


1Faculty of Health Science, University of Southern Denmark, Odense, 2HAE International (HAEi), Horsens, Denmark, 3Department of Dermatology and Allergy, Comprehensive Allergy Centre Charité, Charité – Universitätsmedizin Berlin, Berlin, Germany, 4Allergy Department, Hospital Universitario La Paz, 5Hospital La Paz, Institute for Health Research (IdiPaz), 6Center for Biomedical Research Network on Rare Diseases (CIBERER U754), Madrid, Spain, 7Department of Clinical Research, Faculty of Health Science, University of Southern Denmark and 8Department of Clinical Genetics, Odense University Hospital, Odense, Denmark
Angioedema and hereditary angioedema are characterized by swelling of the subcutaneous and/or submucosal tissue, resulting in localized oedema. The rarity, but also the diverse clinical presentation, of these conditions can be challenging regarding diagnosis, treatment, and management. Patient-reported outcome measures (PROMs) are data received directly from the patient, providing the patient’s perspective on various subjects regarding health and well-being. PROMs can be helpful tools to optimize treatment and long-term management of conditions. A major challenge regarding the consistent use of PROMs in clinical settings in Scandinavia is language availability; many of the validated PROMs for hereditary angioedema and angioedema lack translations into the Nordic languages. The litterature search yielded 9 different PROM tools for angioedema and hereditary angioedema. Five were found suitable for use in clinical practice in Europe. Even though several PROMs exist they are not used consistent. Accessible electronic PROMs and careful planning is required to implement PROMs optimally in routine care processes.
Key words: hereditary angioedema; angioedema; patient-reported outcome measure.
Accepted Mar 10, 2021; Epub ahead of print Apr 21, 2021
Acta Derm Venereol 2021; 101: adv00456.
doi: 10.2340/00015555-3807
Corr: Anna Trier Heiberg Brix, Faculty of Health Science, University of Southern Denmark, DK-5000 Odense, Denmark. E-mail: anbri14@student.sdu.dk
This article reviews the patient-reported outcome measures available for angioedema and hereditary angioedema, and assesses their availability in the Nordic languages. Patient-reported outcome measures have immense possibilities when used consistently and systematically in clinical practice, ultimately providing patients with better, and more personalized, care. This review provides an overview of clinically relevant PROM tools for angioedema and hereditary angioedema and where they can be accessed.
Angioedema (AE) is a clinical symptom characterized by self-limiting swellings of subcutaneous or submucosal tissue, resulting in localized, often non-pitting, oedema. The swellings are unpredictable, and the frequency, location and severity of swellings vary between patients and intra-individually (1, 2). AE develops over several hours and resolves spontaneously within a few days if not treated. The typical locations are face, lips, tongue, extremities, genitalia, upper airways or abdomen (3, 4).
AE can be accompanied by wheals, or may be primary (monosymptomatic) AE without wheals (3, 5). The swelling is a consequence of increased vascular permeability induced by different vasoactive mediators, such as histamine or bradykinin. Histaminergic AE and urticaria can be treated with antihistamines, while non-responders to high-dose antihistamines often benefit from omalizumab as long-term prophylaxis (6, 7). Acute attacks of bradykinin-mediated AE can be treated with icatibant, which is a bradykinin B2 receptor antagonist, or complement C1-inhibitor (C1-INH) concentrates, which are advanced orphan drugs licensed for use in hereditary angioedema (HAE) (5, 8, 9). Long-term prophylactic treatment is indicated in severe cases, mostly patients with HAE. Prophylactic treatments of bradykinin- mediated AE include complement C1-inhibitor concentrates, or lanadelumab, which is a human monoclonal antibody targeted against plasma kallikrein (8, 9). Additional drugs for the treatment of patients with HAE are the kallikrein inhibitors ecallantide and berotralstat, but these are not yet available in Europe.
