


1Department of Dermatology and Venereology, University of Copenhagen, Bispebjerg Hospital, Copenhagen, Denmark, 2LEO Pharma AB, Malmö, Sweden, 3Incentive, Holte and 4Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark
To estimate the cost of illness in adult patients with moderate-to-severe atopic dermatitis (AD) a cohort study was conducted identifying Danish citizens (≥ 18 years) diagnosed with AD between 1997 and 2018 in the Danish National Patient Register. Moderate-to- severe AD was defined as ≥ 3 hospital contacts regarding AD the first year after diagnosis. Each patient with AD was matched to 3 reference individuals through the Central Person Registry. Societal costs included the direct costs for primary-sector visits, inpatient hospitalizations, outpatient contacts, prescription medicine and indirect costs of lost productivity 3 years before and 5 years after the index date (the study period). A total of 5,245 patients with moderate-to-severe AD were identified. The mean attributable healthcare costs for patients with moderate-to-severe AD were EUR 10,835 (p < 0.0001) during the study period. Moderate-to-severe AD among adults inferred substantial economic burden compared with a group of matched reference individuals.
Key words: atopic dermatitis; burden of disease; cost of illness; real-world evidence; register-based cohort study.
Accepted Aug 25, 2021; Epub ahead of print Aug 26, 2021
Acta Derm Venereol 2021; 101: adv00538.
doi: 10.2340/00015555-3908
Corr: Andreas W. Brenneche, LEO Pharma AB, Hyllie Stationsväg 42, SE-201 24 Malmö. E-mail: awbse@leo-pharma.com
Atopic dermatitis is a chronic inflammatory skin disease resulting in dry, itchy skin. This register-based study showed that having moderate-to-severe atopic dermatitis as an adult was associated with substantial economic burden, with lower income and reduced lifetime earnings on an individual level, and higher societal costs on the overall level, such as higher healthcare utilization, paid sick leave, disability insurance, etc., compared with individuals who do not have atopic dermatitis. The study indicates an unmet need for better management and treatment of patients with moderate-to-severe atopic dermatitis.
Atopic dermatitis (AD) is a chronic, inflammatory skin disease characterized by dry, eczematous, and itchy skin in typical anatomical locations, and commonly co-existing with allergic disease. AD is associated with a high burden of disease, negatively affecting quality of life and associated with depressive and anxiety symptoms (1, 2). A recent systematic review has shown a range of 1-year prevalence estimates between 1.2% and 17.1% among adults. Thus, AD is a common chronic skin disease (3–5).
Patients with moderate-to-severe AD use a large amount of prescription medicine, which adds to the disease-related costs. In addition, AD is associated with a substantial economic burden, largely in the form of indirect costs (1, 6–13). A Danish register-based cohort study (7) found that younger patients with severe AD, in particular, were more likely to receive social benefits, i.e. paid sick leave (odds ratio (OR) 1.37, 95% confidence interval (95% CI) 1.25–1.52), compared with reference individuals. A recent systematic literature review found a high socioeconomic impact of AD and an unmet need from a patient perspective (14). New treatments have been introduced recently, and more novel, innovative, and improved treatments for moderate-to-severe AD are expected. To evaluate the cost-effectiveness of these new treatments, it is important for decision-makers to establish the economic burden of patients with moderate-to-severe AD. Current knowledge about healthcare costs and utilization among patients with AD in Denmark is scarce. The objective of this register-based cohort study was to estimate healthcare costs and utilization among Danish patients with moderate-to-severe AD.
A retrospective population-based cohort study was performed including adult (≥ 18 years) Danish citizens with moderate-to-severe AD, using the Danish national healthcare registers in the period 1997 to 2018.
Data sources
At birth or migration all Danish residents are assigned a unique 10-digit personal identification number, recorded in the Central Person Register (CPR) (15). For all individuals, the CPR registers date of birth, sex, vital status, and family relationships, and enables an identity-secure linkage of information between the Danish national registers. Patient-specific data were collected from the Danish National Patient Register (DNPR) (16), which holds information on all somatic hospitalizations to Danish hospitals since 1977. Outpatient activities, emergency room contacts, and activities in psychiatric wards are included in DNPR (16). All diagnoses in DNPR are recorded according to the 10th Revision of the International Classification of Diseases (ICD-10). Costs for all healthcare services are registered as Diagnosis Related Group (DRG) tariffs. Use of systemic drugs and biologics dispensed at Danish hospitals are recorded in DNPR as treatment procedure codes. Contacts and costs in primary care are recorded in the National Health Service Register (17). Data on all prescription medicine dispensed at Danish pharmacies are recorded in the Danish National Prescription Register (18). Data on income are recorded in the Income Statistics Register (19). The DREAM Database includes information on all public transfer payments administered by Danish ministries and municipalities; the database comprises data for all Danish residents (20).
