


1Department of Dermatology, Sheba Medical Center, Tel-Hashomer, Ramat-Gan, 2Electron Microscopy Unit, Department of Chemical Research Support, Weizmann Institute of Science, Rehovot, 3Azrieli Faculty of Medicine, Bar-Ilan University, Safed and 4Institute of Pathology, Sheba Medical Center, Tel-Hashomer, Ramat-Gan; 1,4Affiliated with the Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
#These authors contributed equally to the manuscript.
Frontal fibrosing alopecia is a cicatricial alopecia with rising incidence. Titanium nanoparticles were suggested as a potential environmental trigger, yet this is unproven. This study assessed hair morphology, chemical composition and nanoparticles in 20 patients and 40 healthy controls using scanning electron microscopy and energy-dispersive X-ray spectroscopy. Morphological evaluation revealed a significantly higher degree of cuticle weathering in patients compared with controls when there were no differences in hair care routine. There were no differences in the background elemental composition, while particle analysis revealed a significant increase in particles containing titanium, chlorine, silicon, magnesium, and iron in the patient group. Titanium-containing nanoparticles showed the most significant increase, being 8.6 times greater than in controls, without relation to age and disease duration. The results indicate that patients with frontal fibrosing alopecia should be advised to avoid aggressive topical cosmetic and medical hair treatments, and refrain from using cosmetic preparations containing titanium nanoparticles.
Key words: frontal fibrosing alopecia; hair shaft; nanoparticle; titanium.
Accepted Aug 13, 2021; Epub ahead of print Aug 16, 2021
Acta Derm Venereol 2021; 101: adv00541.
doi: 10.2340/00015555-3891
Corr: Anna Lyakhovitsky, Dermatology Department, Sheba Medical Center, Tel-Hashomer, Derech Sheba 2, Ramat Gan, 5262000, Israel. E-mail: anna.lyakhovitsky@sheba.health.gov.il
Frontal fibrosing alopecia is a hair disorder of unknown aetiology that is resistant to treatment and causes permanent baldness. Titanium nanoparticles in cosmetic products have been raised as a possible trigger, but their role is unproven. This study examined the structure and chemical content of hairs in patients with frontal fibrosing alopecia and compared these with normal hairs. It was found that hairs in frontal fibrosing alopecia are more weathered and contain more nanoparticles, especially titanium. Therefore we suggest that patients with frontal fibrosing alopecia should avoid, or at least reduce, aggressive hair care and topical treatments, as well as usage of cosmetic preparations containing titanium nanoparticles.
Frontal fibrosing alopecia (FFA) was first described in 1994 as a type of cicatricial alopecia occurring predominantly in postmenopausal women, most frequently involving the fronto-temporal hairline and eyebrows (1). A steep increase in the incidence of FFA has been observed the last 15 years (2, 3). Genetic, epigenetic, immune-mediated, hormonal, and environmental factors are implicated in the pathogenesis of FFA (2, 4). Potential environmental triggers include sun exposure, topical allergens, foods, toxins, and trauma (2, 3, 5). It has been proposed that exogenous agents penetrating the hair follicle, functioning as a reservoir, may trigger an immunological response (2). Furthermore, decreased sebum flow during menopause causes slower elimination and increases the risk of inflammation or toxicity; this may be the cause of increased incidence of FFA in older females (6). Aldoori et al. were the first to describe a higher incidence in the use of sunscreens by patients with FFA and raised a possible link, followed by a number of epidemiological studies showing similar findings (5–8). Several hypotheses regarding the pathogenesis, including T-cell mediated allergic reactions, suppression of the anti-inflammatory effect of sunlight, endocrine effects, and oxidative damage were proposed (5–11). Since the 1990s, when nanoparticles (NPs), particularly titanium dioxide (TiO2), as ultraviolet (UV) filters were added to sunscreens and facial skin care products, speculations have surfaced on their potential role (7). Brunet-Possenti, et al. (12) first described the presence of TiO2 NPs in hair shaft in patient with FFA. Notably, most particles mentioned were > 500 nm, rendering them micro-particles rather than NPs. A recent pilot study demonstrated the presence of TiO2 particles not only in 16 patients with FFA, but also in 3 out of 4 controls (13). Current data cannot link all aspects of FFA, including involvement of the posterior scalp, disease in unexposed persons, and the low incidence in the population using sunscreens, to sunscreens, and provide unequivocal evidence of their causative role (3, 7, 14–22). Since hair loss may occur due to alterations in hair structure or chemical composition, their evaluation is essential. Alterations in the chemical composition of hair may lower its resistance to external factors and has been described in different metabolic disorders, cancers and other pathologies (23–27).
The aim of the current study was to analyse and compare hair shaft morphology, elemental composition, and NPs in patients with FFA and controls, using scanning electron microscopy (SEM) and energy-dispersive X-ray spectroscopy (EDX).
Study population
A single-centre case-control study was conducted. Subjects with FFA were recruited from patients visiting the outpatient dermatology clinic at Sheba Medical Center, Israel, between January 2019 and December 2019, who agreed to participate. Inclusion criteria were: age ≥ 18 years, and diagnosis of FFA made by a dermatologist experienced in hair diseases. Diagnosis was based on clinical examination and confirmed on biopsy in most cases. Control group participants were selected from patients who visited the dermatology clinic for other reasons, or hospital staff, and were paired with each case in the patient group, with a 2:1 control-to-case ratio, according to sex and age (±5 years). Patients with known hair or scalp disorders were excluded. Participants’ use of leave-on and wash-off facial and hair cosmetic products, sunscreens and hair treatments was reviewed for 5 years prior to participation, including frequency of use and particular agents used. Frequency of use of facial and hair cosmetics was categorized into: < twice weekly, ≥ twice weekly. Sunscreen use was categorized into: no use, as needed (before sun exposure), ≥ twice weekly during summer, ≥ twice weekly all year. Hair treatments evaluated included: heated hair styling (no, ≤ twice weekly, > twice weekly); dyeing (no, < once monthly, ≥ once monthly); traction hair practices (no, yes); perming or straightening (no, ≤ once a year, > once a year). The study was carried out according to the Declaration of Helsinki and was approved by the Review Board of Sheba Medical Center (SMC 5086-18). Informed consent was obtained from all participants.
Hair sampling
Two to 4 terminal hairs were plucked from the anterior hairline from all participants after the area was cleaned with alcohol. In addition, hair samples were taken from uninvolved scalp area (vertex or occiput) from 7 patients with FFA and 3 controls. The samples were stored in a paper envelope. Washing procedures were not performed prior to sample preparation, in order to preserve any contaminants.
Sample preparation
From the hairs plucked from each subject, the less traumatized samples were chosen for evaluation, using trichoscopy. The samples were mounted on a glass slide with a cover slip for evaluation by light microscopy. In preparation for evaluation by SEM, the proximal fragment of the hair sample (measuring 15 mm) was cut to enable analysis at a point 5–10 mm from the proximal end. Samples were attached to aluminium stubs using double-sided carbon sticky tape (“SPI” adhesive carbon tape 05072-AB; SPI supplies, West Chester, PA, USA). The mounted samples were coated with a 15-nm thick carbon layer in a carbon coater (CCU-010, Safematic GMBH, Switzerland) using a planetarium stage tilted to 40° for high-resolution imaging and reducing the charging effect on non-conductive organic samples.
Sample imaging and data analysis
Full-length hair samples were analysed using trichoscopy and high-power field light microscopy. SEM evaluation was performed using Carl Zeiss Sigma and Ultra SEM (Carl Zeiss Microscopy, Oberkochen, Germany). Three random sites on each sample, 0.25–1 mm apart, were scanned to ensure uniform changes. Secondary electron (SE) detector imaging was performed for hair shaft evaluation. Digital photomicrographs were taken at magnifications of ×77, ×500, ×1,000, ×2,500, and ×5,000. Three measurements of hair shaft width were obtained from each sample. The mean value was used for statistical analysis.