HAE is a rare genodermatosis with potentially life-threatening swelling attacks (8–10). The pathogenesis of HAE types I and II is related to extensive bradykinin release due to deficiency or lack of function of C1-INH. HAE with C1-INH deficiency is associated with disease-causing variants in the SERPING1 gene. A more recently described subtype of HAE is HAE with normal C1-INH, in which mutations in genes encoding factor XII, angiopoietin, plasminogen, myoferlin and kininogen-1 have been identified in some patients (11, 12).
The severity and unpredictable pattern of diseases with recurrent AE, along with painful and often disabling swellings, results in impaired health-related quality of life (HRQoL), which describes the patient’s emotional, social and physical well-being (13–16). Patients may have, or may develop, anxiety and depression as important associated disorders (17, 18).
In recent years there has been an increased focus on patients’ perspectives on their health and well-being, recorded with the help of PROMs (19). PROMs capture data directly from the patient, without interference from the physician (or any other healthcare professional). They provide useful knowledge about the patients’ own assessment of their disease situation, which can be used to improve disease activity, disease control and HRQoL, enhance patient–physician communication and thereby possibly increase patient satisfaction (19, 20). PROMs can also be important target parameters to tailor individual treatment needs and refine management of conditions. When used repetitively in the same patients, PROMs can also improve the assessment of treatment effectiveness. Finally, PROMs are important outcome measures in clinical trials.
The potential of a structured and consistent use of PROMs to monitor, evaluate and optimize treatment and HRQoL is promising, but requires work and appropriate management of workflow to implement in clinical routine. For patients with AE or HAE, 6 different outcome tools have recently become available, as reported below.
This is a narrative review. A literature search for published data regarding PROMs for AE and HAE was performed in PubMed, with the following terms “hereditary angioedema”, “angioedema”, “HAE”, “oedema” both alone or combined with “patient-reported outcomes”, “PROMs”, “PROM”, “health-related quality of life” and “HRQoL”. Studies using only generic tools, such as EuroQoL5, SF12, SF36 or VAS scale, were excluded. Studies using non-validated, study-specific questionnaires to access PROMs were also excluded. Nine different HAE/AE-specific tools were found, described in 9 articles (21–29), and 2 reviews of PROMs for HAE with a different focus (15, 16). The start date was June 5, 2020, and end date of the search was November 2020.
Angioedema tools
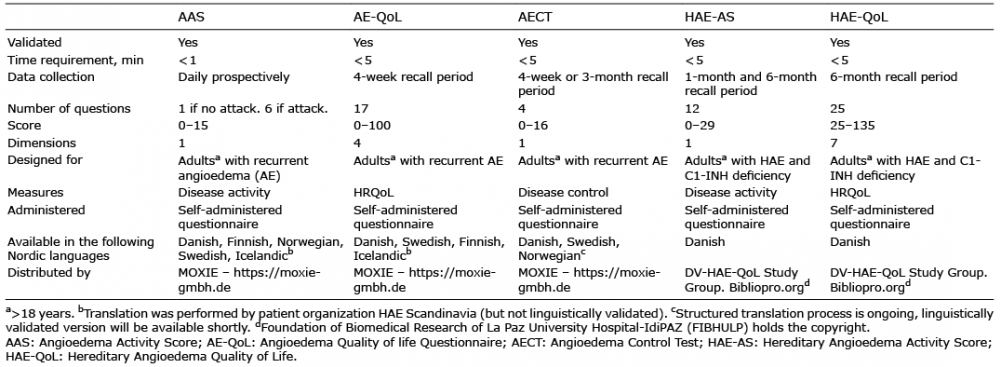
Validated instruments developed for AE are the Angioedema Activity Score (AAS) (21), Angioedema Quality of life Questionnaire (AE-QoL) (22), and the Angioedema Control Test (AECT) (23) (Table I). These instruments can be used in all forms of recurrent AE, including HAE.