Study population
Adult patients were defined as age ≥ 18 years at the first AD-related hospital contact, i.e. a hospital contact where AD was the primary diagnosis (ICD-10 diagnosis code: L20 including sub-levels). To ensure that patients were correctly diagnosed and reflects the anticipated treatment pattern in the Danish healthcare system, the patient population was limited to: (i) patients who appeared in the CPR at the time of diagnosis; (ii) patients who had received an AD diagnosis as a primary diagnosis at a dermatology department within 1 year after the patient’s first AD-related hospital contact; (iii) patients who had their first hospital contact regarding AD in year 1997 or later; (iv) patients who had at least 3 hospital contacts for AD-related treatment in the first year after the index date; and (v) patients who had at least one contact with a primary care dermatologist within the study period (any diagnosis). The 5 inclusion criteria ensured that patients had presumed moderate-to-severe AD.
For each patient with AD, 3 reference individuals with no history of AD in the DNPR were randomly selected from the CPR. Patients (i.e. patients with moderate-to-severe AD) and reference individuals were matched by sex, year of birth, and region of residence in the index year. The index year was defined as the year of the patient’s first AD-related hospital (inpatient or outpatient) contact.
Endpoints
In estimating the healthcare costs of patients with moderate-to-severe AD, market prices (for prescription medicine, according to the Register of Medicinal Product Statistics), fees (for general practitioners and specialists, according to the National Health Insurance Service Register), and tariffs for hospital contacts (DRG tariffs for admissions and outpatient visits, according to the DNPR) were applied.
Productivity was proxied by earnings, as shown in the Danish Income Register (Appendix S1), allowing for an estimation of the cost of lost productivity. The mean number of weeks that patients and reference individuals received social benefits and paid sick leave was estimated from data in the Danish DREAM database. Healthcare utilization was estimated as the mean number of inpatient hospitalization and outpatient contacts per year, as well as the mean number of visits to a primary care dermatologist.
Data analysis
The study followed participants for 3 years prior to the index date, i.e. the date of first AD hospital contact (at the earliest, 1 January 1997), and up to 5 years after the index date, the date of death, emigration, or the end of follow-up (31 December 2018), whichever occurred first. For all analyses, the outcomes of patients with moderate-to-severe AD were compared with the outcomes of matched reference individuals in the study period. The societal costs of AD were estimated on an individual level as both actual costs and attributable costs. Actual costs were estimated as the patients’ and reference individuals’ mean costs in year t relative to the index date. Attributable costs were estimated as patients’ actual costs in year t minus the reference individuals’ actual costs in the same year. A t-test was applied to examine whether the actual costs were significantly different between patients and reference individuals. General linear hypothesis testing was applied to test for significant differences in total healthcare costs and earnings across the full study period (21). To test the robustness of the results, a sensitivity analysis was performed, changing the definition of patients with moderate-to-severe AD to have at least 2 (instead of 3) hospital contacts in the first year after the index date.
Patients with 3 or more AD contacts per year in the first 4 years after the index date (year 0 to year 3) were identified as a sub-group, and the mean individual healthcare costs during the study period were estimated.
In the case of AD, it is thought unlikely that the index date, here defined as the patient’s first AD-related hospital contact, reflects the true onset of the disease. This would invalidate the difference-in-difference approach (Appendix S1) to estimating the cost attributable to AD, since patients are probably affected by the disease prior to the index date. For that reason, the difference-in-actual-costs approach was used to estimate the costs attributable to AD.
Data management and statistical analyses were carried out using SAS statistical software (9.4, SAS Institute, Inc., Cary, NC, USA).
Ethical considerations
The study was register-based and complied with the regulations set up by the Danish Data Protection Agency (J. nr. 2014-54-0664). No ethical approval was needed.