The assessment of hair shaft morphology comprised evaluation of the cuticle edge and surface characteristics (graded 0–2) and hair shaft damage (graded 0–4) (28). The cuticle edge characteristics were as follows: (i) scale border definition (0, uniformly well-defined border; 1, some areas of reduced definition; 2, ill-defined border), (ii) regularity of scale orientation (0, uniformly regular; 1, some areas of irregularity; 2, mostly irregular), (iii) jagging (0, no jagging; 1, mild/≤ 5 jagged scales per sample; 2, moderate to severe/ ≥ 5 jagged scales per sample), (iv) lifting (0, no lifting; 1, mild; 2, moderate to severe), and (v) broken fragments (0, none; 1, few/≤ 2 fragments per sample; 2, many/≥ 3 fragments). The cuticle surface characteristics were as follows: (i) scaling (0, none; 1, mild/localized; 2, severe/diffuse), (ii) grooves (0, none; 1, single; 2, ≥ 2), (iii) fissures (0, none; 1, few/≤ 2; 2, many/≥ 3), and (iv) holes (0, none; 1, few/≤ 2; 2, many/≥ 3). Hair shaft damage was graded from 0 to 4 as follows: 0, intact cuticle with regular overlay; 1, irregular overlay without cracks or holes; 2, severe lift up with cracks or holes without cortex exposure; 3, foci of partial cortex exposure; and 4, foci of disappearance of cortex.
A blind evaluation of morphological characteristics was performed by 2 dermatologists. In case of score differences, samples were re-examined by a third dermatologist.
A high-resolution angular selective backscattered electron detector (HAsB; Carl Zeiss Microscopy) was used for identifying inorganic particles. For the elemental analysis, an EDX (Bruker QUANTAX EDS Xflash® 6 detector with a 60 mm2 probe (Bruker Nano Analytics, Berlin, Germany) was used. A diagram of the elemental distribution according to the energy peaks was obtained. The element amount was measured in atomic percentage (resolution ±0.5 atomic percent). The mean of 3 measurements was used for statistical analysis.
Carbon analysis was not included in the results as the samples were prepared using carbon coating. Hydrogen analysis was also excluded because its measurement is not feasible using EDX. For particle analysis, Bruker EDS ESPRIT Feature and Particle Analysis module were used. The number of particles per 2,171 m2 surface, their size (in nm), and composition were measured for each site. The mean of 3 measurements was used for statistical analysis.
Statistical analysis
A total of 20 cases and 40 controls were recruited to enable identifying a difference of 1 ± 1 in Ti NPs and assuming normal distribution, with 95% confidence and 94.8% power. For quantitative variables normal distribution was tested using Shapiro–Wilk test. Quantitative variables with normal distribution are expressed as mean ± standard deviation (SD). Non-normally distributed variables are expressed as median [25th–75th percentile]. Categorical variables are expressed as numbers and percentages (%). An independent Student’s t-test was used for normally distributed variables and the Mann–Whitney test for non-normally distributed variables to compare continuous measurements between patients and controls. Fisher’s exact test and the χ2 test were used to compare categorical variables between the groups. All statistical tests were 2-sided, and a p-value < 0.05 was considered statistically significant. Logistic regression model adjusted to age with a forward selection method was applied to identify the variables that most significantly discriminated between FFA and controls. Analysis of variance (ANOVA) was used to identify factors related to the number of NPs containing titanium (Ti). SPSS software was used for all statistical analyses (IBM SPSS, version 27, Armonk, NY, USA).
Demographic data
Out of 38 patients who met the inclusion criteria, 18 declined to participate. The main reason was reluctance to undergo hair pulling. Twenty patients with FFA were included. Mean age was 62.7 ± 11.2 years (range 42–86 years). The control group consisted of 40 subjects, with a mean age of 64.2 ± 9.1 years (range 46–78 years). The difference in age between the groups was statistically insignificant (p = 0.581). All patients and controls were women. The mean duration of disease in the patients’ group was 6 ± 3.5 years (range 2–15 years). Evaluation of use of facial and hair cosmetics showed tendency for more frequent use of facial leave-on products and sunscreens in patients with FFA, but the differences were not statistically significant. There was also no significant difference in the frequency of hair treatments (Table SI). Most participants reported the use of multiple cosmetic products, with only some being able to name brands, and fewer reporting the name of a specific product. Therefore, it was impossible to categorize facial and hair products by brand name and ingredients.
