


1Dermatology Department, Hôpital Victor Dupouy, 69 rue du Lieutenant-Colonel Prud’hon, FR-95100 Argenteuil, 2Private Office, Saint-Germain-en-Laye, 3Private Office, Dijon, 4Private Office, Commercy, 5Private Office, Brest, 6Private Office, Paris, and 7Public Health Department, Ambroise Paré University Hospital, Assistance Publique-Hôpitaux de Paris, Boulogne-Billancourt, France. *E-mail: emmanuel.mahe@ch-argenteuil.fr
Accepted Apr 26, 2021; Epub ahead of print Apr 27, 2021
Acta Derm Venereol 2021; 101: adv00475.
doi: 10.2340/00015555-3813
Psoriasis is one of the most common chronic inflammatory skin diseases, the management of which has been revolutionized over the past decade by the development of biotherapies (1, 2) Symptoms occur in 20–30% of patients before the age of 18 years (3). When considered mild, psoriasis in children and adolescents may be managed with topical treatments. For moderate-to-severe psoriasis, guidelines are rare and poorly applied, and management is frequently delayed (4–6).
Therapeutic inertia is the failure to initiate or intensify treatment in a patient even when recommended (7, 8). Already evaluated in chronic diseases (e.g. diabetes, multiple sclerosis, hypertension), this phenomenon is rarely considered in dermatology (9, 10). The aim of this study was to investigate therapeutic inertia among dermatologists treating moderate-to-severe plaque psoriasis in adolescents.
This study was performed using a survey sent by e-mail to the 2,500 dermatologists who were members of the Fédération Française de Formation Continue et d’Evaluation en Dermatologie-Vénéréologie (FFFCEDV) (www.fffcedv.org). FFFCEDV is a French association dedicated to medical education with over 83 local associations. A 3-part survey was sent out in November 2019, followed by 2 weekly reminder emails. The first part of the survey investigated the demographics and clinical practice of physicians, their medical education regarding psoriasis over the past year, and the number of adolescents seen per trimester. Only practitioners treating adolescents with psoriasis could access the next part of the survey, exploring therapeutic inertia, which included questions about managing adolescents with uncontrolled moderate-to-severe plaque psoriasis despite local treatment and/or phototherapy. Three aspects were evaluated: patient and family parameters; drug and institutional variables; and physician-associated factors. For all analyses, quantitative data were expressed as means ± standard deviation, and qualitative data were expressed as numbers and percentages.
A total of 168 responses were received (females 73.8%; mean age 48.6 years), 38.7% worked in private practice, 29.2% in a hospital, and 30.4% in both. Of these, 132 (78.6%) regularly managed adolescents with psoriasis and completed the whole questionnaire (Table SI).
Most dermatologists consider having adequate information to evaluate the consequences of the disease (77.3%) and the efficacy and tolerance of treatments (59.1%). However, less than half report receiving sufficient information on guidelines (44.7%) and therapeutic optimization (36.4%) (Table SII).
Dermatologists also feel comfortable informing adolescents about their disease (86.4%) and treatments (74.2%), distinguishing adolescents’ and parents’ requests (68.2%), and starting new treatment if necessary (51.5%); including phototherapy (77.3%), acitretin (68.2%) and methotrexate (63.6%). However, less than half felt comfortable prescribing other treatments or optimizing treatment when needed (Tables SIII and SIV).
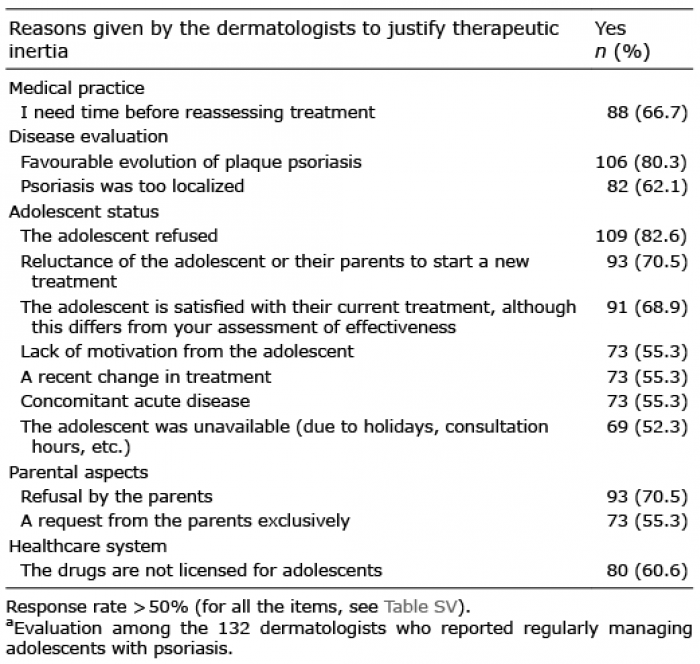
The dermatologists’ responses (positive response rate ≥ 50%) to the explanations for therapeutic inertia are detailed in Table I (all items in Table SV). Responses for elements that could reduce therapeutic inertia (positive response rate ≥ 50%) are seen in Table II.