Table I. Patient-reported outcome measures (PROMs) for recurrent angioedema
The AAS is a short daily, diary-type questionnaire that prospectively assesses daily AE activity and can be performed in less than 1 min. If AE is present, the patient needs to answer 5 additional questions, each scored 0–3. Cumulative data from 4 consecutive weeks provides a valid assessment of disease activity (21). The AAS has been translated into all Nordic languages.
The AE-QoL is a short 17-item questionnaire designed to retrospectively assess HRQoL, with a recall period of 4 weeks. Its results can be displayed as a total score or as 4 domain scores. The scores each range from 0 to 100, after linear transformation of raw values (22), with higher scores indicating higher HRQoL impairment. Linguistically validated versions of the AE-QoL are available in Danish, Swedish, and Finnish.
The patient organization HAE Scandinavia has translated AAS and AE-QoL to Icelandic. However, the Icelandic versions are not yet validated.
The AECT monitors disease control retrospectively, with a recall period of 4 weeks or 3 months. The validation shows that the results are largely similar between the 4-week and the 3-month recall period, and the physicians can choose which recall period suits the individual setting (24). The AECT comprises 4 questions, is quick to complete, and can be used easily in clinical practice as a routine tool to monitor disease control (23, 24). The AECT is available in Danish and Swedish, and a translation process to Norwegian is currently ongoing.
The AAS, AE-QoL and AECT are all available to physicians free-of-charge (from www.moxie-gmbh.de).
Hereditary angioedema specific tools
HAE-specific validated PROMs include the Hereditary Angioedema Activity Score (HAE-AS) (25) and Hereditary Angioedema Quality of Life (HAE-QoL) (26).
The HAE-AS is a retrospective questionnaire with 12 questions assessing disease activity, with a recall period of 1 month for 2 questions and 6 months for the remaining 10 questions (25).
The HAE-QoL is a retrospective questionnaire with a recall period of 6 months. It contains 25 questions grouped into 7 categories, assessing treatment difficulties, physical functioning and health, disease-related stigma, emotional role and social functioning, concern about offspring, perceived control over illness and mental health (26).
HAE-AS and HAE-QoL were developed in Spain and have limited Nordic language availability. HAE-QoL is available in 18 languages, with Danish being the only Nordic language. HAE-QoL is available to physicians free-of-charge (from www.bibliopro.org/).
The Hereditary Angioedema Patient Reported Outcome (HAE PRO) (27), was developed for use in the Icatibant outcome study. In contrast to the other tools described, HAE-PRO is completed when the patient has an attack of HAE. After e-mail correspondence with Shire/Takeda, we were not able to access the HAE PRO, and the tool is not described further here.
Physicians in the USA may use the Hereditary Angioedema Association (HAEA-QoL) questionnaire. Since this tool is developed specifically for the medical system in the USA, it is not described further here (28).
The Mean Symptom Complex Severity (MSCS) and the Treatment Outcome Score (TOS) (29) are disease-specific, validated tools, which provide a composite score regarding the severity of an attack at a given time (e.g. baseline, prior to administration of a study medication, time-period after drug administration) and the treatment response (TOS). The tools have been used only for ecallantide, and are therefore not ideal for regular monitoring of patients with HAE. The tools are complex and not suitable for routine use in clinical practice; therefore they are not described in detail here.
Diagnosis, management and treatment of AE can be complicated, as AE includes several subtypes with different pathophysiological backgrounds. Management of HAE is a lifelong and challenging process, involving many factors, including hereditary aspects. Several advanced orphan drugs are licensed for use in HAE and should be used conscientiously in patient care, primarily with a focus on efficacy and safety, but also with a regard to drug expense (30, 31). In order to individualize and optimize treatment of HAE, physicians need information not only on the severity and frequency of attacks, but also on the impact of the disease on patients’ lives. The divergence in how physicians and patients with chronic illnesses understand disease severity and activity is well known (16). To our knowledge, no disease-specific PROM for angioedema exists for children (<18 years old). HRQoL have been investigated in children with HAE (32, 33), with the generic Pediatric Health-Related Quality of Life 4.0 Generic Core scales (34), with diverse results (32, 33). In addition, a children’s version of the Dermatology Life Quality Index (DLQI) is available and may be applied in children with recurrent AE (35).