Hair shaft morphology evaluation using trichoscopy and light microscopy
There were no differences between patients and controls. Hair shafts in both groups appeared normal; had a cylindrical shape, regular contour, and uniform pigmentation.
Hair shaft morphology evaluation using scanning electron microscopy
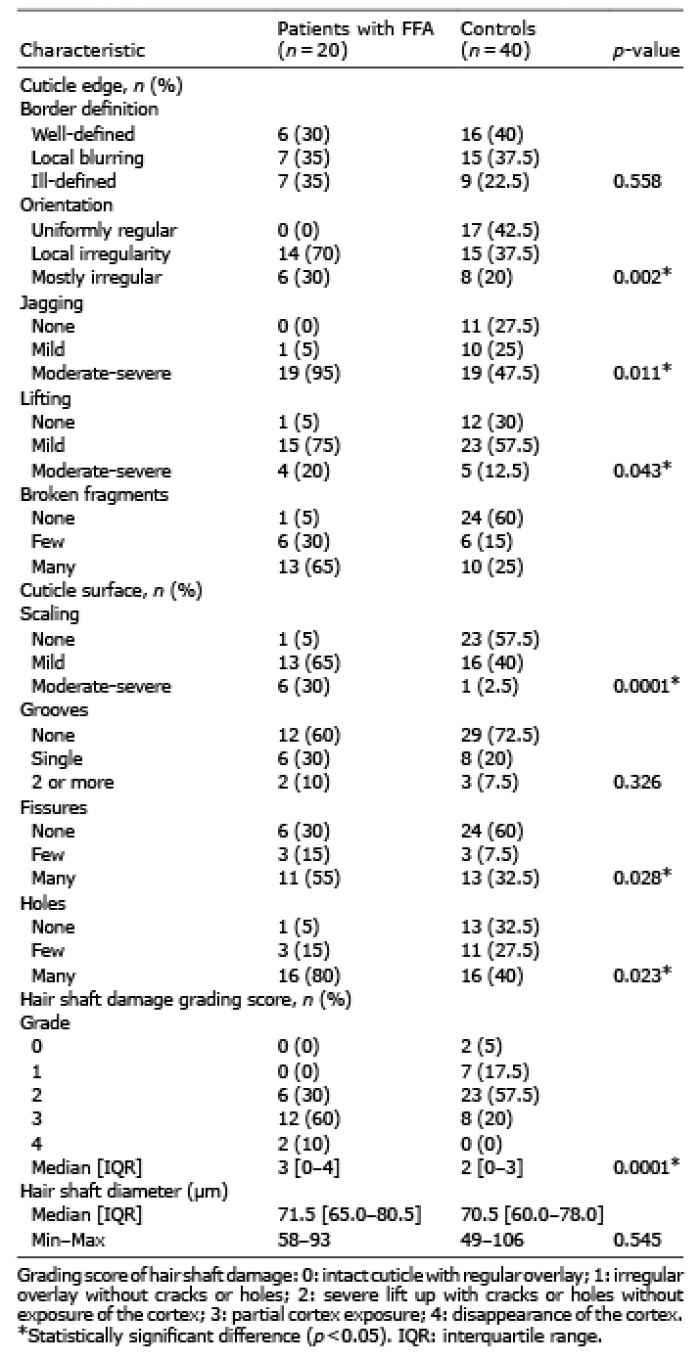
Table I shows the results of the morphological assessment. There were no significant differences in the hair shaft diameter between groups. Hair surface changes were non-specific and matched the alterations linked to weathering, with no unique characteristics of FFA (Fig. S1). However, differences were observed in the prevalence and severity of these changes, most of which were more pronounced in patients with FFA.