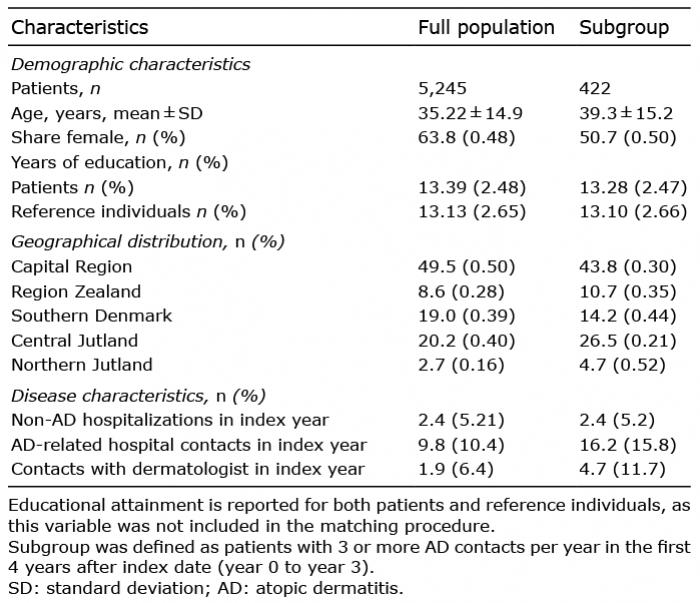
A total of 18,866 persons were identified in DNPR between 1997 and 2018 with a primary diagnosis code of AD, registered at a dermatology department. Among these, 7,167 patients were excluded because they had fewer than 3 AD-related hospital contacts in the year following the index date, and 1,633 patients were excluded because they had no contact with a primary care dermatologist during the study period. A total of 4,821 patients were excluded because they had their first AD-related hospital contact before the age of 18 years. In total, the study population comprised 5,245 patients with presumed moderate-to-severe AD (Fig. S1). Among the study population, 63.8% were female and the mean ± standard deviation (SD) age at the index date was 35.2 ± 14.9 years (Table I).
Table I. Characteristics of the patients in the study population, including geographical distribution and disease characteristics of the patients included in the study population in the index year
Healthcare costs
The individual mean yearly healthcare costs were significantly higher throughout the study period among patients with moderate-to-severe AD compared with their matched reference individuals (Table SI). The mean ± SD individual healthcare costs for each of the 3 years preceding the index date were EUR 1,870 ± 4,304, EUR 1,986 ± 4,606, and EUR 2,491 ± 5,713, respectively. On average, this is EUR 625 higher (p < 0.0001) than the costs in the group of matched reference individuals (Table SI).
The difference in healthcare costs were largest in the first year following the index date, with an estimated individual mean ±SD healthcare cost of EUR 4,930 ± 6,813) for patients with AD and EUR 1,572 ± 3,078) for the matched reference individuals (p < 0.0001). In the years following (years 1–5), the healthcare costs for patients decreased, but remained higher than the costs during the years leading up to patients’ first AD-related hospital contact. The difference in mean healthcare costs between patients and reference individuals almost doubled in the years following the index year (years 1–5), to EUR 1,120 (p < 0.0001), compared with the 3 years prior to the index date. In total, the attributable healthcare costs for patients with moderate-to-severe AD were estimated to be EUR 10,835 (p < 0.0001) during the study period (Fig. 1).
Fig. 1. Mean healthcare costs in the sample of patients with moderate-to-severe atopic dermatitis (AD) and in the matched sample of reference individuals in each year relative to the index date, in Euro (EUR).
Cost of prescription medicine
Patients with moderate-to-severe AD had a higher utilization of prescription medicines throughout the study period (Table SII). The individual mean annual cost of prescription medicines for patients with moderate-to-severe AD was EUR 169 (p < 0.0001) (95.5%) higher than for people in the reference group, corresponding to estimated attributable costs of prescription medicine of EUR 1,521 (p < 0.0001) for patients with moderate-to-severe AD during the study period. The difference in costs associated with use of antibiotics for topical use, corticosteroids and other dermatological preparations accounted for 35% of the difference.
