


Department of Pathophysiology and Transplantation, Università degli Studi, Foundation IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy. E-mail: stefano.veraldi@unimi.it
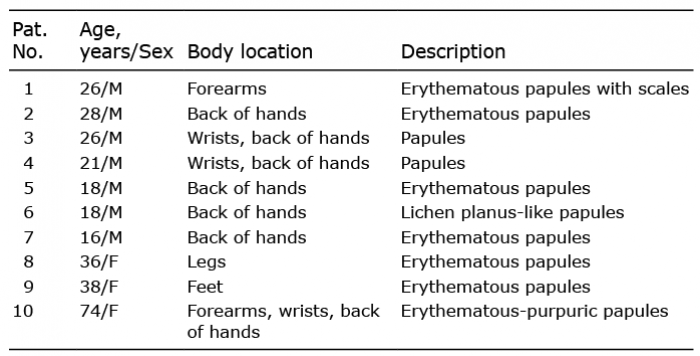
We read with interest the paper by Brin et al. (1) on a case of Gianotti-Crosti syndrome in an adult patient with coronavirus disease-19 (COVID-19). From March 2020 Milan and the Lombardy region (Northern Italy) have experienced an outbreak of severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) with a very high number of infected people and deaths. From March to December 2020, we have observed a high number of patients with COVID-19 with different skin manifestations. Among them, we have observed 10 patients with acrodermatitis. These patients were 7 males and 3 females, age range 16–74 years (mean age 30.1 years). The hands were affected in 7 patients, wrists in 3, forearms in 2, and legs and feet in one patient each. Erythematous papules were the most frequent clinical presentation (Table I, Fig. 1). Itching was mild or absent. In 8 out of 10 patients, acrodermatitis occurred from 5 to 12 days before the appearance of the first clinical manifestations of COVID-19. The latter were headache, cough, fever (< 38.2°C), arthralgia, myalgia and weakness. One patient reported abdominal pain and diarrhoea.
Table I. Patients’ characteristics
Fig. 1. Clinical photographs. (A) Patient 1. Erythematous papules with scales on the forearm. (B) Patient 8. Erythematous papules on the lower leg.
Nasal/pharyngeal swabs were positive for SARS-CoV-2 RNA in all patients. For organizational reasons linked to the outbreak, biopsy was performed in only one patient. The epidermis of the wrist showed mild hyperkeratosis, focal parakeratosis, acanthosis and spongiosis. In superficial and mid dermis, a perivascular infiltrate, consisting mainly of lymphocytes with some histiocytes, was observed.
All patients were followed at their homes and treated only with paracetamol. No therapy was prescribed for skin lesions. Complete remission of both cutaneous and systemic clinical manifestations was detected within 3 weeks in all patients.
Published data on Gianotti-Crosti syndrome in patients affected by COVID-19 are very limited. Some cases of acral lesions have been reported (2–5); however, none of them were typical cases of Gianotti-Crosti acrodermatitis. Based on our group of 10 patients, we can state that: (i) acrodermatitis frequently occurred some days before the appearance of the first clinical manifestations of COVID-19; (ii) acrodermatitis seemed to be more frequent in young males; (iii) COVID-19 in these cases was of mild severity.
Hôpital Cochin, Assistance Publique-Hôpitaux de Paris, Department of Dermatology and Venereology, AP-HP Centre-Université de Paris, Paris, France
We thank Veraldi et al. for their interest in our case report. Their letter demonstrates that acrodermatitis can be observed in the setting of COVID-19 and must be added to the various skin manifestations associated with SARS-CoV-2 infection. We have read their report with care, and would like to add some comments, as we notice some differences between their cases and our observation.
In our case, the rash occurred late after the symptoms resolved, and the nasopharyngeal PCR was negative while the serology was positive, which seems to be different from the patient descriptions reported by Veraldi et al. The rash was very itchy and associated with increased eosinophilia in the blood, and the improvement was slowly favourable with topical steroid treatment.
Vesicular lesions have been described in the course of COVID-19 disease, mostly as a rash in middle-aged patients, and with acral localization in young patients (1, 6). Surprisingly, in our patient the rash predominated on the extension faces of the limbs, sparing the hands and feet.
However, in agreement with the cases reported by Veraldi et al., in our case, the rash occurred in a young man and was associated with a moderate form of COVID-19.


 Click to show fullsize
Click to show fullsize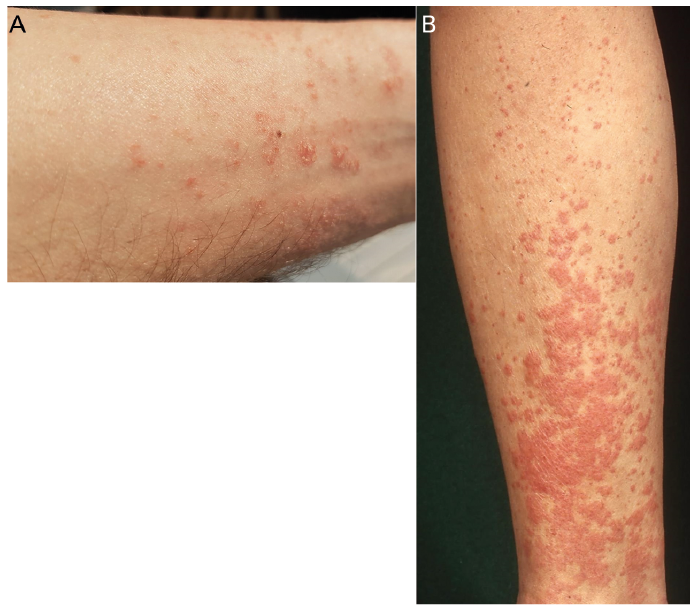 Click to show fullsize
Click to show fullsize