Table I. Hair shaft surface morphology in patients with frontal fibrosing alopecia (FFA) and controls, based on scanning electron microscopy
Background elemental composition of hair shafts by energy-dispersive X-ray spectroscopy
EDX analysis did not reveal significant differences between groups. Elements evaluated and compared included oxygen, sulphur, nitrogen, chlorine, calcium, sodium, potassium, and copper. Carbon, hydrogen, silicon, magnesium, manganese, chromium, and zinc were also identified, but their data could not be compared. Carbon analysis was not included in the results as the samples were prepared using carbon coating. Hydrogen analysis was excluded because its measurement is not feasible using EDX. Other elements were not compared because their concentration was below resolution analysis.
Particle analysis using energy-dispersive X-ray spectroscopy
Data on the number and contents of particles are shown in Table II. NPs were observed in both patients and controls. No elements unique to patients or controls were observed. Although a higher number of NPs were found in patients compared with controls, the difference was insignificant (p = 0.103). The particles contained various elements, including chlorine, calcium, Ti, sodium, silicon, potassium, magnesium, iron, aluminium, and copper. The number of particles containing Ti, chlorine, silicon, magnesium, and iron was significantly higher in patients with FFA. The most significant differences were observed for Ti (p = 0.00005), followed by silicon (p = 0.003), and magnesium (p = 0.003). Ti NPs were detected in hair shafts from the anterior scalp in 100% of patients with FFA and 80% of controls, and their median number was 8.6 times higher in patients with FFA. In some particles Ti was combined with calcium, aluminium, chloride, iron, sodium, or silicon (Figs 1 and 2). There was no significant correlation between the number of Ti NPs and age in all study participants (p = 0.352), and between the patient and control groups when examined separately (p = 0.136 and p = 0.663, respectively). In addition, there was no significant correlation between the number of Ti NPS and disease duration in patients with FFA (p = 0.531). Particle diameter analysis revealed aggregates of various sizes ranging from 47 to 569 nm (Table SII). In 7 patients with FFA in whom both involved and uninvolved areas were evaluated, analysis of hair shaft from uninvolved areas revealed significantly lower content or absence of Ti NPs compared with involved areas (mean 0.09 ± 0.15 and 8.11 ± 4.82, respectively, p = 0.01). In 3 controls in which samples from anterior and posterior scalp were evaluated, no or single Ti NPs were observed, and due to low numbers no statistical comparison was made.
Table II. Number of particles per area in patients with frontal fibrosing alopecia (FFA) and controls obtained using energy-dispersive X-ray spectroscopy
Fig. 1. (a) An example of a hair shaft image of a patient with frontal fibrosing alopecia (FFA) taken using a backscattered electron detector on a scanning electron microscope (SEM) for detecting nanoparticles (NPs) on the surface of the hair shaft (original magnification ×10,000). (b) The magnified area is marked by a white square in (a) (original magnification ×30,000); violet arrows indicate titanium NPs; red arrowheads indicate iron NPs. (c) Visualization of NPs using the Bruker EDS ESPRIT Feature analysis: violet=titanium-containing NPs, red=iron-containing NPs; (d and e) examples of the energy-dispersive X-ray spectroscopy diagram obtained from the titanium and iron NPs analysis, respectively.
Fig. 2. Hair shaft image of a patient with frontal fibrosing alopecia (FFA) taken by a scanning electron microscope (SEM) for the visualization of nanoparticles (NPs). (a) Secondary electron (SE) detector presents an image of surface. (b) HDAsB (angle selective backscattered electron) detector allows the recognition of NPs. EDS detector reveals NPs composition. Light-violet arrows: single titanium-containing NP; dark-violet arrows: a conglomerate of smaller titanium-containing NPs; red arrowheads: iron-containing NPs. Original magnification ×50,000.
Although the data from the current study revealed a trend towards larger diameters for several elements in FFA, only calcium-containing particles revealed a significant difference (p = 0.027).
