or blood vessel proliferation were observed. A limited, focal extravasation of red blood cells was observed, as well as a scant inflammatory infiltrate, represented mainly by lymphocytes (Fig. S1C). Rarely, intravascular neutrophils were observed (Fig. S1C, D).
Eight patients showed positive anti-parvovirus B19 IgG antibodies and 2 of these also had positive IgM and circulating parvovirus B19 DNA. One patient was positive for circulating HHSV7 DNA, while 2 patients were positive for anti-CMV IgG antibodies. One patient was positive for Proteus mirabilis on haemoculture.
EPA was first documented in children and is considered as a childhood rash; however, an increasing number of cases have been reported in adults to date. The aetiology of EPA is not clear, despite earlier cases being associated with viruses (1, 2). The distinct clinical and histological appearance of EPA has led several authors to consider it as a viral or paraviral eruption (1, 2, 4, 7). This concept of paraviral eruptions has been applied to clinically well-defined and recognizable eruptions (e.g. Gianotti-Crosti syndrome, asymmetric periflexural exanthem in childhood, gloves and socks disease) which have many causes, including at least one clearly identified viral infection or reactivation. Circulating parvovirus B19 DNA was found in 2 of our patients who were also positive for anti-parvovirus B19 IgG and IgM. This is an interesting aspect, because it suggests evidence in favour of a viral reactivation and the consequent induction of skin manifestations. However, this is only a hypothesis, and would be the first association between EPA and parvovirus B19 reported in the literature.
Regarding the pathogenesis of EPA, it has been hypothesized that capillary dilatation could be the result of virus localization and proliferation within the endothelial cells or an indirect effect following an antigen-antibody complex formation at the vascular level (1, 2). The papular component may be due to concomitant perivascular oedema with an anaemic halo. In order to confirm viral presence in endothelial cells, Prose et al. (2), Neri et al. (8) and Misery et al. (9) performed electron microscopy, but no conclusive evidence was obtained regarding the presence of viral particles.
Some authors have attributed EPA to mosquito bites, given the acral localization and seasonal correlation, suggesting that immunosuppression, ageing, or exposure to a high number of bites may modify the immune reaction (6, 10). Oka et al. (10) performed mosquito bite experiments to reproduce EPA lesions, concluding that the lesions were an age-dependent desensitization to mosquito bites; however, they did not report histological findings. Furthermore, this explanation does not account for cases in childhood. In particular, typical mosquito bites appear as pruritic polymorphous pink papules, often with a central punctum. Despite our patients being affected by a range of different comorbidities, with a wide spectrum of immune statuses, the clinical aspect of the lesions was always monomorphous without pruritus, suggesting that the immune status does not appear to play a significant role in the evolution of EPA. The limited role of the immune status in EPA is also confirmed in the literature (11, 12). In our opinion, histology is essential to diagnose EPA, along with the clinical appearance of the lesions, since, together, they form a highly distinctive clinical picture.
Differential diagnosis is represented mainly by reactive angioendotheliomatosis (RAE), malignant angioendotheliomatosis (MAE), papular urticaria, and adrenergic urticaria (13–15). RAE can be differentiated on the basis of clinical findings such as variable presentation of lesions, blood vessel proliferation, and symptoms. such as pain and ulceration, which have never been reported for EPA (13). MAE differs from EPA due to its clinical presentation, poor prognosis, and the presence of atypical intravascular B lymphocytes (14). Lesions are highly transient and pruritic in adrenergic urticaria, whereas EPA lesions last a few weeks or longer and are rarely pruritic (15).
The inherent limitations of a retrospective case series must be considered for the current report, such as lack of controls, inability to assign causality, and incomplete/missing data for some patients who were subsequently not included in the paper. In the current report, transmission among patients sharing the same rooms, monomorphism of the lesions, and a good prognosis with spontaneous resolution in all cases are perfectly coherent with the literature and point to a viral/paraviral origin, although it is still unclear whether viruses play a direct pathogenetic role or whether lesions could be considered as paraviral manifestations. In particular, we report here a possible association with parvovirus B19 infection, which, to the best of our knowledge, has not been reported previously.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize