


Department of Clinical Sciences Lund, Dermatology and Venereology, Lund University, Lund Sweden and Skåne University Hospital, Lund, Sweden
Prurigo simplex or “itchy red bump” disease is a controversial pruritic papular eruption. The objective of this study was to delineate the diagnostic criteria for this disease. A PubMed search was performed for: “prurigo simplex”, “prurigo simplex subacuta”, “subacute prurigo”, “chronic papular dermatitis in adults” and “itchy red bump disease”. Medical charts of patients with prurigo diagnoses in a university setting were analysed. The literature search revealed 32 relevant studies (431 patients) on different aspects of the disease. Out of 50 patients with prurigo diagnoses, 5 patients (4 women, mean age at onset 54 years) matched the description in literature. Small, severely itchy papules without secondary skin lesions continued to appear for years (mean 5.6 years). Skin biopsies revealed lymphocytic perivascular infiltrates, few eosinophils and occasionally spongiosis. Treatment with long-term methotrexate or cyclosporine cleared the symptoms. Some major and minor diagnostic criteria for prurigo simplex are proposed and compared with chronic prurigo.
Key words: prurigo simplex; itchy red bump disease; chronic prurigo; pruritus; itch; immunosuppressants.
Accepted Aug 25, 2021; Epub ahead of print Aug 26, 2021
Acta Derm Venereol 2021; 101: adv00539.
doi: 10.2340/00015555-3912
Corr: Joanna Wallengren, Department of Dermatology and Venereology, Lund University, Skåne University Hospital, SE-221 85 Lund, Sweden. E-mail: Joanna.Wallengren@med.lu.se
Many skin diseases are characterized by small, itchy, dome-shaped lesions. Classification of these disorders is essential for their treatment. This study focuses on patients with extremely itchy, tiny elevations with blistering on top. These skin lesions have a chronic course and have a negative impact on quality of life. The literature review and patients presented in this study suggest that this disorder belongs to the prurigo (intensely itchy spots) group of diseases and should benefit from guidelines on management of prurigo. High-dose immunosuppressants clear the symptoms, but there is an unmet need for novel therapies to combat the intense itch.
The term prurigo, originating from the Latin prurire (to itch), is a condition of itching papules. Prurigo was a common disease in the 19th and 20th centuries, and a great number of scientific descriptions, bearing names of leading dermatologists, were published. A detailed review of the literature in 1962, a “conceptual chaos” according to its author, resulted in a rough classification of prurigo variants into acute, subacute and chronic forms (1).
Acute prurigo (strophulus), common in regions of poor sanitary conditions, is associated with insect stings or infestations (1, 2). Chronic prurigo, on the other hand, is triggered by endogenic factors causing itch (3). The main criteria for chronic prurigo have recently been consented to the presence of chronic pruritus for ≥ 6 weeks, a history or signs of repeated scratching and multiple localized or generalized pruriginous skin lesions (3). Chronic prurigo may present as papules, nodules (flat/topped or umbilicated), plaques or linear skin lesions, considered secondary to scratching (3).
Subacute prurigo, characterized by small papulo-vesicles, is the most controversial category of prurigo (1, 4). Besides many eponyms, it is also known as prurigo simplex, prurigo simplex subacuta or urticaria papulosa chronica perstans (1, 2). Lately, the classification of prurigo into acute, subacute and chronic forms has been questioned (5). It is discussed whether subacute prurigo (prurigo simplex) belongs to the prurigo group of diseases, or if it is just one of many papular eruptions. In American literature, it is better known as “itchy red bump” disease. The term was coined by Ackerman (6), who described it as a “maddeningly pruritic, persistent condition that clinically resembles dermatitis herpetiformis with histologic features similar to papular urticaria”.
Another controversial issue is whether prurigo simplex or “itchy red bump” disease is a clearly defined entity or a variant of chronic prurigo. It has been suggested that it is a transitional stage of prurigo that transforms from an acute to a chronic form (7).
The objective of this study was to search the literature for case reports and relevant theories, as well as to analyse patients with presumed prurigo simplex at a university dermatology department to further delineate this condition and explore its relation to chronic prurigo.
Literature search
A PubMed search was performed in January 2021 using the following search terms: “prurigo simplex”, “prurigo simplex subacute”, “subacute prurigo”, “papular dermatitis in adults” and “itchy red bump disease”. Publications on conditions of papular dermatoses secondary to external triggers, internal endocrine factors or malignancy were excluded.
Patients
According to the International Classification of Diseases 10th revision (ICD-10), Prurigo nodularis (L28.1) and Other prurigo (L28.2) were included in the search of the patient database of the Department of Dermatology, Skane University Hospital in Lund, who visited the centre for the last 10 years. Patients with nodular, papular, papulovesicular or coalescing (plaques) prurigo lesions of duration > 6 weeks were selected and invited by post to participate in the European Prurigo Project (8). Medical charts and histopathology of 50 patients, who agreed to participate in the project, were analysed with regard to the description of prurigo simplex in the literature. The study was reviewed and approved by the local Ethics committee, Lund University (number 2017/677) and a written consent form was obtained from all patients.
Literature search
In total, 170 publications with search terms: prurigo simplex (n = 81), prurigo simplex subacuta (n = 15), subacute prurigo (n = 36), chronic papular dermatitis in adults (n = 50) and itchy red bump disease (n = 3), respectively were tracked. Several publications appeared under more than 1 search term. Thirty-two publications (4 reviews) met the inclusion criteria. A total of 431 patients were enrolled in the clinical studies, selected parameters of the disease being reported.
Morphology of skin lesions
Summarizing descriptions of a prurigo simplex lesion, Kogoj found a 2–5-mm erythematous, hard, round, dome-shaped papule with a vesicle on top; a “seropapule” (1). This is exactly the definition of a prurigo papule, coined by Willan in 1798 and referred by Kocksard (4).
Most frequently, the skin lesions presented at doctors’ visits were papules with no vesicular element, but often with excoriations, as in 26 patients reported by Ollech (9) and 28 patients reported by Uehara & Ofuji (10). Multiple flesh-coloured to erythematous non-follicular papules with superimposed excoriations or lichenification were described in 12 patients (11). The pruritic papules were mostly confined to the neck, behind the ears, trunk, extremities or buttocks (9, 11).
There are 2 reports on papular eruption on the trunk and upper extremities in 7 black men and 20 Korean men (12, 13). The lesions were characterized by recurrent, severely pruritic, non-follicular, monomorphic, erythematous urticarial papules. There was no evidence of insect stings, atopy or other pruritic erythematous papular dermatosis, and the authors considered the condition a variant of prurigo (12, 13).
Two other reports from Japan deal with 6 patients with “grouping prurigo” (14). The patients presented with localized 3–4-mm papular eruptions that were either persistent or recurrent in summertime (14).
Histopathology of skin lesions
Original descriptions of prurigo simplex underline the occurrence of an intraepidermal sero-haemorrhagic vesicle, or crust and infiltration of lymphocytes, with a few histiocytes and eosinophils in the papillary dermis (1). Histological features common to all cases described in the current study include a mixed superficial and deep perivascular infiltrate of mononuclear cells with scattered interstitial eosinophils (9, 10, 12–15). According to Gamblicher et al. (15), the inflammatory cell infiltrates observed in prurigo simplex appear to be different from those found in eczematous skin changes, e.g. atopic dermatitis (AD). In some reports, the histological changes were found in connection with hair follicles, while others did not observe predominant follicular involvement (10, 11). In some reports spongiosis was found (10, 11, 15).
In a neurohistological study on 16 patients with prurigo simplex, Tritsch & Kantner (16) described richly innervated epidermis in unscratched papules and damaged nerve fibres due to scratching in the excoriated papules. They found proliferation of subepidermal nerve fibres that penetrate epidermis in the healing phase of erosions (16). The authors concluded that these findings are common in itching conditions and are not specific for prurigo simplex.
Differential diagnoses
Prurigo simplex may be clinically confused with many papular dermatoses, such as AD, contact dermatitis, urticaria, infestations, and different bullous diseases, such as dermatitis herpetiformis, pityriasis lichenoides et varioliformis acuta or transient acantholytic dermatosis (11).
Other conditions with excoriations to be differentiated from prurigo are neurotic excoriations, which display no papules and acne excoriée, where comedones are present. Histopathology is diagnostic in such cases. Ollech et al. (9) presented a diagnostic algorithm for the evaluation of chronic pruritic papular eruption.
There are some reports of prurigo simplex associated with bullous diseases: a case of “subacute prurigo-like linear IgA disease” and 2 cases of bullous pemphigoid mimicking prurigo simplex (17–19). In all cases, direct immunofluorescence was positive. These entities belong to the spectrum of bullous diseases and not primarily to the prurigo group. Immunofluorescence assays in patients affected by long-lasting pruriginous dermatoses are recommended to exclude autoimmune bullous dermatoses.
Comorbidities
Atopy diagnosed by a history of atopic respiratory or skin disease, or alternatively by positive prick-tests, has been described in several reports on prurigo simplex (11, 15, 20–22). The most commonly observed internal disease was diabetes (7, 15, 22). Hypertension and renal disease were also mentioned (15). Seikowski & Frank (23) examined 70 diagnosed patients using psychological tests. One-third of the patients reported psychosomatic complaints, and one-third reported severe psychosocial risk factors, mostly in terms of critical life events (23).
Therapy
As antihistamines and topical steroids are often insufficient, patients require systemic treatment, which often starts with courses of systemic steroids (9, 12, 13). However, the problem tends to recur as soon as the medication is stopped (12).
The second line of treatment seems to be phototherapy. A comparative study on courses of ultraviolet B (UVB) alone, ultraviolet A (UVA)/UVB and psoralen ultraviolet A (PUVA) showed that, although patients in all groups relapsed with time, the PUVA-treated patients had the best response rate (24). PUVA and UVA1 were reported as superior to UVB-narrow band in the management of prurigo simplex (25). Also, bath PUVA was reported to be effective (26, 27).
In a retrospective study, Moustafa et al. (28) identified 14 prurigo simplex patients on systemic medication during a 10-year period. The median duration of treatment was 25 months. Methotrexate was used first line in 12 patients, with control of disease achieved in 8 patients with a dose between 2.5 and 10 mg weekly. Azathioprine and mycophenolate mofetil provided control of the disease when used as first-line therapy in the remaining 2 patients. While azathioprine was effective in patients who failed methotrexate, gastrointestinal side-effects limited its long term use (28).
Cyclosporine at a dose of 4 mg/day for 7 years was effective in a patient with very severe prurigo simplex who failed several other treatments (29). Significant improvement was also reported in 4 of 5 patients with severe prurigo simplex treated with daily intravenous recombinant interferon gamma for 7–60 days (30).
A psychological approach in combination with medical treatment was suggested by Seikowski & Frank (23).
Pathogenesis and distinction from papular atopic dermatitis, acute and chronic prurigo
Sometimes, the patients described here may be primarily diagnosed with refractory AD due to papular or follicular eruption (11). Sherertz et al. (11) investigated 12 such patients, with careful history-taking regarding criteria for AD, skin biopsies, immunofluorescence studies, food challenges and patch testing. The authors concluded that the patients are not atopic by strict criteria, but that “the clinical and histological presentation bridges the description of prurigo simplex subacuta and papular variant of atopic dermatitis” (11).
Although acute prurigo (strophulus) and prurigo simplex share common morphology (the sero-papule) Kogoj emphasized 2 differences (1). The seropapule is the primary lesion in prurigo simplex, while it is preceded by a weal in strophulus (1). Secondly, prurigo simplex has a continuous course, while strophulus is recurrent (1).
Prurigo simplex and chronic prurigo are considered separate entities, but some authors are of the opinion that transitional stages between them are common (7). The main argument for this hypothesis, according to Greither, is that the conditions share the same aetiology, including metabolic and endocrinological disorders, as well as atopy (7).
On the other hand, Pereira & Ständer (5) emphasize demarcation between prurigo simplex and chronic prurigo. The main argument for this statement is differences in the aetiopathogenesis and morphology of skin lesions (5). While papules and papulo-vesicles of prurigo simplex are primary skin lesions, the lesions of chronic prurigo are secondary to scratching. This theory is in accordance with that of Kocsard, who goes even further: “In prurigo simplex subacuta, the clinical picture is monomorphic, showing only prurigo papules in various stages of development. In pruriginous dermatoses, on the other hand, the prurigo papules appear in combination with other skin manifestations such as lichenification, eczematization and in the case of prurigo nodularis-nodules” (4).
Patients
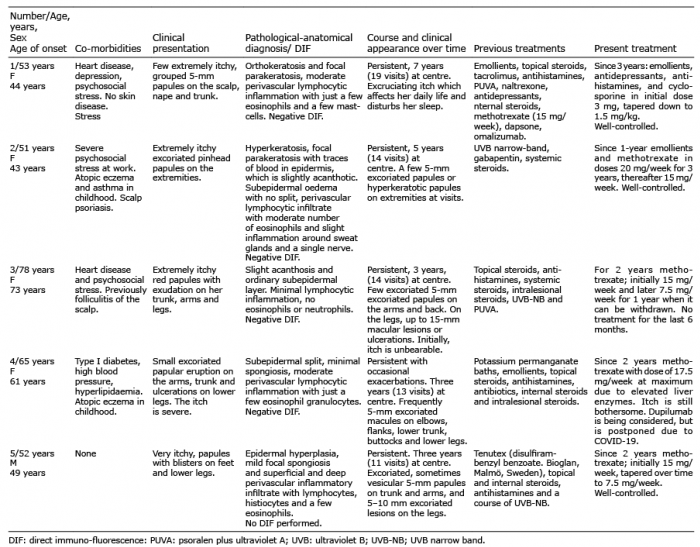
Fifty patients with diagnoses of Prurigo nodularis (L28.1) and Other prurigo (L28.2) with a duration of more than 6 weeks agreed to participate in the study. The patients presented with pruriginous nodules or papules. Details concerning the age, sex, comorbidities of the patients and treatments given are shown in Table SI.
Out of the 50 prurigo patients, 5 patients (4 women, mean age at onset 54 years) presented with clusters of small, intensely itchy papules suggesting prurigo simplex. Two other patients (a woman aged 60 years and a man aged 71 years) were considered for the study, but excluded due to incomplete data. Details of the 5 patients included in the present study are summarized in Table I. Patients presented here could tell quite exactly the day or week when the first rash occurred and the severe itch started. Although skin lesions popped up and disappeared, the course of disease was persistent, and in one patient exacerbations occurred (case 4). The mean duration of disease in this case series was 5.6 years, and only one patient could stop medication during this period.
Table I. Data on 5 patients with prurigo simplex
Patients often described small papules or papulo-vesicles as a first sign. On examination the papules were often excoriated (Fig. 1). Throughout the observation period, the patients presented with the same type of papules, but on some occasions, skin lesions were scattered and more widespread (Fig. 2). No lichenification, hyperkeratosis or nodules were noticed, and no scratch lesions were seen on non-lesional skin. Itch seemed localized to the lesional skin.
Fig. 1. Prurigo simplex. Tiny excoriated papules on the flank of case 4, treated with methotrexate 10 mg/week.
Fig. 2. Prurigo simplex. Erythematous papules and papulo-vesicles on the upper arm of case 5 before systemic treatment.
The histological findings from lesions showed lymphocytic perivascular infiltrates, few eosinophils and sometimes spongiosis, while diagnosis of eczema was excluded. Direct immune-fluorescence from perilesional skin, performed in cases 1–4, was negative, excluding bullous disease. Systemic treatment with methotrexate and cyclosporine was monitored using laboratory tests at regular intervals.
According to Kogoj, “only dermatoses with a seropapel or prurigo knot should belong to the prurigo group of diseases” (1). Darier’s prurigo simplex, Lutz’s prurigo simplex subacuta and Kogoj’s prurigo subacuta all seem to fit the description of the condition described in present study (1, 31). Even if “prurigo simplex” and “chronic papular dermatitis in adults” were the most common keywords in the literature search of PubMed, “prurigo simplex subacuta,” “subacute prurigo” and “itchy red bump disease” selected relevant cases most accurately. Although some patients reported papulo-vesicles, mostly small papules were noticed at doctor’s visits. Patients in this study displayed only papular and no nodular lesions. There was no notice on transformation from prurigo simplex to nodular prurigo in the literature. The lesions developed suddenly, but had a chronic course. It is therefore hard to define the condition as subacute. “Prurigo simplex”, denoting the monomorphic lesion (prurigo papule) without a definition of the course of disease may therefore be a preferred term (32). In the ICD nomenclature, it can be classified as “other prurigo,” since there is no separate code for this entity.
Prurigo simplex has been reported worldwide in Caucasian, African-American and Asian patients of both sexes, and the case series presented here confirms the description in these reports.
Biopsy from lesional skin in this case series included lymphocytic perivascular infiltrates, few eosinophils and sometimes spongiosis. These findings are not precise, but histology is helpful to exclude other pruritic diseases (9). In all the cases in the current study, dermatopathologists considered eczema not likely. Our patients displayed this histopathological picture a long time after their first appearance, as the mean time for the first biopsy at the centre was 1.5 years after reported onset. Negative direct immunofluorescence, performed in all but 1 of the patients excluded bullous diseases, such as dermatitis herpetiformis or bullous pemphigoid.
The most striking feature in this case series was that so few tiny lesions could cause unbearable itch. All patients reported a negative impact on their daily lives, while 3 patients reported severe psychosocial stress for long periods.
Based on the cases described in the literature and on the 5 patients in the present case series, some major and minor diagnostic criteria of prurigo simplex are drafted in Table II. This hypothesis should be tested more directly in case series from other centres. It can then be discussed how many major or minor criteria are required for the diagnosis of prurigo simplex.