Healthcare utilization
Patients with moderate-to-severe AD had a higher number of both non-AD-related hospital contacts and outpatient contacts in the 3 years prior to their first AD-related hospital contact. On average, patients had 0.1 more inpatient hospitalizations (p < 0.0001) and 0.66 more outpatient contacts (p < 0.0001) compared with reference individuals (Table SIII). During this period, 32.2% of the patients’ inpatient hospitalizations were within the medical specialty of orthopaedic surgery and 16.3% of outpatient contacts were within the medical specialty of dermato-venereology, which constituted the 2 most frequently registered medical specialties. The difference in healthcare utilization amounted to an increased cost of EUR 1,166 (p < 0.001) during the 3 years prior to the index date, corresponding to 62% of the difference in total healthcare costs between patients and reference individuals in this period (Table SIV). The number of non-AD-related inpatient hospitalizations and outpatient contacts remained stable and significantly higher for patients during the entire study period.
By definition, neither the patients nor the reference individuals had any AD-related inpatient hospitalizations or AD-related outpatient contacts during the first 3 years of the study period (year –3 to year –1). Patients had a mean of 8.78 ± 7.79 AD-related outpatient contacts and 0.14 ± 0.47 AD-related inpatient hospitalizations during the first year after the index date (Table SIII), amounting to a cost of EUR 2,592 ± 122, corresponding to 53% of the healthcare costs for patients in the index year.
Patients with moderate-to-severe AD had a mean of 2.17 ± 5.42 and 2.77 ± 6.21 visits to a primary care dermatologist 3 and 2 years prior to their first AD-related hospital contact, respectively (Table SIII). For these patients, the number of visits to a primary care dermatologist increased to a mean of 6.54 ± 9.85 visits in the year prior to their first AD-related hospital contact. This amounted to a cost of EUR 221 ± 368, corresponding to 9% of the patients’ healthcare costs in the year prior to the index date, and explains 24% of the difference in total healthcare costs between patients and reference individuals in that year. In the period following the index date, patients’ frequency of visits to the primary care dermatologist decreased to an average of 1.3 ± 0.023 visits per year.
Effect on gross earnings
AD had a considerable effect on earnings, reducing them by EUR 1,331 per year, on average, vs reference individuals, in the 5 years following the index date equivalent to a 4.1% reduction and implying a lifetime earnings loss of EUR 42,789 (Appendix S2) for the average patient from age 18 years to retirement at age 65 years and a loss of EUR 214 million in total for the current (2018) prevalent population of 4,999 patients.
There was a non-significant difference in yearly earnings of EUR –27, EUR –177 and EUR –66 (p-values 0.40, 0.38 and 0.40, respectively) in the 3 years prior to the index date between patients and reference individuals (Table II and Fig. 2). The difference in gross earnings between patients and reference individuals increased from a mean of EUR –90 ± 456 in the years prior to the index date to EUR –1,331 ± 296 per year in the 5 years following the index date.
The probability of receiving disability insurance increased from 4.78% in the first year after the index date, to 7.12% 5 years after the index date, and the increase was 4.2 times larger than the corresponding increase for the matched reference individuals. The total productivity loss per patient attributable to AD was estimated to be EUR 8,256 (p = 0.0002) during the study period.
Table II. Gross earnings per year relative to index date, in Euro (EUR)
Fig. 2. Difference in gross earnings between patients with moderate-to-severe atopic dermatitis (AD) and their matched reference individuals in each year relative to the index date, in Euro (EUR).
Sensitivity and sub-group analysis
A sensitivity analysis with an inclusion criterion of at least 2 AD-related hospital contacts yielded comparable results to the main analysis. To explore whether the results were driven by a subset of individuals with high healthcare resource utilization, a sub-group of 422 patients with continuous AD contacts during the 4 years after the index date was identified. Compared with the main study population, the mean healthcare cost among this sub-population in the index year were 58% higher and remained higher in the following years (years 1–5) (Fig. S2). The attributable costs of AD among patients with continuous contacts was estimated as EUR 25,093 (p < 0.0001) during the study period, which is 132% higher compared with the attributable healthcare costs in the study population. In total, it was estimated that the total productivity loss per patient in the sub-population attributable to AD was EUR 46,823 (p < 0.0001) during the study period, which is a difference of 467% compared with the study population (Fig. S3).
This study documented a substantial economic burden of patients with presumed moderate-to-severe AD in Denmark.
The calculated prevalence from this analysis of moderate-to-severe AD diagnosed in adulthood in Denmark was at least 108 per 100,000 persons, with a large geographical variance of high prevalence in urban areas and low prevalence in rural areas. This may be explained by reduced access to tertiary care in specific rural areas (e.g. Northern Jutland) in the study period. Hence, patients with moderate-to-severe AD may have received treatment from a secondary care dermatologist instead, and thus were not included in the study population.