An ANOVA model was applied to identify whether FFA was associated with increased number of Ti NPs, with adjusting to all statistically significant morphological variables from previous analysis. This analysis demonstrated significantly higher mean number of Ti NPs, when comparing FFA with controls (19.5 ± 4.56 vs 5.4 ± 2.48, respectively, p = 0.003), while no significant effect was demonstrated for each morphological variable separately.
Logistic regression for the evaluation of differences between patients with FFA and controls
To identify the most significant variables that allowed discrimination between patients with FFA and controls, a logistic regression model using the forward selection method was applied. It included age, hair shaft grading damage and variables of particle analysis. The most significant variable in the model was number of Ti NPs with odds ratio (OR) 1.16 (95% confidence interval (95% CI) 1.06–1.27, p = 0.002). Age and grading of hair shaft damage were not statistically significant (OR 0.951; 95% CI 0.88–1.03 and OR 3.01; 95% CI 0.74–12.19, respectively). Nagelkerke R2 0.45.
This study found that hair of patients with FFA was prone to weathering and showed an increased number of NPs containing Ti, silicon, magnesium, chlorine, and iron, with Ti showing the most significant increase. This further supports the association between Ti and FFA pathogenesis.
Trichoscopy and light microscopy are readily available tools for diagnosis of hair disorders. However, several conditions display subtle changes that are not recognizable using these modalities. In such cases, SEM is the preferred high-resolution diagnostic tool (28–30). In this study, while trichoscopy and light microscopy showed no morphological changes, SEM revealed a higher incidence and degree of non-specific cuticle alterations in the patients with FFA. Such alterations can be due to a genetic predisposition to hair weathering or various exogenous factors, namely, mechanical (damaging hair practices), chemical (toxins, medications), or physical (UV radiation). Previous studies have investigated the correlation between FFA, hair care products, and hair care practices; however, no such correlation was found (5, 6). In fact, the frequency of hair dyeing, shampooing, and traction hairstyling has been reported to be lower in patients with FFA than in healthy controls, possibly due to patients being concerned about the harmful effects of these practices, as well as physician guidance (6, 31). In the current study no significant differences were found between the frequency of use of cosmetic products and hair treatments between the patients with FFA and controls.
The question arises as to whether cuticle damage in FFA could be a consequence of topical medical treatments. To date, there are no reports linking hair damage to topical medications. Furthermore, several studies have described improvement in hair shaft disorders under treatment with topical minoxidil (32, 33). However, the possibility that aggressive application of topical agents can cause mechanical or chemical damage cannot be excluded. Therefore, the current findings raise the possibility that hairs in patients with FFA are more susceptible to mechanical damage. Thus, we suggest that patients with FFA should be advised to avoid or at least reduce aggressive cosmetic treatments and rigorous application of topical medications.
There were no significant differences in background elemental composition of hair shafts and in the types of elements that made up NPs between groups. In concordance with previous study, Ti NPs were found in both patients and controls (13). Although the total number of NPs in patients with FFA was higher, the difference was statistically insignificant. Therefore, it cannot be concluded that hairs in patients with FFA are more permeable to NPs. However, several NP elements, especially Ti, were significantly more common in patients with FFA. Ti NPs were detected in 100% of patients with FFA and 80% of controls, and their number was 8.6 times higher in FFA. The lack of a relationship between the disease duration and the number of Ti NPs shown is more supportive of their causative role rather than being a consequence of the disease. Ti NPs are used extensively in cosmeceuticals, such as moisturizers and sunscreens, foods, and pharmaceutical products. Exposure to Ti NP containing products is high and can occur through ingestion, inhalation, dermal or follicular penetration during occupational contact or personal use (34, 35). Cosmeceuticals and sunscreens represent a potential source of dermal and follicular exposure (34, 35). Previous studies have shown that patients with FFA use facial moisturizers and sunscreens more frequently than the control group (5–11). This was also the trend in the current study, which leads to the hypothesis that follicular exposure is the main route. Given that there were considerably higher amounts of Ti NPs found in hairs from the frontal scalp vs the vertex and occipital scalp, a link to facial products rather than hair products can be speculated. Since exposure to Ti NPs is high in both affected and non-affected persons, the possibility of a higher sensitivity to Ti NPs in patients with FFA still needs to be explored.