Table I. Reasons given to justify therapeutic inertiaa
Table II. Responses for elements that could reduce therapeutic inertia
Therapeutic inertia is a complex phenomenon influencing the daily management of patients with chronic pathologies (7). This study evaluated therapeutic inertia in the management of adolescents with uncontrolled moderate-to-severe plaque psoriasis. The study found that the origin of therapeutic inertia in the management of these adolescents was multifactorial. In particular, the following elements that contributed to the development of therapeutic inertia were identified: disease evaluation by the practitioner, practice habits of the dermatologist, type of treatment in place, availability of medical training and specific information on the subject, healthcare system delays during usual practice, and concerns raised by the adolescent or their relatives regarding the therapeutic management adopted by the practitioner.
Scheen et al. (8) divided the sources of therapeutic inertia into 3 subcategories, of which the role of the clinician, the patient and the healthcare system accounted for 50%, 30% and 20%, respectively. Similar percentages were reported in our previous study of inertia in uncontrolled moderate-to-severe plaque psoriasis in adults (10). The physician appears to be the main actor contributing to this phenomenon among adults, since uncertainty and tendency to maintain the status quo may induce caution and hesitation when dealing with a patient afflicted by a chronic condition (9, 10).
The current study highlights the major impact of adolescents and their parents on therapeutic inertia. In over 70% of cases, the refusal or reluctance of the patient or their parent seems to have an impact on the practitioner’s therapeutic approach. Adolescence is a complex period, marked by disturbances in self-image, problems with therapeutic adherence and parental conflict, which may encourage patients to try to reduce therapeutic constraints. Two of our recent studies evaluating the comorbidities and clinical aspects of children with psoriasis in France reported a relative absence of adolescents with psoriasis in specialized consultations (11, 12). This could explain the major role of the adolescent and their family in delaying management.
Additional aspects associated with inertia have been identified, including the lack of marketing authorization that may block the initiation of effective and well-tolerated treatments (13). In addition, the presence of a limited affection was an obstacle to therapeutic adjustment. However, limited psoriasis of the nails, genitals or scalp can induce major physical and social handicaps impacting quality of life (14, 15).
Finally, a discrepancy in the responses of dermatologists was noted: while dermatologists clearly expressed their desire for additional training and guidance in the management of these patients, such elements were not considered factors in therapeutic inertia. However, it is possible that better information from doctors regarding possible treatments, their effects and side-effects could play a role in the unwillingness of parents and adolescents to change medication. In the same way, information given by patients’ associations could play this role.
The main limitation of this study was the low response rate despite national dissemination to dermatologists, a relatively short questionnaire, follow-up contact, guaranteed confidentiality and academic sponsorship. Several factors may account for this low response rate: (i) most dermatologists, especially those in private practice, rarely see patients with childhood psoriasis (12); (ii) the high frequency of surveys offered to dermatologists may have discouraged potential respondents. This potential bias may explain why rates of therapeutic inertia attributed to the physician and the healthcare system were lower in this study than reported previously. These initial results could serve as a pilot for larger international studies, as the question regarding treatment inertia in adolescence with psoriasis is “universal”.
Additional studies on therapeutic inertia in adolescents with psoriasis, as well as in the young population with chronic dermatological diseases, are necessary to allow strategies to be disseminated. Guidelines for the management of adolescent patients with moderate-to-severe psoriasis should include information supporting specific education and training, in order to minimize therapeutic inertia.
Conflicts of interest. FC is a consultant and has received speaker remuneration from Celgene and Novartis. CN, RM and BH are consultants for Celgene. EM is a consultant, has been an investigator, and has received speaker remuneration from Novartis, AbbVie, Janssen Cilag, Lilly, Leo Pharma, Celgene, and Amgen. The other authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize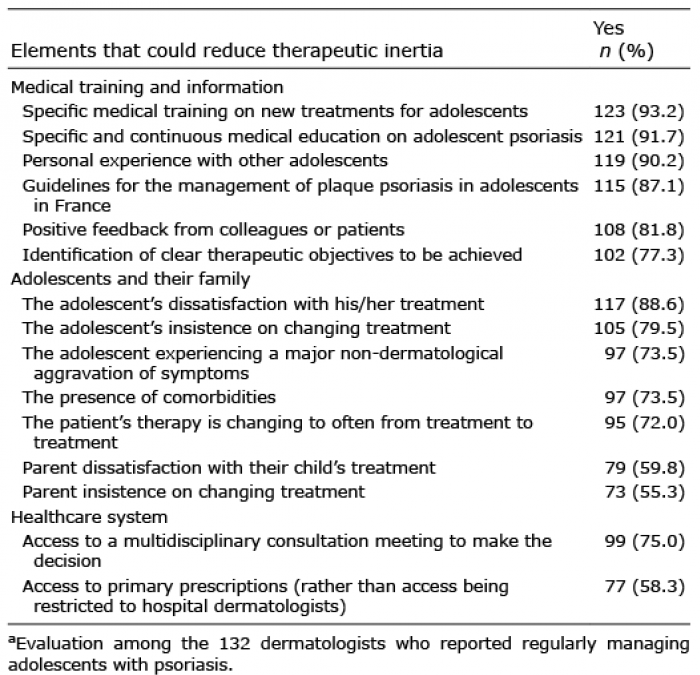 Click to show fullsize
Click to show fullsize