The cost-of-illness analysis showed that patients had significantly higher individual healthcare costs than reference individuals in the study period. Management and treatment of patients with moderate-to-severe AD in Denmark is associated with an attributable yearly cost of AD to the healthcare sector of EUR 5.6 million (Appendix S11). This is well illustrated by the average patient in this sample having the first AD-related hospital contact at age 35 years, and imposing attributable healthcare costs of nearly EUR 55,400 during adulthood, from 18–65 years of age. The results indicate that the individual healthcare costs associated with moderate-to-severe AD in Denmark are similar to psoriasis (22) and the individual direct cost attributable to AD is 96% higher than that of asthma (23).
In the 3 years prior to the index date, patients, on average, had more than 11 visits to their primary care dermatologist, and more than 6 of these took place in the year prior to the index date, indicating treatment failure with the primary care dermatologist. The results suggest that shifting treatment for these patients from the primary care dermatologist to the hospital would significantly reduce the patients’ need for consultations, as the total number of AD contacts, i.e. in hospital and in the primary sector, decreased after the index date. A recent Danish register study (24) also found a higher number of visits to the primary care dermatologist in the year prior to the index date, but a lower mean number of visits, as the study population included mild, moderate, and severe AD in both children and adults. That study (24) highlights considerable differences in treatment patterns between primary and secondary care and the hospital. The reduced number of AD contacts after the index date in the current study supports that finding.
The results of this study indicate that the patients saw reductions in gross earnings after their first AD-related hospital diagnosis, as the difference in gross earnings between patients and reference individuals increased from the years prior to the index date to the 5 years of follow-up. This may be explained by high disease burden despite treatment, and, to a degree, that it affects productivity, increases sick leave, etc.
Similar to an earlier Danish study, the current study showed that patients with moderate-to-severe AD are more likely to receive disability insurance (7). It was shown that 2.3%-point more patients with moderate-to-severe AD received disability insurance 5 years after their first AD-related hospital contact, implying an additional societal attributable cost of EUR 106.4 million in the period from the index date until retirement.
Strengths and limitations
The strengths of this study included its retrospective register-based design, including all patients with a hospital-registered diagnosis of AD registered in the period from 1997 to 2018. The ICD-10 code of AD in the Danish National Patient Register was validated in a recent study by Andersen et al. (25). The large study population reduced the risk of random variation in the study’s cost estimates.
In the current study, indirect costs were limited to lost productivity; however, the cost associated with social benefits attributable to the disease should also be taken into consideration in the assessment of the total cost and expenses to society, which herein may imply an underestimation of the indirect costs. Conversely, using Danish registers, only patients with hospital-seeking behaviour are identified, which may imply an overestimation of the total costs. The true prevalent moderate-to-severe AD population could not be identified via the registers. This means that caution should be taken before extrapolating results beyond the included population. It was not known whether reference individuals had mild AD. This was an inherent uncertainty given the study methodology, which presumably resulted in slightly underestimated cost differences between patients and reference individuals. Patients with an AD diagnosis before the age of 18 years were excluded from this study. The consequences of this on the cost estimates are unclear. Full 9-year follow-up was possible only for patients and controls with an index date before 2014. The study relied on costs collected for other purposes, and costs such as the cost of short-term sick leave, transportation time related to consultations, and informal care provided by friends and family were not included, as this data is not available in the registries. Information on non-prescription treatment, including special types of emollients, are not captured in Danish registers. Hence, the use and costs of these are not included herein.
Using Danish registers, it was only possible to identify the date of first hospital contact regarding AD. This was used as the index date, although it was unlikely that this date reflected the incidence of the disease. This was mitigated by ascribing the difference in direct and indirect costs between patients and reference individuals prior to the index date to the patients’ AD.
Conclusion
Moderate-to-severe AD among adults was associated with substantial economic burden, highlighting an unmet need with regard to better management and treatment of patients with moderate-to-severe AD.
The authors thank Jens Olsen from Incentive for his valuable comments and suggestions throughout the research and writing of this paper. The study was funded by LEO Pharma Nordic.