The ability of TiO2 NPs to elicit an inflammatory response, either by contact sensitization or by enhancing the penetration of other substances, such as gold, was previously stated as a concern (7, 8, 13, 36). Furthermore, under UV radiation, TiO2 NPs were found to generate free radicals and promote oxidative stress with DNA damage response. TiO2NPs have also been described to cause pulmonary inflammation and fibrosis in mice (37). Further studies evaluating Ti NPs in other hair diseases, as well as the effect of avoiding of contact with Ti-containing preparations in patients with FFA are needed to expand our knowledge. Nevertheless, the current findings suggest that, at this point, a recommendation for patients with FFA to refrain from using cosmetic preparations containing Ti NPs is reasonable.
In addition to Ti, the current study revealed a significantly large number of particles containing silicon, chlorine, magnesium, and iron in FFA. These elements have not been previously reported in association with FFA, and further studies are needed to validate these findings. Silicon-containing NPs are found in cosmetics, medicines, and foods. They have been described as having an anti-inflammatory or pro-inflammatory effect related to their size and charge (38). Interestingly, iron-containing NPs were recently shown to have hair-growth-promoting effects and were proposed as drug delivery systems for topical treatments of alopecia (39, 40). To our knowledge, no study has demonstrated a link between NPs containing magnesium or chlorine, and hair disorders. Notably, this study did not demonstrate the presence of zinc oxide NPs, which were raised as a potential trigger for FFA related to sunscreens. Regarding particle size, calcium-containing particles were found to be larger in patients with FFA. The significance of this is unclear and should be further investigated.
This study has a number of limitations. One limitation was the small study group. Furthermore, this study evaluated the presence of Ti NPs in the hair shaft after its emergence from the follicular ostia, which does not prove their entrance to the follicle. A further limitation was the inclusion of prevalent (previously treated) patients along with new cases. This raises the question of the effect of topical medications on the cuticle in treated cases of FFA, which was discussed. Another limitation was the exclusive use of SEM-based methods. SEM was chosen because it is a powerful technique, which does not cause hair destruction and allows detailed visualization of the morphology along with analysis of background elemental composition and particles. In order to avoid selection bias, all controls in the study were selected randomly from the same population that produced the cases, using several sources, and were paired with cases in the patient group according to age and sex.
In conclusion, it was demonstrated that the hair of patients with FFA showed more signs of weathering and contained more Ti NPs. These findings denote that the hair of patients with FFA may be prone to mechanical damage and support the previously suggested role of Ti in pathogenesis of FFA. The results of the current study indicate that patients with FFA should be advised to avoid aggressive topical cosmetic or medical hair treatments, and refrain from using preparations containing Ti NPs.
Larger studies using a combination of evaluation methods, such as transmission electron microscopy combined with SEM, inductively coupled plasma mass spectrometry, and EDX, that will provide more comprehensive data on hair morphology and location of NPs in the hair follicle, will extend our knowledge on the pathogenesis and aid the management of this challenging condition.