Table II. Proposal of major and minor diagnostic criteria for prurigo simplex
In agreement with other reports, all the current patients were, at some point in time, treated with UV therapy, but the condition relapsed after the UV course was completed (24–27). Only immunosuppressants could clear the symptoms. In this case series, relatively high doses of methotrexate were required, higher than those reported by others (28).
In the current study university setting, this entity constituted approximately 10% of all prurigo cases with a chronic course. A limitation is, however, that some cases meeting diagnostic criteria for prurigo simplex might have been missed being registered as toxicoderma, drug eruption or eczema instead.
In addition to differences in morphology and histopathology, there are some similarities between prurigo simplex and chronic prurigo (Table III). Notably, in both disorders, immunohistochemistry shows dermal proliferation of nerve fibres and damaged nerves in the epidermis (16, 33, 34). This pattern is also seen in other pruritic conditions, such as brachioradial pruritus (35).
Table III. Prurigo simplex vs chronic prurigo
Most importantly, the therapy used in chronic prurigo also seems to be effective in prurigo simplex (Table SI, and Tables I and III). Here, lessons can be learned from guidelines on chronic prurigo (36). The immunosuppressive treatment has to go on for years in both conditions. Consequently, it is important to switch therapy to medications with a good safety profile.
New drugs targeting specific receptors in the nervous system and in the immune system have proved effective as antipruritic therapies (37). Dupilumab, a human monoclonal antibody against interleukin IL-4Ra, common to IL-4 and IL-13 receptors, has been reported to clear symptoms in several case series of prurigo nodularis (37–39). It could also be tried in prurigo simplex, as increased expression of IL-4 and IL-31 was shown even here (40).
Nemolizumab, a humanized antihuman interleukin-31 receptor A monoclonal antibody, has proved promising in a phase II randomized, placebo-controlled trial on chronic prurigo (37, 41).
Interestingly, a special feature of prurigo simplex is the presence of eosinophils. Theoretically, eosinophil activity could be reduced using monoclonal antibodies against IL-5 or Janus kinase (JAK2 inhibitor), which blocks activation of IL-5 by intracellular mechanisms (42). Baricitinib (selective JAK1-and JAK2-inhibitor) could be tried here, as it was shown to significantly reduce pruritus in a phase II, double-blind, randomized trial on AD (37, 43). However, the effectiveness and safety of the novel medications has to be confirmed in larger studies.
In conclusion, the literature review and case series suggest that the disorder presented here belongs to the prurigo group of diseases. Based on the literature and on this case series, diagnostic criteria for prurigo simplex and a comparison with chronic prurigo are suggested. Future investigations that test these hypotheses more directly in patients from other centres or in a multicentre study are warranted. A consensus on the definition and classification would greatly facilitate further research on the pathogenesis and therapy of this burdensome disease.
A research grant from the Edvard Welander Foundation/Hudfonden is gratefully acknowledged.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize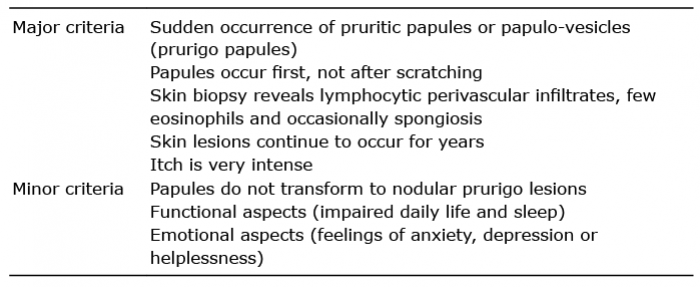 Click to show fullsize
Click to show fullsize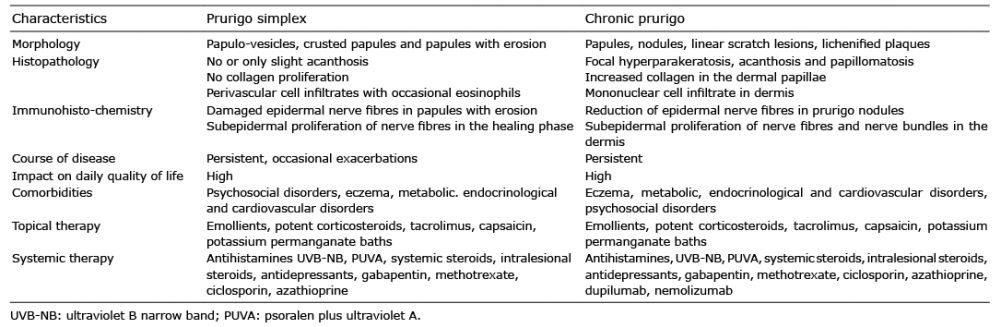 Click to show fullsize
Click to show fullsize