Conflicts of interest. AWB and DJT are employees of LEO Pharma. MHP and MEM are employees of Incentive, which is a paid vendor of LEO Pharma. JPT and CV did not receive any funding from LEO Pharma to conduct this study. JPT has been an investigator, speaker, and/or consultant for Almirall S.A.; AbbVie A/S, Galderma Nordic AB, Pfizer ApS, Pfizer Ltd., LEO Pharma A/S, Sanofi-Aventis Denmark A/S, Sanofi A/S, Genzyme Europe B.V., Eli Lilly Denmark A/S. CV has acted as a speaker and/or consultant for Sanofi A/S, Eli Lilly Denmark A/S, Novartis Healthcare A/S, Janssen-Cilag A/S, LEO Pharma A/S, AstraZeneca A/S, Eli Lilly & Co Ltd.
 Appendix S1 Appendix S2 Table SI Table SII Table SIII Table SIV Figure S1 Figure S2 Figure S3
Appendix S1 Appendix S2 Table SI Table SII Table SIII Table SIV Figure S1 Figure S2 Figure S3

 Click to show fullsize
Click to show fullsize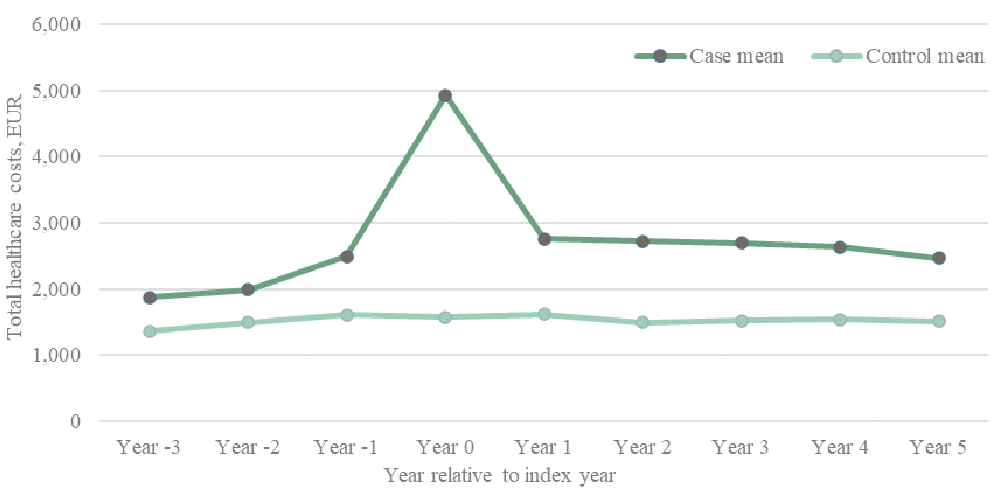 Click to show fullsize
Click to show fullsize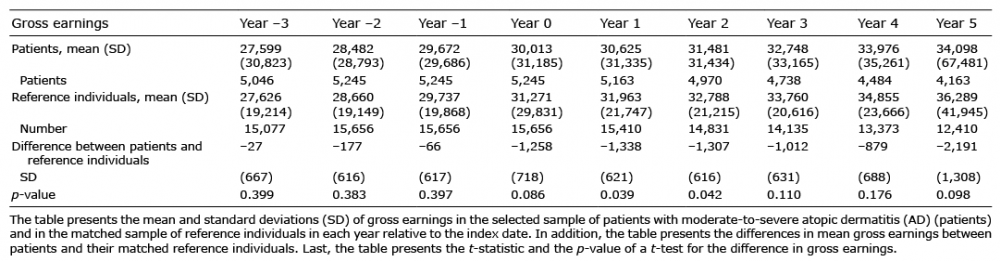 Click to show fullsize
Click to show fullsize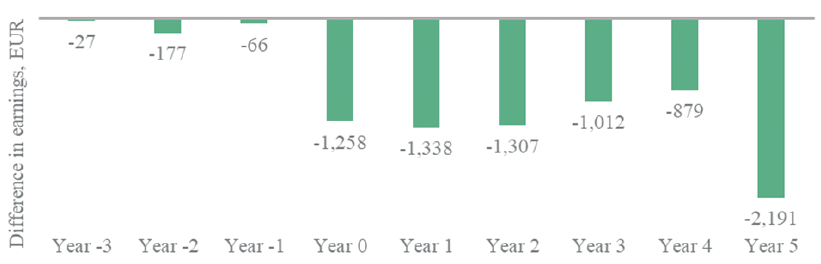 Click to show fullsize
Click to show fullsize