In order to personalize treatment, it is meaningful to monitor disease activity, disease control and HRQoL on a consistent basis. It is also important to integrate PROMs into the electronic medical health record. The AECT has recently been approved in an electronic version (in German), but the rest of the tools described here are available only in printed form. The paperwork and the time needed to complete the questionnaires can be a challenge to fit into the daily life of patients and time-consuming for treating physicians. Thus, electronic versions could be a better way of collecting PROMs (36). Digitizing the questionnaires, making it fast, easy to use, and available on the patients preferred device, is key to unlocking the value of PROMs, as useful tools in managing and optimizing patient care.
Another important issue is the language in which the PROMs are available. Five questionnaires are available in Danish, 3 out of 5 are available in Swedish, 2 out of 5 are available in Finnish, but only the AAS is available in all Nordic languages; however, it is not linguistically validated in Icelandic. Translation and cultural adaption can be a time-consuming process (37–40). It is recommended to follow a structured process of forward and backward translation, followed by pre-testing of the instrument and cognitive interviewing (cognitive debriefing). Reconciliation, cognitive debriefing and validation ensure that the meaning and function of the PROM is not lost during the translation process (38, 39). Each country may also need PROMs in languages other than their national language. For example, the Danish HAE Centre serves patients from Germany, Norway, Portugal, Hungary, Turkey, Syria and Pakistan (41); hence, to be successful with the use of the PROM tools in the entire patient group, the range of language availability needs to be expanded. Cultural adaption, along with translation, is often necessary to ensure that the aim is conserved in translation, via scaling or replacing items to ensure that it is equivalent relevant and valid in a new culture (38–40). Each country differs in terms of how the medical system is organized, which is why the USA use their own QoL tool for patients with HAE (28).
If used correctly and consistently as a monitoring tool, it is expected that PROMs will help the refine individual treatment and may also reduce the annual cost of medication per patient, by enabling a better overview of treatments that provide “value for money”.
In April 2020 the Global Allergy and Asthma European Network (GA2LEN) and HAE International (HAEi) launched a new concept: Angioedema Center of Reference and Excellence (ACARE), with inspiration from other successful GA2LEN networks. To certify as an ACARE unit, a total of 32 requirements in 5 domains must be fulfilled (42). The use of PROMs is highlighted and, in order to successfully certify as an ACARE centre, documentation of consistent use of at least 1 tool in 80% of the patients with recurrent AE must be present.
In addition, valuable information is collected through PROMs, which can be used in general quality improvement and research.
In conclusion, PROMs for use in monitoring and managing patients with HAE have been developed and validated, but are not yet used on a regular basis in the management of HAE in the Nordic countries. The potential use of PROMs in the clinic setting has a wide range of benefits, both for patients and for the healthcare system. However, planning is required regarding how to implement PROMs optimally in the local routine care processes, preferably as an electronic version that is easily accessible for patients.
Conflicts of interest. ATHB has been involved in teaching activities for CSL Behring. HBB reports no conflicts of interest. KW reports grants from Shire, non-financial support from Moxie, during the conduct of the included study; personal fees from Novartis, personal fees from Moxie, personal fees from Shire/Takeda, personal fees from BioCryst and personal fees from CSL Behring, outside the submitted work. TC reports personal fees and other from BioCryst, personal fees, non-financial support and other from CSL-Behring, personal fees from Merck, personal fees and other from Novartis, personal fees from Octapharma, personal fees, non-financial support and other from Shire HGT, personal fees and other from Pharming NV, outside the submitted work. AB reports grants and other from CSL Behring, grants and other from Shire/Takeda, other from ViroPharma, from HAE Scandinavia, outside the submitted work.


 Click to show fullsize
Click to show fullsize