The authors thank Professor Ronen Alon from the Weizmann Institute of Science for his valuable assistance, constructive advice, and encouragement during the planning and conduct of this research, and the team of Moscowitz Center for Nano and Bio-Nano Imaging at the Weitzmann Institute of Science for technical support. We thank Jakob Rimer, MSc, PhD, Zvi Segal, MD, and Ido Tzanani, MD, MPH, for their insightful contribution to the statistical analysis of the results. We also thank all the participants in this study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize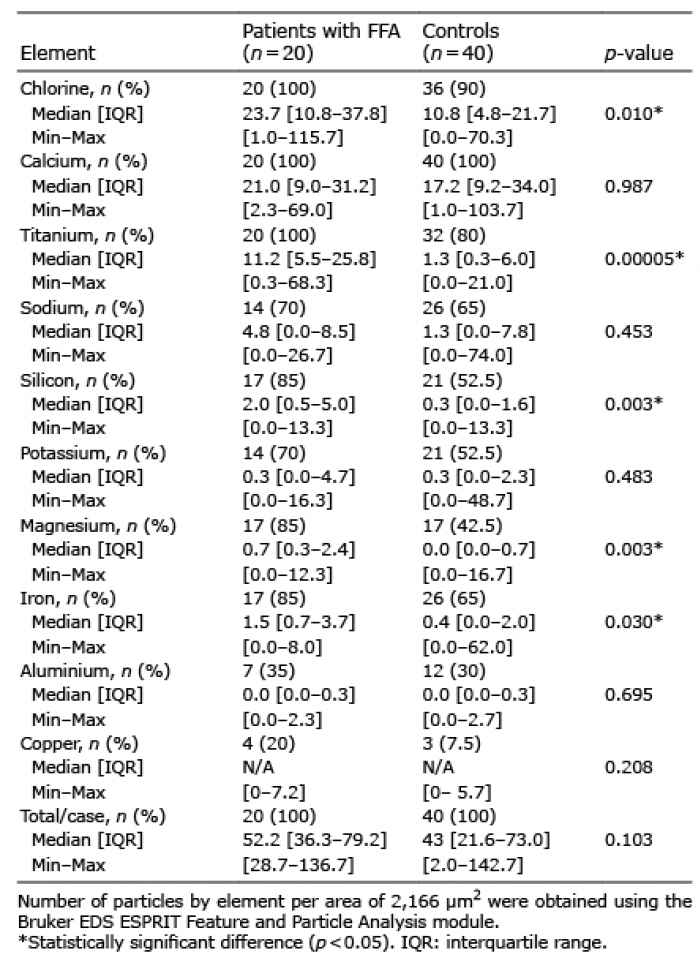 Click to show fullsize
Click to show fullsize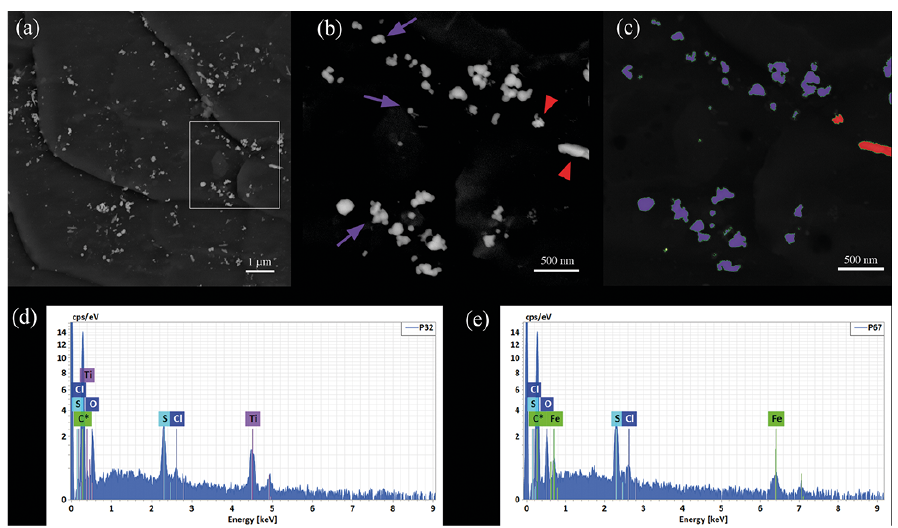 Click to show fullsize
Click to show fullsize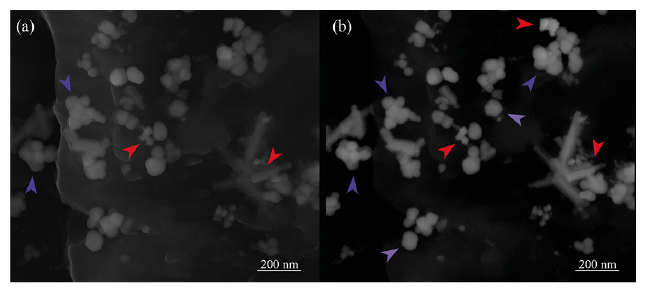 Click to show fullsize
Click to show fullsize